This is the first immunohistochemical comparison of the laryngeal tissue of a patient with C1-INH-HAE who died from suffocation caused by upper airway angioedema with a control patient who died from other condition without any signs of angioedema. We found strong C1-INH staining in both patients—i.e., in the C1-INH-HAE and control patient-, besides a slightly decreased BDKRB1 and BDKRB2 expression and more intensive T cell/monocyte infiltration in the C1-INH-HAE patient. Interestingly, PAR1 expression was significantly lower in the C1-INH-HAE patient, which may reflect to receptor consumption due to PAR1 activation.
The major limitation of our study is that only a single HAE patient’s data have been involved, so every observation of ours should be considered with special care. Although obtaining in vivo samples from angioedematous tissues raises ethical issues, in particular, the biopsy (a known trigger factor of AE attacks) may further worsen the patient’s condition—especially in the case of submucosal edema formation [13], our observations urge these in vivo biopsy studies to clarify the local role of PAR1, BDKRBs and active serine proteases. Skin biopsy studies during HAE attacks would be even more important because a submucosal tissue biopsy is hardly achievable during attacks, and because of the almost negligible chance for obtaining post mortem specimen from the larynx of a C1-INH-HAE patient who succumbs to suffocation from laryngeal edema. Specifically, UAE is rare in C1-INH-HAE—occurring in approximately 0.9% of all AE attacks—and the proportion of patients who have ever experienced UAE during their lifetime is 50% (Bork et al.[4] and our unpublished data). Furthermore, nowadays, patients are sufficiently informed about the risk of UAE, as well as they are adequately trained and supplied with emergency treatments [14]. Consequently, the risk of fatality from UAE is extremely low.
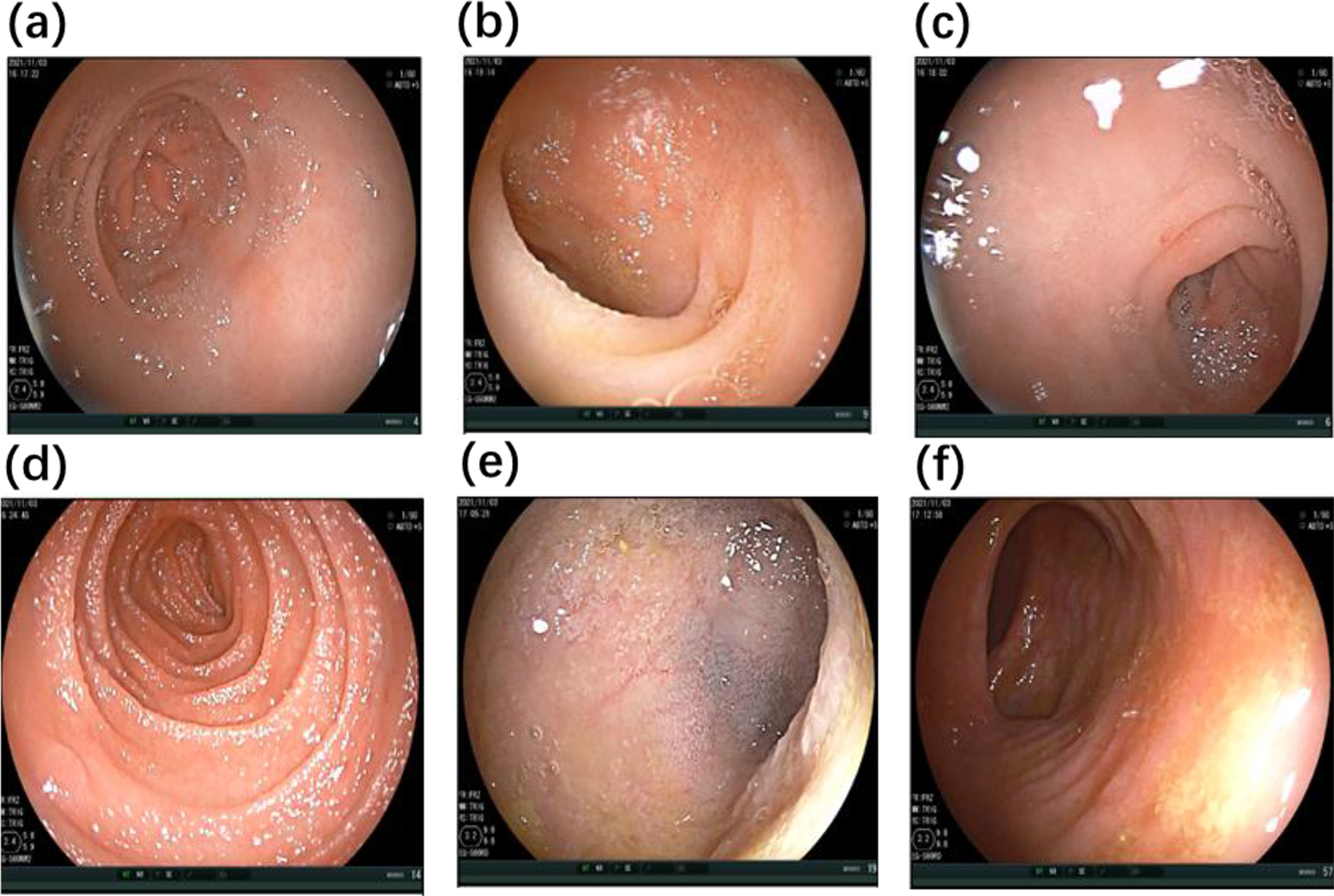
Considering the macroscopic picture of laryngeal edema, we found that submucosal edema localized mainly at the epiglottic and false vocal fold areas, and the true vocal folds were less involved. These findings are similar to the previous observations [9]. Hematoxylin–eosin staining of the laryngeal tissue confirmed the macroscopic observations.
We demonstrated moderate leukocyte infiltration in the C1-INH-HAE patient’s laryngeal tissue. We previously described that the level of several homing chemokines was elevated during HAE attacks [12], which may explain the leukocyte infiltration.
Our patient with type 2 C1-INH-HAE had an elevated C1-INH plasma concentration. In line with this, we demonstrated a slightly more intense C1-INH staining in the C1-INH-HAE patient than in the control patient. The staining pattern showed that endothelial cells, epithelial cells, muscle cells, leukocytes and interstitial space all contain a significant amount of C1-INH, which suggests that—besides the liver as the primary source of C1-INH production—the other tissues/cells are also able to produce and/or store C1-INH. These data are in line with the previous findings [15,16,17,18], which demonstrated that fibroblasts, monocytes and endothelial cells can synthesize C1-INH.
We found an interesting and surprising staining pattern regarding the bradykinin receptors. The literature is controversial in this field: BDKRB2 was considered as the constitutive and BDKRB1 as the inducible bradykinin receptor [19], although in meta-data bases both bradykinin receptors are widely expressed in different tissues (https://www.proteinatlas.org/ENSG00000100739-BDKRB1, https://www.proteinatlas.org/ENSG00000168398-BDKRB2). In our cases, both bradykinin receptors were expressed in the C1-INH-HAE patient and in the control patient, too. The expression of both bradykinin receptors was slightly lower in C1-INH-HAE patient than in the control patient. This suggests that both bradykinin receptors were activated during the HAE attack of our patient.
Our most important and novel observation was that the PAR1 expression was strongly reduced in the C1-INH-HAE patient compared to the control patient. In our previous in vitro study, we showed that PAR1 activation by thrombin, MASP-1 [7] and other plasma serine proteases controlled by C1-INH [8] leads to endothelial cell hyperpermeability. During this PAR1 activation, the receptor is cleaved, and the immunohistochemical reactivity decreases compared to the intact form. These previous findings of ours harmonize with the reduced expression of PAR1 in the C1-INH-HAE patient’s laryngeal edematous tissue, which suggests an important role of MASP-1 and other plasma serine proteases in the pathogenesis of angioedema. Our hypothesis regarding PAR1-cleaving serine protease activation during HAE attacks is further supported by several previous studies, where elevated activation of the coagulation-, complement- and fibrinolytic-system was found [20,21,22]. Based on our observation, both PAR1 and its activator serine proteases (all of which are current therapeutic targets in other diseases) may be considered as new therapeutic targets in HAE if further studies involving tissue biopsy can confirm our results.
Finally, if our observations, derived from the sample of a type 2 C1-INH-HAE patient, are validated, they may well be applicable for the pathomechanism of type 1 C1-INH-HAE and probably (with some restrictions) for that of other BK mediated angioedemas.
In conclusion, studying the molecular and cellular mechanisms in human angioedematous tissues is a necessary future target besides blood plasma analysis. On the one hand, our unique case and novel results confirmed those observed in plasma (e.g., regarding data on C1-INH), on the other hand, it suggested new information about the pathomechanism HAE attack, which seems to be much more complex than we had thought before.


留言 (0)