
記住我







The prevalence of chronic heart failure with reduced ejection fraction (HFrEF) is increasing worldwide, in part due to medical, surgical, and device therapies, which reduce mortality. Thus, there is a huge need for novel therapies to further increase cardiac contractility and improve symptoms.
Electric stimulation of tissues has been applied to promote remodeling, regeneration, and repair in the treatment of bone fractures, spinal cord injuries, and wound healing. Furthermore, electrical stimulation with a dedicated microcurrent was associated with significant improvement of left ventricular ejection fraction (LVEF) in animal models of chronic HF.1–5 A novel implantable device has been developed to apply microintensity electrical current directly to the human heart (C-MIC System, BerlinHeals GmbH, Berlin, Germany). C-MIC consists of a transvenous right ventricular (RV) lead similar to a single-coil defibrillator lead, an epicardial LV patch lead with a large electrically active surface and a fully implantable power generator. The device applies an electrical microcurrent through the LV patch directly to the epicardial surface of the heart, and the endocardial RV lead serves as a counter electrode. In contrast to traditional pacemakers or implantable cardiac contractility modulators, the C-MIC System generates a continuous direct transmyocardia microcurrent (DC current) in the μ-ampere range, which is applied independently from electrical or mechanical cardiac activity. Parameters are set at implantation and can be modified via a portable wireless user terminal.
Case ReportA 79-year-old man who suffered from advanced HFrEF due to dilated cardiomyopathy was referred to our center. He had experienced multiple hospital admissions for worsening HF symptoms in the past and presented with NYHA class III. Thirteen years before, he had undergone aortic valve replacement and implantation of a dual-chamber pacemaker for atrioventricular block. Further comorbidities were hypertension, type 2b diabetes mellitus, stage 2 chronic kidney disease, history of pulmonary embolism, and adenocarcinoma of the lung with brain metastases treated with surgery and radiotherapy. Echocardiography revealed a dilated LV with diffuse hypokinesia and a LVEF of 30%, preserved RV function and a competent aortic bioprosthesis. Computed tomography showed a centrilobular emphysema without signs of recurrent neoplasia or lymphadenopathy. The interdisciplinary Heart Team judged the patient not suitable for CRT-D therapy due to a narrow QRS complex and absence of left bundle branch block, nor for durable mechanical circulatory support or heart transplantation. Notwithstanding, due to significantly impaired quality of life, compassionate use of the C-MIC System was offered and discussed with the patient, who gave informed consent to the procedure.
Implantation was conducted under general anesthesia with a minimally invasive surgical approach. A left anterolateral thoracotomy was performed at the fifth intercostal space above the cardiac apex. The LV free wall was dissected from adhesions, and the LV patch lead was positioned on the LV epicardial surface and fixated with 4-0 polypropylene sutures (Figure 1A). A 5 cm incision was performed at the level of the left infraclavicular fossa, and the LV lead was tunneled subcutaneously from the left pleural cavity to the new prepectoral pocket (Figure 1B). The left subclavian vein was punctured, and the RV lead implanted in the RV cavity under fluoroscopic guidance (Video, Supplemental Digital Content 1, https://links.lww.com/ASAIO/A691). Both LV and RV leads were connected to the C-MIC generator (Figure 1C), which was finally implanted in the prepectoral pocket. Wounds were closed (Figure 1D), and correct position of the device and leads was confirmed by fluoroscopy (Figure 2). The patient tolerated the procedure well, with minimal blood loss and no complications. The patient was extubated in the operation room and transferred to the normal ward for monitoring. The postoperative course was uneventful, with regular mobilization and stable clinical parameters (Table 1). A postoperative computed tomography scan showed a correct position of the device and both LV and RV leads (Figure 2B). After drain removal, oral anticoagulation with phenprocoumon was started, with a target international normalized ratio of 2.0–3.0 due to previous pulmonary embolism and repeated episodes of deep vein thrombosis. The patient’s clinical status was monitored in-hospital for the following 10 days. The C-MIC device continuously operated without malfunction, and no electrical interference between devices was observed during hospitalization and at 30-day follow-up. Table 1 shows the patient’s vital signs, laboratory data, and echocardiographic results from preimplant to 30 days after surgery. Echocardiography showed a LVEF of 40% (Video, Supplemental Digital Content 1, https://links.lww.com/ASAIO/A691) at 30 days follow-up.
Table 1. - Patient’s Vital Signs, Laboratory, and Echocardiography Data Variables Preimplant Discharge 30 days Vital signs Heart rate, beats/min 57 80 55 Systolic blood pressure, mm Hg 141 140 113 Diastolic blood pressure, mm Hg 53 83 53 Echocardiogram LVEF, % 30 35 40 LVEDD, mm 6.63 6.45 6.6 LVESD, mm 5.37 5.56 5.34 PAPs, mm Hg 32 28 Laboratory data White blood cells, x1,000/mL 13.5 10.6 9.0 Hemoglobin, g/dL 12.6 11.3 9.9 Platelets, x1,000/mL 176 179 230 AST, U/L 29 n.a. 21 ALT, U/L 31 n.a. 12 Creatinine, μmol/L 134 175 142 CK, U/L 24 37 31 NT-proBNP, pg/mL 4,805 n.a. 4,529ALT, alanine aminotransferase; AST, aspartate aminotransferase; CK, creatine kinase; LVEF, left ventricular ejection fraction; LVEDD, left ventricular end diastolic diameter; LVESD, left ventricular end systolic diameter; n.a., not available; NT-proBNP, N-terminal pro-B-type natriuretic peptide.
 Figure 1.:
Figure 1.: Implantation of the C-MIC device: A: exposure of the left ventricular wall through left thoracotomy and positioning of the epicardial left ventricular patch; B: tunneling of the left ventricular lead until exit at the preclavicular space; C: connection of right and left ventricular leads to the implantable microcurrent device; D: final result after wound closure. C-MIC, cardiac electrical microcurrent.
 Figure 2.:
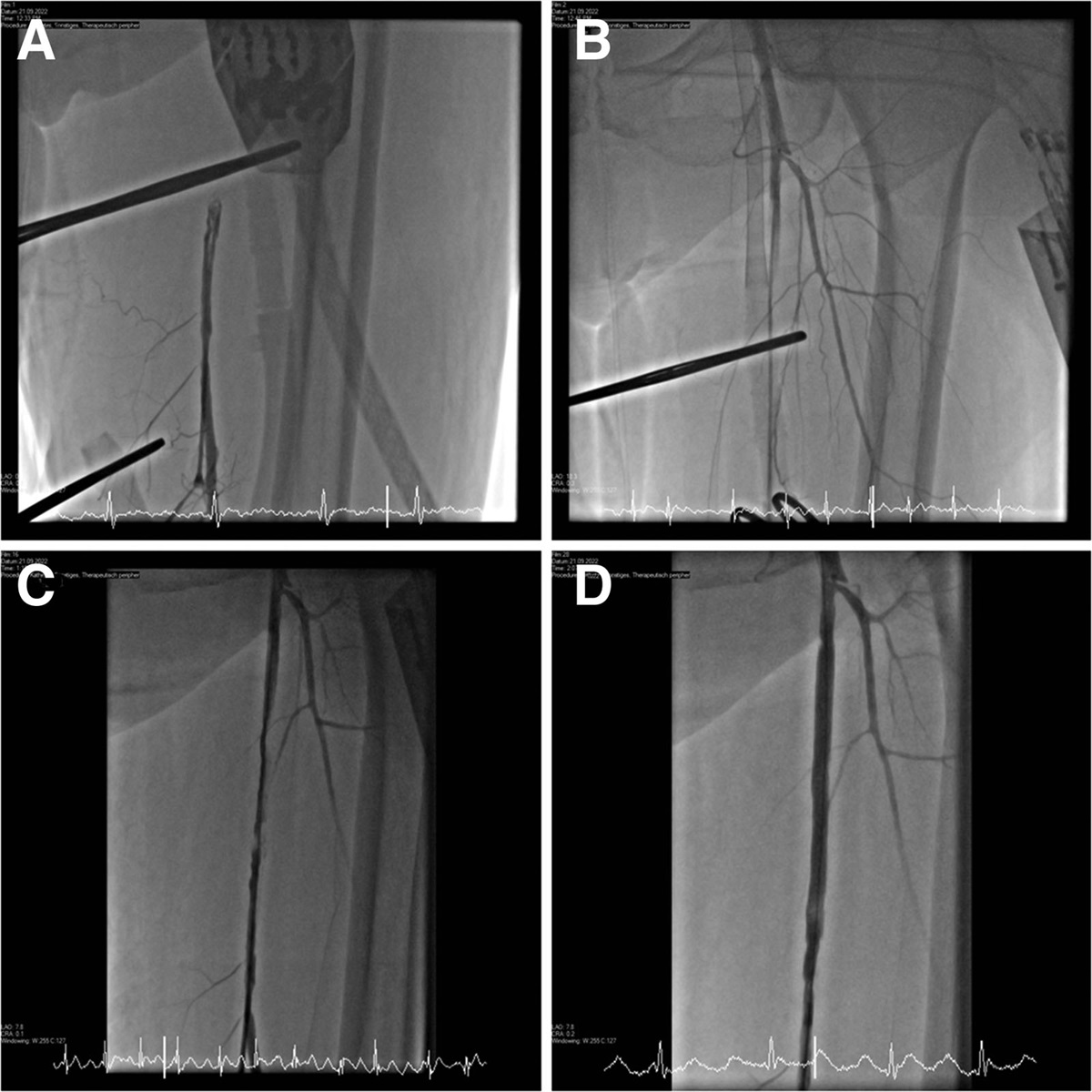
Figure 2.: A: angiographic view of the implanted device. B: postoperative computed tomography scan, coronal oblique maximum intensity projection.
DiscussionHerein, we report on the first-in-man implantation of the C-MIC System, a novel fully implantable device for cardiac electrical microcurrent application in HF. Different forms of microcurrent are currently used for several physical and regenerative therapies to promote tissue healing and injury repair.6 Indeed, the application of electric currents in the μ-ampere range can substantially change cell metabolism, being similar to electric currents generated by human tissues.6 Preclinical animal experiments demonstrated that continuous microcurrent applied to the failing heart over several weeks promotes reverse myocardial remodeling with direct effects on extracellular matrix and local proinflammatory signals.1,7 Moreover, electrical potential gradients are deeply involved in the regulation of interstitial edema, which can significantly compromise heart function in acute and chronic scenarios.8 Consequently, the application of cardiac microcurrent may generate positive effects on failing hearts through a rapid effect on tissue edema and an anti-inflammatory effect, which develops over time. In our own preclinical experience, C-MIC therapy applied over several weeks was associated with an improvement of LVEF in a sheep model of ischemic HF,4 suggesting that further remodeling can be expected even after the 30-day follow-up time. Moreover, preliminary data on the use of microcurrent stimulation in hearts suffering from ischemia-reperfusion injury after prolonged cardiopulmonary bypass demonstrated the feasibility and potential benefits of microcurrent therapy also in acute settings.3
Despite the promising preclinical results of microintensity electrical current application to failing hearts, a delivery system for human use was still not available until now. Observations from this first clinical experience demonstrate that the implantation of the C-MIC device can be performed using a minimal-invasive surgical technique. Adverse effects on the cardiovascular system as well as on other organ functions were not observed. Although this first-in-man use and preclinical data indicate possible improvements of systolic cardiac function, a prospective study is required to assess C-MIC efficacy in HFrEF patiens with persisting symptoms with optimal therapy. The C-MIC device is currently under investigation for clinical use within the first pilot study including 10 patients with nonischemic dilated cardiomyopathy.9
References 1. Macfelda K, Kapeller B, Holly A, et al.: Bioelectrical signals improve cardiac function and modify gene expression of extracellular matrix components. ESC Heart Fail. 4: 291–300, 2017. 2. Schmitto JD, Coskun KO, Coskun ST, et al.: Hemodynamic changes in a model of chronic heart failure induced by multiple sequential coronary microembolization in sheep. Artif Organs. 33: 947–952, 2009. 3. Mariani S, Napp LC, Meyer T, et al.: Animal model of cardiac reperfusion injury to evaluate the effects of electrical microcurrent application: preliminary results. J Heart Lung Transplant. 39:S361, 2020. 4. Napp LC, Baum C, Dogan G, et al.: Improvement of left ventricular ejection fraction by a novel electrical microcurrent therapy in a sheep model of chronic heart failure. J Heart Lung Transplant. 38: S259, 2019. 5. Ahadian S, Ostrovidov S, Hosseini V, et al.: Electrical stimulation as a biomimicry tool for regulating muscle cell behavior. Organogenesis. 9: 87–92, 2013. 6. Naclerio F, Seijo M, Karsten B, et al.: Effectiveness of combining microcurrent with resistance training in trained males. Eur J Appl Physiol. 119: 2641–2653, 2019. 7. Kapeller B, Mueller J, Losert U, Podesser BK, Macfelda K: Microcurrent stimulation promotes reverse remodelling in cardiomyocytes. ESC Heart Fail. 3: 122–130, 2016. 8. Ciutac AM, Dawson D: The role of inflammation in stress cardiomyopathy. Trends Cardiovasc Med. 31: 225–230, 2021. 9. Kosevic D, Wiedemann D, Vukovic P, et al.: Cardio-microcurrent device for chronic heart failure: first-in-human clinical study. ESC Heart Fail. 8: 962–970, 2021.
留言 (0)