
記住我








The study was conducted as a non-interventional retrospective new-user cohort study using longitudinal German statutory health insurance (SHI) claims data of the Institute for Applied Health Research Berlin (InGef) Research Database. The research database comprises anonymized healthcare claims of more than four million covered lives insured in approximately 60 SHIs in Germany. This sample covers approximately 4.8% of the German population [12] and 5.6% of the German SHI population [13] as of 2020 and is structured to represent the German population in terms of age and gender according to the Federal Office of Statistics (DESTATIS [12]). The InGef Research Database was proven to have good external validity to the German population in terms of morbidity, mortality, and drug use [14]. Available data domains include core data regarding patients’ demographics, outpatient and inpatient healthcare services with diagnoses, procedures, and operations, prescription data, data on remedies, devices, and aids, and sick leave payments on an anonymized case-by-case level.
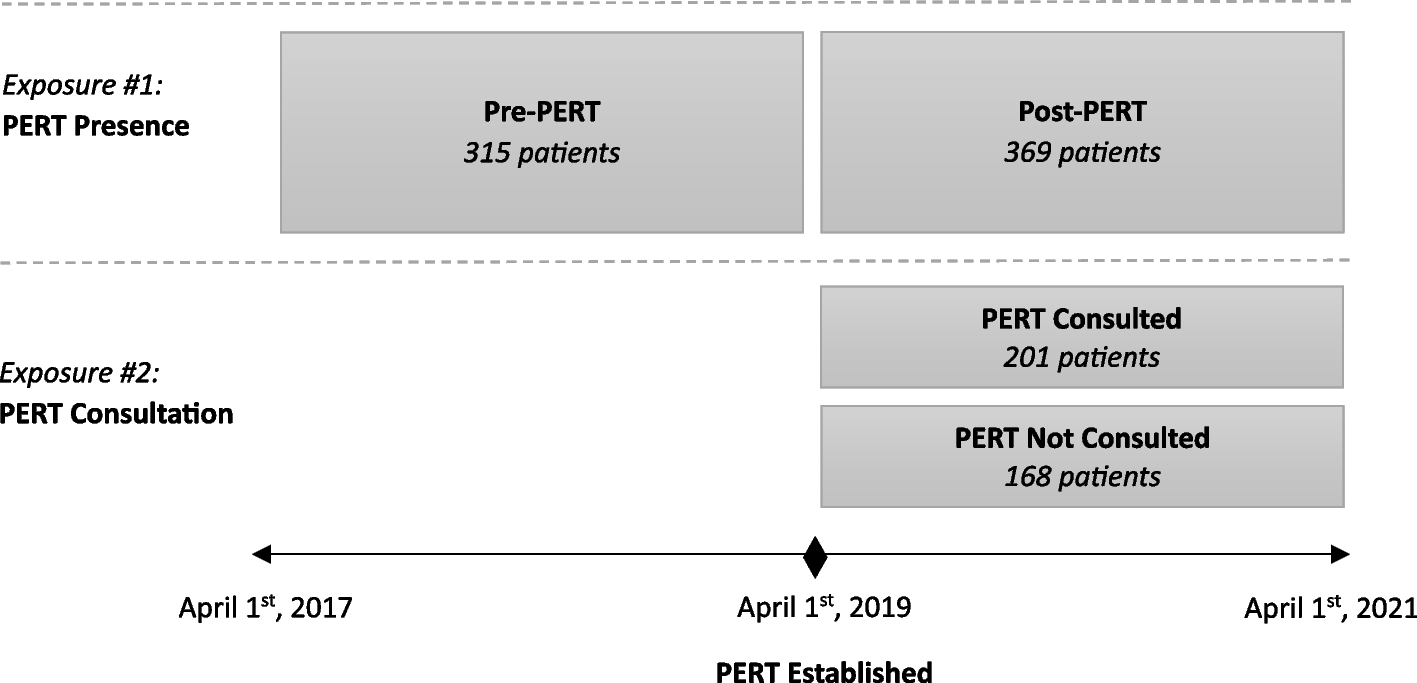
Study timeframeThe study period spanned from January 1st, 2014 until June 30th, 2019. NVAF patients initiating treatment with edoxaban or phenprocoumon for stroke prevention were identified between January 1st, 2015 through December 31st, 2018. The index date was defined as the first edoxaban or phenprocoumon dispensation documented in the identification period and marked the beginning of the individual post-index period. Figure 1 gives an overview of the study periods and timeframes.
Fig. 1
Study periods and timeframe
Study populationThe study population consisted of all NVAF patients who initiated edoxaban (60 mg or 30 mg) or phenprocoumon treatment between January 1st, 2015 and December 31st, 2018. All patients who had an ambulatory verified or primary or secondary hospital discharge diagnosis of AF in the previous or same quarter as the index date, who were aged ≥ 18 years in the index quarter, and who were continuously enrolled in the individual pre-index period of 365 days/four quarters before the index date were further included in the study.
Patients receiving any anticoagulant substanceFootnote 1 within the previous 365 days before the index date, more than one anticoagulant substance, or more than one dosage of edoxaban (60 mg and 30 mg) on the index date were excluded from the study. In addition, patients with at least one coded dialysis in the 365 days before or on the index date, patients receiving edoxaban/phenprocoumon and heparin on the index date, patients with documented cardiac valve surgery in the 365 days prior to the index date or on the index date, patients who presented any evidence of pregnancy in the four quarters prior to or in the index quarter, and patients with thrombosis or pulmonary embolism in the four quarters prior to or in the index quarter were excluded.
Study medication was identified by German Pharmaceutical Registration Numbers (PZN) or Anatomical Therapeutic Chemical Classification System (ATC) codes, diagnoses by outpatient and inpatient International Classification of Diseases, 10th Revision, German Modification (ICD-10-GM) codes, and procedures based on Key of Operations and Procedures (OPS) for inpatient procedures and German Physician Fee Schedule (EBM) codes for outpatient procedures.
Baseline characteristics of the study population were descriptively assessed in the individual pre-index period of 365 days/four quarters preceding the index date and included demographic characteristics, healthcare resource utilization, comorbidities, concomitant medications, and risk scores (CHA2DS2-VAScFootnote 2 [15], modified HAS-BLEDFootnote 3 [16], Charlson Comorbidity Index (CCI) [17,18,19]) associated with stroke and bleeding. If available, the definition and operationalization of covariates were set as closely aligned as possible with the publication of Hohnloser et al. [10] and the corresponding study report [20]. A definition of the respective baseline characteristics and the ICD-10-GM codes can be found in Additional file 1.
Geriatric patientsSubgroup analyses on geriatric patients were performed regarding age, comorbidities, polypharmacy, and frailty. In the first geriatric subgroup, the study population was stratified by age groups (< 65 years, 65–74 years, ≥ 75 years) with age determined in the index quarter.
For the second geriatric subgroup, comorbidities were assessed using the CCI weighing comorbidities that occurred in the pre-index period. A global CCI score for the total population of patients receiving edoxaban or phenprocoumon was calculated based on ambulatory verified as well as primary and secondary hospital discharge diagnoses within the 365 days/four quarters before the index date. Included conditions and their assigned weights were based on the original classification of diseases by Charlson et al. [17], incorporating the ICD-9 adaption by Deyo et al. [18] and ICD-10 adaption by Quan et al. [19]. High comorbidity was defined as scoring above the median score of the overall study population (individual CCI > median CCI).
The third geriatric subgroup was formed based on frailty, which was exploratorily applied according to a modified score based on auxiliary diagnoses from the publication of Segal et al. [21]. The approach of frailty classification using claims-based diagnoses was recently validated in the US against the Fried criteria as a gold standard of frailty assessment and showed a strong association with all-cause mortality and admissions to hospital or nursing homes [22]. To predict the probability of frailty for each patient in the study population, a claims-based frailty index (CFI) was calculated using the CFI variables and β coefficients from the adaptive lasso regression derived in Cardiovascular Health Study data by Segal et al. [21]. The median CFI of the overall study population was used to differentiate between frail (CFI > median CFI) and non-frail patients (CFI ≤ median CFI).
The fourth geriatric subgroup consisted of patients presenting with polypharmacy. Polypharmacy was defined as an intake of more pharmaceutical substances based on unique ATC codes on a 7-digit basis during the individual pre-index period of 365 days before the index date than the median of the overall study population (individual intake > median intake).
Study outcomesAll study outcomes were assessed that occurred within the individual post-index period spanning from the index date until the occurrence of the first primary or secondary effectiveness or safety event investigated, the end of the study period on June 30th, 2019, the end of continuous enrollment (e.g., due to sickness fund switch or death), discontinuation of edoxaban or phenprocoumon treatment, or treatment switch to another anticoagulant therapy (including warfarin), whatever came first. The exposure start date for each patient was defined as the first edoxaban or phenprocoumon dispensation (dispense date) documented in the identification period spanning from January 1st, 2015 until December 31st, 2018. The exposure time was defined as the days of supply plus the days of not outcome-related hospitalization and a gap period of 30 days. As edoxaban is prescribed at a fixed dose, the number of days’ supply was set equal to the package size or the number of days until the new prescription. In order to account for the intra- and interpersonal variability of the phenprocoumon treatment regime (INR control and potential titration of phenprocoumon), an empirical defined daily dose based on the observed phenprocoumon prescription patterns was computed.
The primary effectiveness outcome of interest was the composite endpoint consisting of stroke (ischemic or hemorrhagic) and SE. Secondary effectiveness outcomes included all strokes, ischemic stroke, hemorrhagic stroke, and all-cause mortality. Effectiveness outcomes were identified based on primary or secondary hospital discharge ICD-10-GM diagnosis codes. A complete list of all ICD-10-GM codes used to identify the effectiveness endpoints and their operationalization is provided in Additional file 2. All-cause mortality included death from any cause.
The primary safety endpoint of interest was major bleeding and was defined as either cases with documented primary or secondary hospital discharge ICD-10-GM diagnosis codes of a major bleeding event in accordance with ICD-10-GM codes classified as major or intracranial bleeding, or hospital cases with an emergency admission in combination with an any bleeding or gastrointestinal bleeding event coded in accordance with ICD-10-GM codes classified as any or gastrointestinal bleeding and validated by the documentation of the OPS code 8-800 or the ICD-10-GM code D62. The secondary safety endpoints were intracranial bleeding, gastrointestinal bleeding, and any bleeding events, which were identified by primary or secondary hospital discharge ICD-10-GM diagnosis codes and OPS codes. A complete list of all ICD-10-GM and OPS codes used to identify the safety endpoints and their operationalization is provided in Additional file 3.
Statistical analysisFor continuous variables such as age and number of hospitalizations, baseline characteristics were assessed using descriptive statistics including the number (n) and percentage (%) of subjects, mean, and standard deviation (SD). Frequencies and percentages were displayed for categorical data. Percentages by categories were based on the number of subjects with no missing data, i.e., added up to 100%. To estimate the balance between the treatment groups edoxaban vs phenprocoumon, the absolute standardized difference (ASD) was calculated. Phenprocoumon was used as the reference group while the threshold indicating imbalance was set to 0.1 [23].
Crude event rates and corresponding 95% confidence intervals (CIs) of the primary and secondary endpoints were described as the number of events per 100 person-years (% per year). Person-years of follow-up were calculated from the initiation of treatment with edoxaban or phenprocoumon to the occurrence of the first event investigated, the end of continuous enrollment, death, the end of the study period, discontinuation of treatment, or switching to another oral anticoagulant (including warfarin), whichever came first. Crude event rates for each endpoint and treatment group were calculated by dividing the number of events by the person time and reported per 100 person-years.
The adjusted event rates were calculated using a Poisson regression model, which considered a fictive patient who possessed the average baseline demographics and clinical characteristics of all patients. The primary and secondary endpoints served as dependent variables, while baseline characteristics and treatment groups were considered as independent covariates. Baseline variables were regarded time-independent, i.e., only the covariates’ value at baseline was considered. Adjusted event rates for the individual treatment groups were the marginal mean values of the prediction derived by the Poisson model and reported per 100 person-years.
To compare the risk for stroke/SE and all-cause mortality (effectiveness events), and bleedings (safety events) between NVAF patients initiating edoxaban and phenprocoumon treatment, hazard ratios (HR) were estimated through multiple outcome-specific cox proportional hazard regression models. Edoxaban was compared to phenprocoumon with phenprocoumon serving as reference category in the analysis. Adjustment included demographic characteristics, comorbidities, and risk factors for stroke/SE and bleeding as dependent variables, while the treatment groups were included as independent covariate. Covariates with significant influence on the multiple outcome-specific cox proportional hazard models were selected through machine learning in terms of backward elimination.
For building of the geriatric subgroups regarding age, comorbidity, frailty, and polypharmacy, the number and percentage of patients in each cohort and summary measures in terms of mean and SD were determined. Baseline characteristics and clinical features were stratified by treatment group (edoxaban vs phenprocoumon) and by subgroups of geriatric patients. In line with the main analysis, differences in the risk of primary and secondary effectiveness and safety events between the treatment groups were determined for geriatric patients. Multiple outcome- and geriatric subgroup-specific cox proportional hazard models were used to estimate the treatment effect on the respective event rates. Using analysis of variance, the effect modification by geriatric subgroups on the association between treatment and outcomes was tested by adding interaction terms for the age, comorbidity, frailty, and polypharmacy subgroups to the multiple cox proportional hazard regressions.
留言 (0)