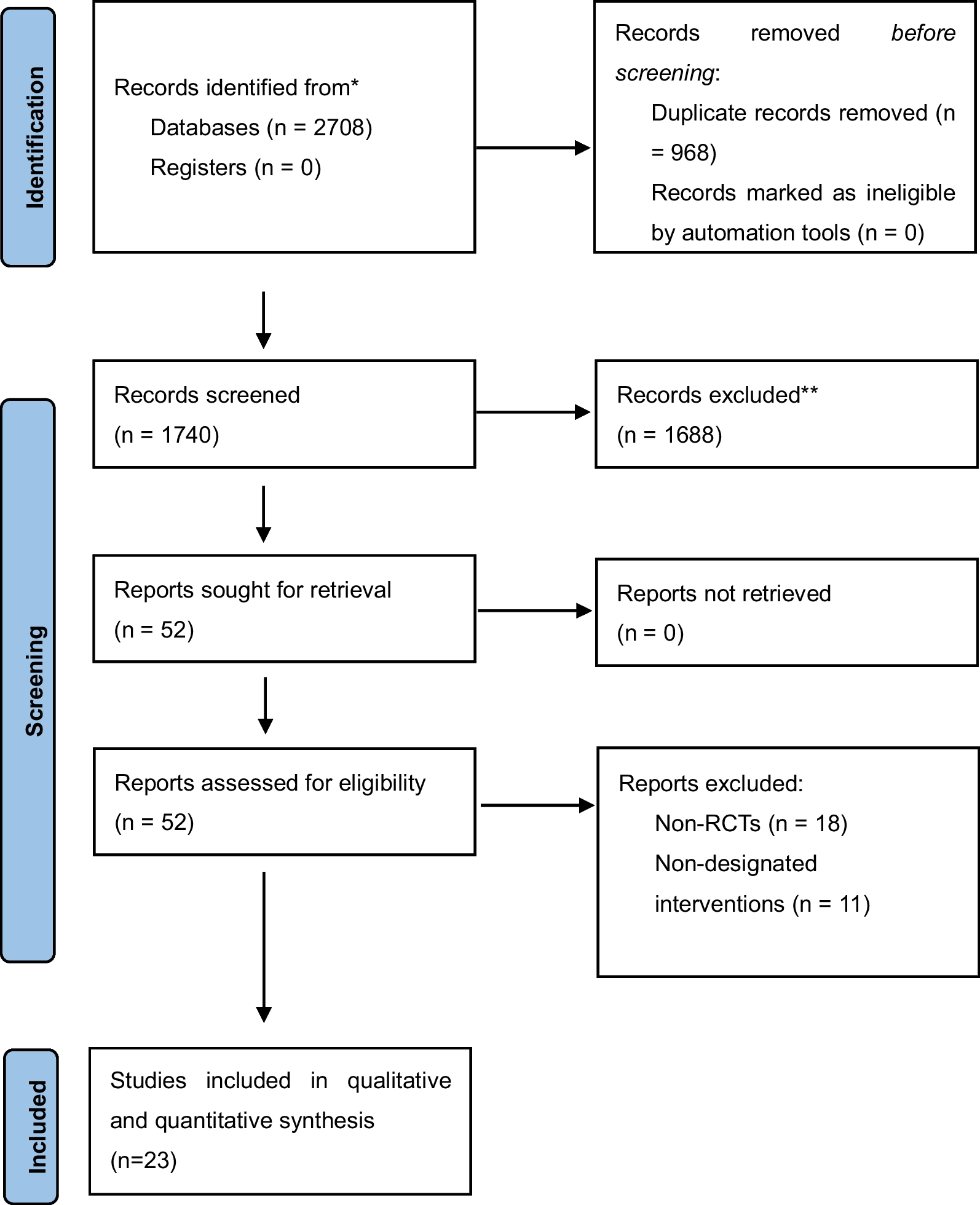
Below, the CQs and their recommendations are described for the five adult areas and the pediatric area. Please refer to Additional files 1, 2, 3, 4, 5, 6 for the search strategies, flow diagram, risk of bias summaries, forest plot, EP and EtD of each CQ.
I. Area A: Diagnosis/severity of illness evaluation/type evaluation
CQ1: Should ARDS diagnoses be conducted for patients with acute respiratory failure?Background
ARDS is a serious and urgent pathological condition that causes acute respiratory failure. Its diagnosis can affect the understanding of these pathological conditions, severity of illness evaluation, and treatment policy, and whether to confirm the diagnosis of ARDS is an important clinical question.
Recommendation
We recommend that ARDS should be suspected for patients with acute respiratory failure (GPS).
Supplementary item
Not only is the diagnosis of ARDS important for improving prognosis but also the diagnosis and treatment of diseases that causes ARDS.
Rationale
Summary of evidence:
There are no clinical studies that compare whether confirming or not confirming ARDS in a patient with acute respiratory failure directly improves patient outcomes. When ARDS is diagnosed, there is a possibility that the prognosis improves as a result of conducting the evidence-based recommendations presented in this guideline.
Balance of effects, acceptability, and feasibility determination:
The diagnosis of ARDS enables important clinical decision-making, such as understanding the pathological condition, evaluating illness severity, and deciding on a treatment policy; furthermore, there is a possibility that the prognosis improves as a result of conducting evidence-based recommendations presented in this guideline. Therefore, there are large benefits in ARDS diagnosis in patients with acute respiratory failure. ARDS diagnosis is based on the Berlin Definition proposed in 2012. The minimum requirements for the diagnostic items in addition to medical history and physical findings are chest imaging tests (simple chest X-rays, chest CT) and arterial blood gas analysis; the harm to patients and additional costs to medical institutions as a result of these actions are thought to be trivial.
CQ2: Should blood brain natriuretic peptide (BNP) and NT-proBNP levels be used for identifying cardiogenic pulmonary edema as the causative disease of acute respiratory failure?Background
Identifying cardiogenic pulmonary edema is important in ARDS clinical practice. Blood BNP and NT-proBNP levels are widely used as a supplementary diagnosis for heart failure, and whether to use these for identifying the causative disease of acute respiratory failure is an important clinical question.
Recommendation
We suggest using blood BNP or NT-proBNP levels for identifying cardiogenic pulmonary edema in patients with acute respiratory failure (weak recommendation/very low certainty of evidence: GRADE 2D).
Supplementary conditions
Changes in clinical conditions (e.g., patient characteristics, testing characteristics and timing, pre-test probability, patient/medical staff values) may change the balance of effects and result in a different option being recommended.
Rationale
Summary of evidence:
We found 6 studies on BNP and NT-proBNP levels in the blood. Blood BNP (cutoff value: 400–500 pg/mL) (3 studies [10,11,12]: N = 252) had an integrated sensitivity of 0.77 (95% confidence interval [CI]: 0.65–0.85) and integrated specificity of 0.62 (95% CI: 0.53–0.70). Blood BNP (cutoff value: 1000 pg/mL) (2 studies [11, 12]: N = 128) had an integrated sensitivity of 0.50 (95% CI: 0.36–0.64) and integrated specificity of 0.82 (95% CI: 0.72–0.89). Additionally, blood NT-proBNP (cutoff value: 4,000 pg/mL) (1 study [13]: N = 121) had an integrated sensitivity of 0.71 (95% CI: 0.52–0.85) and integrated specificity of 0.89 (95% CI: 0.80–0.94). The implementation of testing is generally supported when taking into account the balance between desirable and undesirable effects due to the implementation of testing.
Certainty of evidence:
The quality of evidence for the diagnostic performance of testing was judged as “very low” for almost all cases.
Balance of effects, acceptability, and feasibility determination:
This is already used in routine clinical practice, and there are no problems with acceptability and feasibility.
CQ3: Should serum C-reactive protein (CRP) and procalcitonin (PCT) levels be used for identifying bacterial pneumonia as the underlying disease of ARDS?Background
Pneumonia is a common causative disease of ARDS, most of which is bacterial pneumonia. Whether to use CRP and PCT for early recognition of this bacterial pneumonia is an important clinical question.
Recommendation
We suggest against identifying bacterial pneumonia as the underlying disease of ARDS only with serum CRP and PCT results (weak recommendation/very low certainty of evidence: GRADE 2D).
Supplementary conditions
Changes in clinical conditions (e.g., patient characteristics, testing characteristics and timing, pre-test probability, patient/medical staff values) may change the balance of effects and result in a different option being recommended.
Rationale
Summary of evidence:
We found 14 studies relating to serum CRP and 21 studies relating to serum PCT. Serum CRP (14 studies [14,15,16,17,18,19,20,21,22,23,24,25,26,27]: N = 3093) had a sensitivity of 0.76 (95% CI: 0.63–0.89) and specificity of 0.78 (fixed). Serum PCT (21 studies [14,15,16,17,18,19,20,21,22,23,24,25,26, 28,29,30,31,32,33,34,35]: N = 4,721) had a sensitivity of 0.64 (95% CI: 0.56–0.73) and specificity of 0.83 (fixed) (estimates using HSROC model, fixed at median value of specificity of primary studies).
Certainty of evidence:
In consideration of the risk of bias, indirectness, inconsistency, and inaccuracy, and certainty of evidence relating to the effects of testing was judged as “very low.”
Balance of effects, acceptability, and feasibility determination:
When comparing patients who are suspected of having bacterial pneumonia based on the results of serum CRP or serum PCT tests and those who are treated as if they have bacterial pneumonia regardless of the results of these tests, the latter may be more beneficial in situations, where the pre-test probability is estimated to be above a certain level. Complications from testing are thought to be negligible in terms of clinical decision-making. This is a widely used test with probably no problem regarding feasibility.
CQ4: Should pneumococcal urinary antigen tests and sputum Gram staining be used for identifying pneumococcal pneumonia as the causative disease of ARDS?Background
Pneumococcal pneumonia is a cause of acute respiratory failure and ARDS, and early medical intervention is important. Whether to use urinary pneumococcal capsular antigen tests and sputum Gram staining for conducting the early diagnosis of pneumococcal pneumonia is an important clinical question.
Recommendation
We suggest the use of pneumococcal urinary antigen testing and sputum Gram staining for identifying pneumococcal pneumonia as the causative disease of ARDS (weak recommendation/very low certainty of evidence: GRADE 2D.
Supplementary conditions
Changes in clinical conditions (e.g., patient characteristics, testing characteristics and timing, pre-test probability, patient/medical staff values) may change the balance of effects and result in a different option being recommended.
Rationale
Summary of evidence:
Pneumococcal urinary antigen testing (23 studies [36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58]: N = 10,900) had an integrated sensitivity of 0.65 (95% CI: 0.61–0.68) and integrated specificity of 0.91 (95% CI: 0.85–0.95). Sputum Gram staining (11 studies [55, 59,60,61,62,63,64,65,66,67,68]: N = 1794) had an integrated sensitivity of 0.69 (95% CI: 0.56–0.80) and integrated specificity of 0.91 (95% CI: 0.83–0.96).
Certainty of evidence:
The certainty of evidence relating to diagnostic performance for each test was judged as “very low.”
Balance of effects, acceptability, and feasibility determination:
When comparing the effects and harms of testing with the case, where the treatment policy was decided without testing, it is thought that the desirable effects of testing are large. This is a generally accepted medical practice with no problems regarding feasibility.
CQ5: Should Legionella urinary antigen testing be used for identifying Legionella pneumonia as the causative disease of ARDS?Background
Legionella pneumonia presents with rapid respiratory failure and is important as a causative disease of ARDS. Meanwhile, there is a possibility that an improved prognosis can be obtained with Legionella pneumonia with an appropriate administration of antibiotics, so whether to use Legionella urinary antigen testing is an important clinical question.
Recommendation
We suggest using Legionella urinary antigen testing for identifying Legionella pneumonia as the causative disease of ARDS (weak recommendation/very low certainty of evidence GRADE 2D).
Supplementary conditions
Changes in clinical conditions (e.g., patient characteristics, testing characteristics and timing, pre-test probability, patient/medical staff values) may change the balance of effects and result in a different option being recommended.
Rationale
Summary of evidence:
We found 21 studies [41, 69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88] relating to Legionella urinary antigen testing (N = 11,724); the integrated sensitivity was 0.79 (95% CI: 0.71–0.85) and the integrated specificity was 1.00 (95% CI: 0.99–1.00).
Certainty of evidence:
Considering the risk of bias, indirectness, and inconsistency for both sensitivity and specificity, the certainty of evidence was judged to be “very low.”
Balance of effects, acceptability, and feasibility determination:
When comparing the effects and harms of Legionella urinary antigen testing with the case, where the treatment policy was decided without testing, the desirable effects of testing are thought to be large. This is a generally accepted medical practice with no problems regarding feasibility.
CQ6: Should antigen and PCR tests of the pharyngeal swabs and serum antibody tests be used to identify Mycoplasma pneumonia as the causative disease of ARDS?Background
Mycoplasma pneumonia is relatively common as a form of community-acquired pneumonia and can rarely progress to ARDS and present with serious respiratory failure. Antigen and PCR tests of the pharyngeal swabs and serum antibody tests are generally used for the diagnosis of Mycoplasma pneumonia. Verifying the benefits and harms due to the implementation of these tests is an important issue in ARDS clinical practice.
Recommendation
We cannot provide a specific recommendation regarding whether to use antigen and PCR tests of the pharyngeal swabs or serum antibody tests for identifying Mycoplasma pneumonia as a causative disease of ARDS. The current status of these tests is that they are used based on the experience of clinicians (in our practice statement).
Supplementary conditions
None.
Rationale
Summary of evidence:
No applicable studies.
Since there is no high-quality evidence that investigated the diagnostic accuracy of tests, no clear recommendations can be made for this CQ. Therefore, we provided a description of the current clinical practice rather than an evidence-based recommendation for this CQ.
Certainty of evidence:
Since there are no applicable studies, the quality of evidence cannot be evaluated.
Balance of effects, acceptability, and feasibility determination:
The balance between benefits and harms is unclear. It is thought that there are no problems with regard to acceptability and feasibility, since these tests are conducted in daily clinical practice.
CQ7: Should antigen tests of the pharyngeal/nasopharyngeal swabs and PCR tests of the bronchoalveolar lavage fluid be used for identifying influenza pneumonia as the causative disease of ARDS?Background
It has been reported that the administration of neuraminidase inhibitors reduced hospitalization, pneumonia onset, and mortality rate in influenza virus infections. Antigen tests based on rapid diagnostic kits using pharyngeal swabs or nasopharyngeal swabs are commonly used in the diagnosis of influenza virus infections. Meanwhile, there are some reports that indicated that antigen tests using upper respiratory tract specimens could not diagnose novel Influenza A (H1N1) pneumonia, with diagnoses made using PCR tests of bronchoalveolar lavage (BAL) fluid. Diagnosing influenza pneumonia with these tests and conducting therapeutic intervention based on the administration of the appropriate antiviral medication is important.
Recommendation
We cannot provide a specific recommendation regarding whether to use antigen tests of the pharyngeal swabs and/or PCR tests of the BAL fluid for identifying influenza pneumonia as the causative disease of ARDS. The current status of these tests is that they are used based on the experience of clinicians (in our practice statement).
Supplementary conditions
None.
Rationale
Summary of evidence:
No applicable studies.
Certainty of evidence:
Since there are no applicable studies, the quality of evidence cannot be evaluated.
Balance of effects, acceptability, and feasibility determination:
The balance between desirable effects and undesirable effects is unclear. It is thought that there are no problems regarding acceptability and feasibility.
CQ8: Should PCR tests of the bronchoalveolar lavage fluid and blood antigenemia methods be used for identifying cytomegalovirus pneumonia as the causative disease of ARDS?Background
The cytomegalovirus (CMV) pneumonia blood antigenemia method and CMV-PCR test of the BAL fluid are used for the early diagnosis of CMV infection and determination of the effect of treatment, and they are widely used as an index for monitoring, determining the effect of antiviral agents, and the discontinuation period.
Recommendation
We suggest using PCR tests of BAL fluid and blood antigenemia methods for identifying CMV pneumonia as the causative disease of ARDS (weak recommendation/very low certainty of evidence: GRADE 2D).
Supplementary conditions
Changes in clinical conditions may change the balance of effects and result in a different option being recommended.
Rationale
Summary of evidence:
PCR tests using BAL fluid (5 studies [89,90,91,92,93]: N = 353) had an integrated sensitivity of 0.94 (95% CI: 0.86–0.97) and integrated specificity of 0.84 (95% CI: 0.52–0.96).
Blood antigenemia methods (3 studies [94,95,96]: N = 91) had an integrated sensitivity of 0.67 (95% CI: 0.54–0.79) and integrated specificity of 0.87 (95% CI: 0.73–0.95) when the definition of “positive” was at least one positive cell per 200,000. Furthermore, the frequency of adverse events with BAL was as follows: mortality, 0.000% (95% CI: 0.000–0.035).
Certainty of evidence:
For both PCR tests of the BAL fluid and blood antigenemia methods, the certainty of evidence was judged as “very low” after considering the risk of bias, etc. The certainty of evidence regarding the harm of BAL was judged as “moderate” or “low.”
Balance of effects, acceptability, and feasibility determination:
Benefits included appropriate treatment based on diagnosis, and harms included unnecessary treatment due to misdiagnosis (false positive) and adverse events. When compared with cases, where the treatment policy was decided without testing, the benefits were thought to be large. This is a feasible medical practice.
CQ9: Should serum β-D-glucan be used for identifying Pneumocystis pneumonia as the causative disease of ARDS?Background
Pneumocystis pneumonia (PCP) causes acute respiratory failure, and it is anticipated that early diagnosis with serum β-D-glucan testing would contribute to the improved prognosis of patients. Meanwhile, misdiagnosis with PCP is thought to worsen patient prognosis through the administration of unnecessary drugs and its side effects, as well as the lack of implementation of treatments for other causative diseases. Verifying the benefits and harms of test implementation is an important issue in ARDS clinical practice.
Recommendation
We suggest using serum β-d-glucan tests for identifying PCP as the causative disease of ARDS (weak recommendation/very low certainty of evidence: GRADE 2D).
Supplementary conditions
Changes in clinical conditions (e.g., patient characteristics, testing characteristics and timing, pre-test probability, patient/medical staff values) may change the balance of effects and result in a different option being recommended.
Rationale
Summary of evidence:
When setting a cutoff value (80 pg/mL) for serum β-d-glucan (3 studies [97,98,99]: N = 148), the integrated sensitivity and integrated specificity of PCP diagnosis were 0.84 (95% CI: 0.66–


留言 (0)