
記住我
The COVID-19 pandemic and the control measures adopted since its inception have had a short-term and medium-term impact on the supply of and access to preventive and curative health services globally, for a multiplicity of acute and chronic health conditions, including urgent ones, regardless of the burden of the epidemic in each area.1 2
The Italian network MIMICO-19 was set up in early 2020 to estimate the indirect effects of the pandemic on hospital utilisation and quality of care in seven regions representing the country. Early findings showed that during the first wave, access to the emergency room (ER), and hospitalisation for cardiovascular diseases and for planned or oncological surgery dropped. Conversely, the timeliness of time-dependent interventions remained unchanged.3
Inequalities in access to healthcare are well documented, even in universal health systems.4 The contraction in healthcare supply and utilisation caused by the SARS-CoV-2 epidemic can potentially exacerbate social inequalities in health in the context of a syndemic pandemic resulting from the interaction between the unequal distribution of the COVID-19 burden, the non-communicable diseases and the social determinants of health.5 6 However, whereas there is a mounting literature unveiling the socially patterned nature of the pandemic and showing that COVID-19 risks and unfavourable outcomes are higher among black and minority ethnic groups,7 and individuals from socioeconomically deprived backgrounds,8–10 little is known about the indirect effects of COVID-19 on health and healthcare inequalities. Despite early concerns about the disproportionately large negative impact of the disruption of care on vulnerable populations,11 to the best of our knowledge, only few studies have investigated how the pandemic is undermining the equity of access to and utilisation of health services for conditions other than COVID-19.12–14
The main objective of the study is therefore to evaluate the indirect impact of COVID-19 and related containment measures on socioeconomic inequalities in hospital utilisation and quality of care through a selection of validated indicators in Italy. The secondary objective is to assess potential variations in gradients by sex and age class.
MethodsStudy design, population and data sourcesThis is a multicentre retrospective study carried out within the MIMICO-19 network3 and based on the individual record linkage of regional health administrative and statistical data sources via a unique anonymous key.15 Socioeconomic information relevant for the study was available for five regions (Piedmont, Emilia-Romagna, Tuscany, Puglia, Sicily) and two metropolitan areas: the local health unit of Milan (ATS Milan) and the municipality of Rome.
The study population, derived from the health population registers, consisted of the residents as of 1 January 2018 in each of the above-mentioned geographical areas aged ≥30 years in 2011 and still alive during the observation time.
We considered two observation periods: (1) pandemic period; (2) comparison period covering the average of the corresponding subperiods in 2018–2019.
Hospital discharge and ER archives were used to retrieve the outcomes of interest. The last census, held in 2011, was the source of the information on the socioeconomic position (SEP) measured through the individual educational level in adulthood (ie, in those aged ≥30 years) and the deprivation index at the census block level.16
OutcomesWe chose 12 indicators of hospital utilisation and quality of care encompassing several clinical areas and validated within the National Healthcare Outcomes Programme, an evaluation programme run by the National Agency for Regional Healthcare Services.17 Hospital utilisation was assessed through indicators of volume, defined as absolute number of cases or procedures: five for acute conditions, two for scheduled surgery and three for oncological surgery. To represent the healthcare quality, we chose two indicators of timeliness of procedures. For each indicator, we included all episodes registered in the study population within the two observation periods. Table 1 reports the indicators, the International Classification of Diseases, Ninth Revision codes used in their definition and their availability.
Table 1List of indicators with their selection criteria (ICD-9-CM codes, and age and sex where applicable) and geographical availability
Exposures and other variablesEducational level was our primary SEP indicator, because it is a reliable measure that bridges socioeconomic conditions from early life to adulthood.18 It was classified into three levels according to the highest attained qualification: low (primary education or less, corresponding to the 0–1 levels of the International Standard Classification of Education 1997, modified in 2011 (ISCED-11),19 middle (lower secondary and short-cycle upper secondary education, ISCED-11: 2–3C), high (from completed upper secondary onwards, ISCED-11: from 3A/B upwards). However, information on education was only available for three regions (Piedmont, Emilia-Romagna, Puglia) and the municipality of Rome.15 Therefore, we also used the deprivation index at the census block, as a proxy of individual SEP,20 which was available for all geographical areas included in the study. It was grouped into five quintiles (1 less deprived, 5 more deprived) and used in the secondary analyses whose results are commented in the text but only reported in the online supplemental material.
Age was classified into 5-year age bands (30–34, 35–39, …, 85+) for adjustment and into two groups (30–64, 65+) for stratification.
Statistical analysesAll analyses were carried out for each sex and age group to explore whether differences exist within these population strata.
To assess whether the association between SEP and outcomes was modified by the pandemic and the lockdown measures, we employed both a descriptive and an analytical approach.
First, we estimated age-standardised rates (number of episodes/population) for the volume indicators and age-standardised prevalence (number of procedures/total access eligible for that procedure) for the indicators of timeliness of procedures through direct standardisation using the 2013 European standard population.21 Standardised rates were stratified by observation period and SEP indicator. To assess changes over time for each SEP stratum, we computed relative per cent changes as the ratio between the difference of rates or prevalence in the pandemic and the pre-pandemic periods and the rates or prevalence in the pre-pandemic period.
Second, we fitted Poisson models (with robust errors for process indicators22) adjusted for age and geographical area, and with an interaction term between SEP indicators and period. Through these models, we estimated the Relative Index of Inequality (RII), a summary measure that quantifies the social gradient in relative terms,23 for both the pandemic and the pre-pandemic periods. Values above 1 indicate worse outcomes in the most disadvantaged group whereas those below 1 in the most advantaged one. To test the interaction, we used the likelihood ratio test for volume indicators and the Wald test for timeliness of procedures indicators.
ResultsInequalities by educational levelThe four areas included in the main analysis cover approximately 9.5 million people, about 20% of the Italian inhabitants aged ≥30 years. Piedmont and Emilia-Romagna contribute for about 30% each, Rome for the 17%, and Puglia for the 25%; 42% and 47% of male and female population, respectively, were aged >65 years (table 2). During the first 7 months of the pandemic, volumes of total access to ER and scheduled surgery dropped by approximately one-third compared with 2018–2019; the lowest reduction was registered for the malignant lung cancer surgery with a 4% decline among men and a 9% increase among women (absolute numbers for 2018–2019 are reported in online supplemental table 1).
Table 2Age and geographical distribution of the population, absolute number (N) and column and row percentage (%) of hospital volumes and timeliness of procedures in 2020 and per cent change from 2020 to 2018–2019 by educational level and sex
Figure 1 shows the relative per cent changes in the age-standardised rates and prevalence by sex and age groups (underlying rates and details of per cent changes are reported in online supplemental table 2). Both rates and prevalences were generally lower during the pandemic year compared with 2018–2019. Besides, relative per cent reductions of volumes rates were generally greater among the low educated of both sexes and age groups; on the contrary, reductions on the prevalence of timely procedures were less pronounced and not explicitly socially patterned. Women experienced larger declines than men. Subjects aged ≥65 years experienced the greater contraction in hospital volumes compared with the younger counterpart, except for access to the ER in both sexes and timeliness of percutaneous transluminal coronary angioplasty (PTCA) among women.
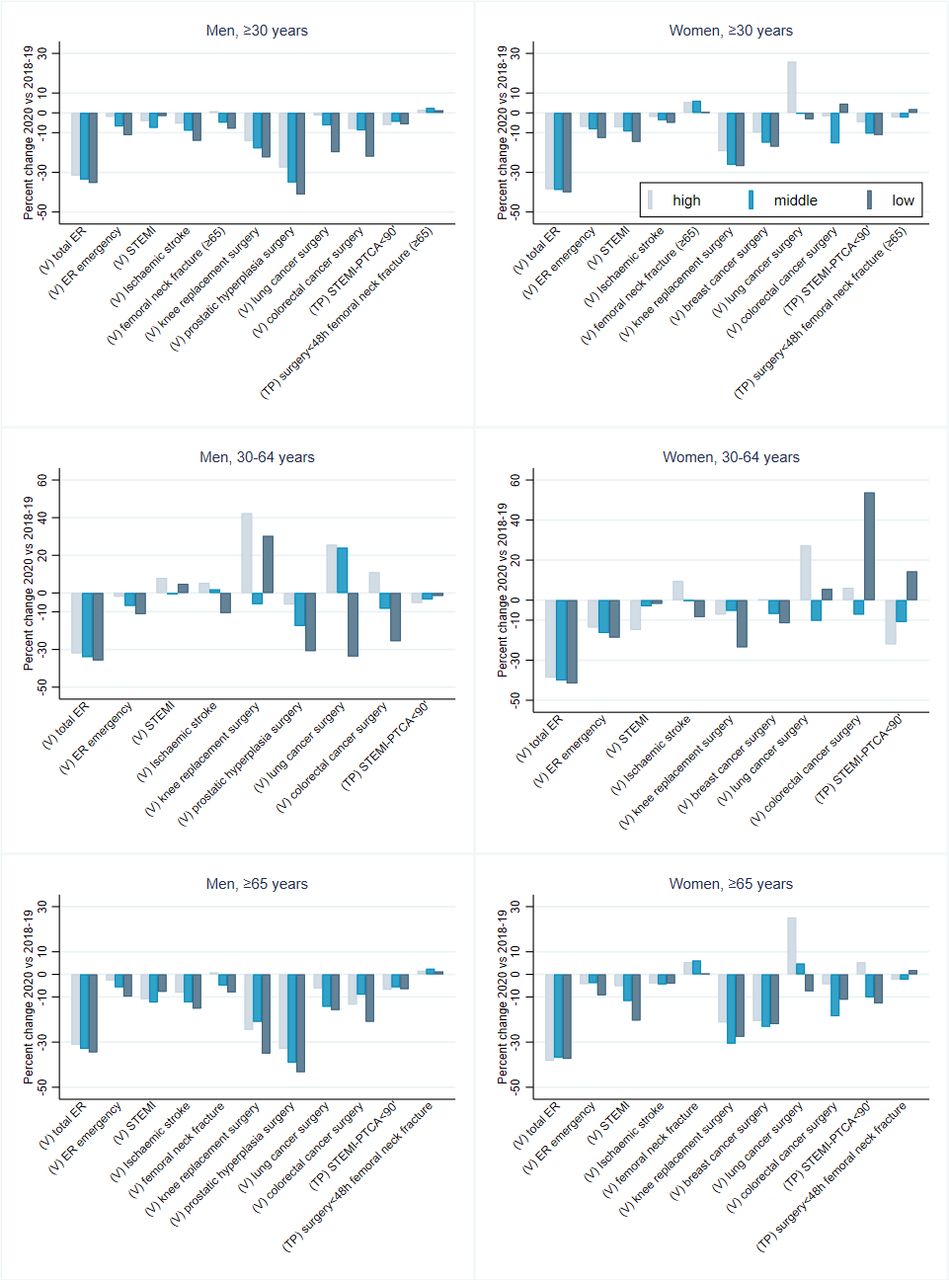 Figure 1
Figure 1 Relative per cent changes of age-standardised rates for the volume indicators and age-standardised prevalence for the timeliness of procedure indicators by educational level, sex and age group. ER emergency not available for Rome; IMA STEMI-PTCA <90’ not available for Emilia-Romagna. ER, emergency room; PTCA, percutaneous transluminal coronary angioplasty; STEMI, ST-elevation myocardial infarction; TP, timeliness of procedures; V, volumes.
These differential reductions were mirrored in the changes in the social gradient of volumes and timeliness indicators measured through the RII. For most of the indicators, educational differences were evident both in 2018–2019 and in 2020; however, during the 7 months of 2020, greater rates’ drops occurred among the low educated and therefore the gradient for all volume indicators either shrank (for those whose risk was greater than 1, eg, total ER access) or widened (for those whose risk was close to or lower than 1, eg, prostatic hyperplasia surgery) (figure 2). Furthermore, there was an interaction between educational level and period suggesting significant changes in the educational gradient in 2020 for all volume indicators in both sexes. In the analyses by age group (figure 3), educational differentials were wider among men and people aged 30–64 years than their counterparts, although the uncertainty of the estimates was greater among the youngest mainly due to a small number of events in this age group. Moreover, some interactions lost their statistical significance. In the age group 30–64 years, reductions of the gradient remained significant only for ER access in both sexes and for indicators of prostatic hyperplasia surgery in men and breast cancer surgery in women. In the age group ≥65 years, the educational gradient significantly narrowed for indicators of ER access and scheduled surgery in both sexes, and for indicators of acute cardiovascular conditions (ST-elevation myocardial infarction (STEMI) and ischaemic stroke) and lung cancer surgery among women.
 Figure 2
Figure 2 Relative Index of Inequality and 95% CIs by educational level, hospital volumes and timeliness of procedure indicators and period, and sex, all ages. ER emergency not available for Rome; IMA STEMI-PTCA <90’ not available for Emilia-Romagna. ER, emergency room; PTCA, percutaneous transluminal coronary angioplasty; STEMI, ST-elevation myocardial infarction; TP, timeliness of procedures; V, volumes; p, p value for interaction.
 Figure 3
Figure 3 Relative Index of Inequality and 95% CIs by educational level, hospital volumes and timeliness of procedure indicators, period, sex and age group. ER emergency not available for Rome; IMA STEMI-PTCA <90’ not available for Emilia-Romagna. ER, emergency room; PTCA, percutaneous transluminal coronary angioplasty; STEMI, ST-elevation myocardial infarction; TP, timeliness of procedures; V, volumes; p, p value for interaction.
Conversely, indicators of timeliness of procedures did not show neither a gradient nor relevant changes across time in both sexes and age groups.
Inequalities by deprivation indexThe seven geographical areas for which the deprivation index was available totalled about 16 million individuals, one-third of the Italian population aged ≥30 years (online supplemental table 3).
Relative per cent changes in the age-standardised rates for volume indicators and prevalence for timeliness of procedures indicators did not show a clear social gradient meaning that they were not consistently higher among the more or less deprived nor any difference between the two age groups emerged (online supplemental figure 1 and online supplemental table 4). As seen for education, declines were consistently greater among women. The RIIs revealed that, although inequalities in access to ER, cardiovascular acute conditions and scheduled surgery were present before the pandemic, their magnitude did not substantially change in 2020 (online supplemental figures 2 and 3), except for total ER access and malignant lung cancer surgery among men of all ages, total ER access among women aged 30–64 years old and malignant colorectal cancer among women aged ≥65 years. It is worth noting that for total ER access, the gradient by deprivation index showed a tendency to widen, contrary to what happened for educational inequalities.
DiscussionThis multicentre study covering seven Italian geographical areas showed that, compared with 2018–2019, hospital volumes and, to a lesser extent, indicators of timeliness of procedures fell during the first 7 months of the COVID-19 pandemic, with larger declines among women and the elderly. At the same time, the low educated of both sexes, who are at higher risk of baseline hospital admission because of their greatest burden of diseases, experienced larger drops in ER access and most of the hospitalisation rates, with a resulting shrinkage (or widening when the RII was <1) of the educational gradient for volume indicators. Indicators of timeliness of procedures did not show any educational gradient neither before nor during the pandemic. The assessment of inequalities through the deprivation index returned a more nuanced picture with smaller differentials whose magnitude did not substantially change in 2020. Our results are in line with the scant evidence on the indirect effects of COVID-19 on healthcare inequalities showing that socially vulnerable individuals, women and the elderly have suffered more from disruptions in healthcare provision.12–14
The reasons behind the global decrease in hospital utilisation during the pandemic are manifold and, arguably, deeply intertwined with the root causes of health inequalities. They span from the massive reorganisation of hospital care to the change in patients’ behaviours, a possible decrease in disease incidence, and the presence of competing risks from COVID-19 and excess mortality.1 2 24
In Italy as elsewhere, the sudden widespread of the pandemic has triggered a profound reorganisation of the national health service, including the hospital system, with changes in the supply of services other than COVID-19 diagnosis and treatment and suspension and cancellation of deferrable interventions such as elective surgery.25 Concurrently, the warnings about the SARS-CoV-2 and the ‘stay-at-home’ messages issued by public authorities have likely induced a self-limitation of the demand in the population who worried about hospital contamination. The ability to access to and travel through healthcare services as well as to adhere to public health recommendations and realise whether a health problem is urgent enough to seek medical care or to wait and see is influenced by individual and system-level factors. These factors include SEP, culture and language, self-efficacy and perceived barriers, which together contribute to define the level of health literacy,26 and system’s complexity and acute care orientation.27 In line with the results of a Danish study, we found that, during the pandemic, low educated people generally experienced lower access to hospital compared with their higher educated counterpart. This may result from increased barriers of access, mostly experienced by socioeconomically vulnerable populations, due to the unexpected system’s rearrangement and a restrictive interpretation of recommendations which led to avoidance of medical care for fear of COVID-19, for both potentially life-threatening conditions, such as myocardial infarction, and scheduled interventions, such as knee replacement.
Inequalities not only ran along the lines of SEP but also at the intersection with age and gender. Contractions in hospital utilisation were larger among the oldest subjects, a result that emerged also from a European multinational study,14 possibly linked to a greater fear of the infection consequences. We also found that women, especially those more disadvantaged, experienced larger drops in hospital access than men, another finding reported by previous researches.13 14 This may reflect gender inequalities stemming from women often playing a central caring role in the family setting and prioritising relatives’ needs over their own13 and a greater compliance with activity-restraining policy measures.28
Decreased service utilisation may also result from an increase use of digital health solutions (eg, telemedicine, online and apps information exchanges, remote patient engagement),29 whose utilisation has ramped up during the pandemic, though not uniformly at national level.30 Our information systems cannot currently capture trends in digital health and therefore we could not ascertain whether digital solutions have had a differential reach across social groups (eg, larger use among deprived communities living in rural areas). However, it is worth recalling that overlooking equity issues in the development of digital care may further amplify existing health inequalities.31
The decrease in diseases’ incidence, such as myocardial infarction and stroke, has also been claimed as a reason for reduced hospital access during the pandemic.2 However, the lower utilisation is likely to be the effect of people avoiding hospitals, especially vulnerable groups as argued before, and eventually dying at home from untreated conditions rather than of a lower incidence. This hypothesis has been confirmed by Italian studies reporting a significant reduction of hospitalisation for myocardial infarction but also a concomitant increase in the out-of-hospital cardiac mortality.32 33
Italy has paid a very high toll in terms of mortality during the first pandemic phases34; the risk of all-cause and COVID-19-related death was higher among the elderly35 and among deprived groups.8 This competing risk from COVID-19 and excess mortality may have depleted the population in need of hospital assistance, especially the most disadvantaged and oldest pockets, and may partially explain the unequal decrease in hospital utilisation.
The good news is the absence of educational inequalities in PTCA interventions in patients with STEMI and surgery for femoral neck fracture in the elderly, whose timeliness was guaranteed during the pandemic. This result is in line with earlier findings of a study carried out in Lazio region that reported improvements over time in terms of equity due to an increasingly comparable management across educational levels for both PTCA in patients with STEMI and femoral neck fracture surgery.36 Authors argued that the greater is the urgency, the more the inequality decreases and that healthcare organisation and quality seem to be more important than patients’ choice in time-sensitive procedures. Our findings too suggest that patients’ hospital management is not affected by individual SEP and that health inequalities mostly originate outside secondary care and are driven by wider determinants (eg, education, housing, working conditions, access to primary and preventive healthcare), which interact syndemically to shape people’s exposure to noxious factors.
Estimates by deprivation did not show a clear social gradient nor significant changes between the pre-pandemic and pandemic period, even when we only considered the areas included in the main analyses by education (online supplemental table 5). A certain degree of exposure misclassification and, to a lesser extent, the ecological bias inherent to the metric may explain these results. Indeed, the deprivation index is based on 2011 sociodemographic data16 whose distribution has sensibly changed in the last decade, especially in metropolitan areas, and therefore it may not accurately describe the current distribution of the social and material deprivation and dilute the association between SEP and outcomes.
Strengths and limitationsThe is the first study to assess socioeconomic inequalities in hospital utilisation for conditions other than COVID-19 during the pandemic in Italy, and one of the few in Europe. It draws upon health information and administrative registries that virtually cover the entire resident population minimising the risk of selection bias and allow to follow people over time37 and explore multiple outcomes simultaneously. Moreover, thanks to its wide geographical coverage, it provides a robust approximation of the national situation during the first pandemic phases. The study is not exempt from drawbacks. As recalled above, the information on SEP came from the 2011 census and may not accurately describe the current situation. However, the educational level is deemed to be stable after the age of 30 years18 and therefore the 2011 data can still be considered a reliable source. Unfortunately, however, this information was available only for four areas. In order to implement a comprehensive and timely monitoring systems for health inequalities, a more complete availability of socioeconomic data on health information systems would be desirable, as also recommended by the Joint Action on Health Equity Europe.38 Results cannot be generalised beyond national borders because of both the intensity with which the pandemic hit the country and the features of our national health system, which guarantees universal access to the population. Finally, the nature of our study did not allow to directly investigate the reasons behind the decrease in hospital utilisation and the underlying social patterns.
Conclusions and implications for policiesDuring the first months of the COVID-19 pandemic in Italy, the low educated, the elderly, and the women experienced significant ER access and hospitalisation contraction with the consequent shrinkage of the social gradient.
Midterm and long-term consequences of this socially patterned reduction range from a surge in late-presenting conditions to a potential exacerbation of health inequalities among those groups who were already the most vulnerable before the pandemic. Besides public policies expanding social protection and public services,6 the healthcare service as a whole should contribute to contrast health disparities worsened by COVID-19. As recommended by the Independent Panel for Pandemic Preparedness and Response, to protect the most vulnerable populations’ health in the pandemics that may occur in the future, countries need to prepare effective, coordinated and equity-oriented containment strategies.39 To this extent, it is crucial to deliver a more efficient communication on how and when to safely access care to enable people, particularly the most disadvantaged, to navigate the system. It is also vital to strengthen primary healthcare and preventive services to implement locally appropriate interventions and foster community participation and empowerment. These efforts, along with those needed to act on the wider social determinants, require a sustained financial support in terms of human resources and infrastructures as envisaged in the Italian National Recovery and Resilience Plan40 that represents an unprecedented opportunity to tackle health inequalities.
留言 (0)