
記住我
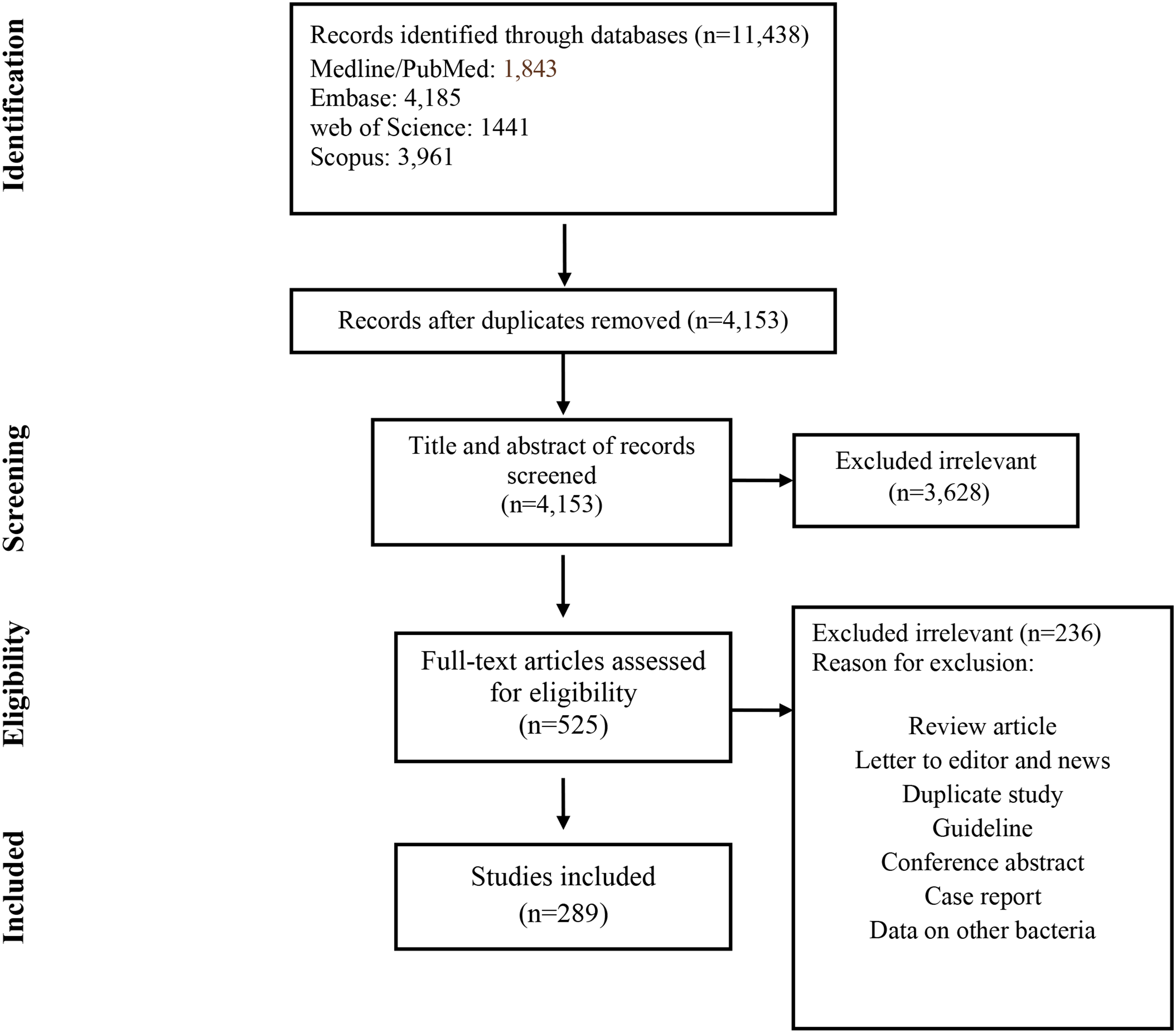
Literature search detected 4509 articles after removal of duplicates (Fig. 1). During screening of titles and abstracts, we excluded 4460 articles, such as reviews and meta-analysis, in vitro studies, studies on animals and humans, such as case reports and observational studies. Moreover, we excluded articles not written in English, as well as comments, recommendations and expert opinions. After full-text assessment, 17 articles were included for quality and quantity analysis.
Fig. 1
Study selection for meta-analysis
All included studies are randomized controlled trials with control group. In the studies, four types of vaccines were evaluated: mRNA vaccines [14,15,16,17,18,19], viral vector vaccines [20,21,22,23,24,25], subunit [26, 27] and inactivated vaccines [28,29,30]. Among these trials, in Brazilian study by Clemens et al. [23] and by Voysey et al. [25] at first dose participants received MenACWY conjugate vaccine as a control, while at second dose they received placebo as a control, whereas in the study from the United Kingdom by Voysey et al. [25] there were two experimental cohorts: in first cohort the participants received low dose of vaccine at first, and a standard dose as a second dose. While in the second cohort, participants received two standard doses, and both control groups received MenACWY conjugate vaccine. Two studies were conducted in South Africa [22, 26], one study in South Africa, Brazil, and the United Kingdom [25], one study in Indonesia [29], one study in Russia [20], one study in Brazil [23], one in the United Kingdom [27], one in Turkey [30], one in the United States, Chile, and Peru [24], one in South Africa, Argentina, Chile, Brazil, Colombia, Peru, Mexico, and the United States [21], one in the United Arab Emirates, Jordan, Egypt and Bahrain [28], one in the United States, Argentina, Brazil, South Africa, Germany, and Turkey [18], and five in the United States [14,15,16,17, 19]. Additionally, three studies were conducted on adolescents [17,18,19]. Table 1 shows the characteristics of included studies.
Table 1 Characteristics of included RCTsQuality assessmentRisk of bias was prepared for 17 included RCTs. According to our risk of bias assessment, 2 of the analyzed studies represent high risk of bias; while remaining 15 studies represent low risk of bias. Additional file 1 shows the summary of risk of bias.
The efficacy of vaccines against symptomatic COVID-19 infectionsBecause of high level of heterogeneity, the subgroup analysis of symptomatic COVID-19 incidences from clinical trials of different types of vaccines compared to control was performed (Fig. 2). The analysis found that vaccination decreased the risk of symptomatic COVID-19 infection by 81% (RR = 0.19; 95% CI [0.13; 0.27]; p < 0.0001). The lowest level of risk of symptomatic COVID-19 infection was noted after full vaccination with mRNA vaccines and equals 0.08 (95% CI [0.07; 0.09]) without heterogeneity, while in case of viral vector vaccines the risk was 0.31 with considerable heterogeneity (95% CI [0.23; 0.41], I2 = 80%). Similar effects were obtained after vaccination with inactivated and subunit vaccines: 0.24 (95% CI [0.18; 0.32], I2 = 9%) and 0.20 (95% CI [0.05; 0.78], I2 = 87%), respectively. However, the risk of symptomatic COVID-19 after vaccination with one dose vaccine (Ad26.COV2.S) was higher after 28 days after vaccination than after 14 days following the vaccination: 0.33 (95% CI [0.27; 0.41]) and 0.40 (95% CI [0.30; 0.53]), respectively. In adolescents, full vaccination with mRNA-1273 vaccine decreased the risk of symptomatic COVID-19 infection by 95% (RR = 0.05, 95% CI [0.00, 1.00]), while BNT162b2 vaccine decreased by 97% (RR = 0.03, 95% CI [0.00, 0.49]).
Fig. 2
The efficacy of COVID-19 vaccines for preventing symptomatic COVID-19. *Studies in adolescents; **study in adolescents and adults; $first dose was low, while second dose was standard, the United Kingdom; $$both doses were standard, the United Kingdom; $$$both doses were standard, Brazil; #observation at least 14 days after vaccination; ##observation at least 28 days after vaccination
The efficacy of vaccines against severe COVID-19 infectionsOnly 10 studies were included in the subgroup analysis, because other studies reported no cases of severe COVID-19. (Fig. 3). Overall, full COVID-19 vaccination decreased the risk of severe COVID-19 infection by 91% (RR = 0.09; 95% CI [0.04; 0.20]; p < 0.0001, I2 = 54%). Among vaccines, the lowest risk of severe infection course of COVID-19 was 0.04 (95%CI [0.01; 0.25]) after vaccination with mRNA vaccines. Moreover, the risk of severe COVID-19 infection with one dose vaccine (Ad26.COV2.S) was lower after 28 days after vaccination compared to risk after 14 days following the vaccination: 0.15 (95% CI [0.06; 0.37]) and 0.23 (95% CI [0.13; 0.42]), respectively.
Fig. 3
The efficacy of COVID-19 vaccines for preventing severe COVID-19. #Observation at least 14 days after vaccination; ##observation at least 28 days after vaccination
The efficacy of vaccines against hospitalization related with COVID-19 infectionsWe analyzed the efficacy of different types of vaccines in preventing hospitalization related with COVID-19 infections (except mRNA vaccines—no data has been reported), which was 93% (RR = 0.07, 95% CI [0.03; 0.17], p < 0.0001) without heterogeneity (Fig. 4a). The highest risk of hospitalization was observed after viral vector vaccine ChAdOx1 nCoV-19 and subunit vaccine NVX-CoV2373, and equals 0.33 (95% CI [0.01; 7.98] and 0.33 (95% CI [0.01; 8.18]), respectively.
Fig. 4
The efficacy of COVID-19 vaccines for preventing hospitalization and death related to COVID-19. a preventing hospitalization related to COVID-19; b preventing death related to COVID-19; #observation at least 14 days after vaccination; ##observation at least 28 days after vaccination
The efficacy of vaccines against death related with COVID-19 infectionsMeta-analysis assessing the impact of COVID-19 vaccines on COVID-19 mortality rate was carried out in 4 clinical trials: mRNA-1273 [15, 16], ChAdOx1 nCoV-19 [23] and Ad26.COV2.S [21] vaccines (Fig. 4b). Other studies haven’t reported deaths related to COVID-19 during the study. Full vaccination may prevent death by 82% (RR = 0.18, 95% CI [0.03; 0.15], p = 0.0298) without heterogeneity.
The efficacy of vaccines against different variants of SARS-CoV-2Additionally, we analyzed the efficacy of several vaccines against B.1.1.7, B.1.351 variants of SARS-CoV-2 as well as against Brazilian lineages of SARS-CoV-2 (Fig. 5). Overall, full vaccination may decrease the risk of infections by 64% (RR = 0.36; 95% CI [0.25; 0.53], p < 0.0001, I2 = 45%). Among two analyzed vaccines (NVX-CoV2373 and ChAdOx1 nCoV-19) against B.1.1.7 variant of SARS-CoV-2, the risk of infections was the lowest after NVX-CoV2373 vaccine administration: 0.14 (95% CI [0.07; 0.29]. The efficacy of three vaccines (BNT162b2, NVX-CoV2373 and ChAdOx1 nCoV-19) were analyzed against B.1.351 variant of SARS-CoV-2. BNT162b2 vaccine may prevent the infection rate by 94% (RR = 0.06; 95% CI [0.00; 0.96]). Moreover, the risk of infections with Brazilian lineages of SARS-CoV-2 after ChAdOx1 nCoV-19 vaccine was 0.12 (95% CI [0.02; 0.98]) for B.1.1.33 variant; 0.28 (95% CI [0.14; 0.55]) for B.1.1.28 variant; 0.32 (95% CI [0.22; 0.46]) for P.2 variant and 0.38 (95% CI [0.13; 1.05]) for P.1 variant.
Fig. 5
The efficacy of COVID-19 vaccines against different variants of SARS-CoV-2
The efficacy of COVID-19 vaccines against COVID-19 infections according to age groupsAccording to 8 articles, we analyzed the efficacy of COVID-19 vaccines within age groups, which equaled 83% (RR = 0.17; 95% CI [0.13; 0.23], p < 0.0001, I2 = 87%) (Fig. 6). Moreover, the risk of the infection was slightly lower in adults compared to elderly: 0.16 (95% CI [0.11; 0.23]) and 0.19 (95% CI [0.12; 0.30]), respectively. When comparing both mRNA vaccines (BNT162b2 and mRNA-1273), the efficacy of preventing COVID-19 infection equaled 90% within all age groups. Similar result was observed after vaccination with viral vector vaccine rAd26 and rAd5 and subunit vaccine NVX-CoV2373 in both age groups. Interestingly, ChAdOx1 nCoV-19 vaccine had the better efficacy in elderly cohort \((\ge\) 65 years), because the risk was 0.18 (95% CI [0.06; 0.49]) compared to 0.28 (95% CI [0.21; 0.38]) in cohort 18–64 years.
Fig. 6
The efficacy of COVID-19 vaccines for preventing COVID-19 infection according to age groups. #Observation at least 14 days after vaccination; ##observation at least 28 days after vaccination
Publication biasAdditional file 2 shows the funnel plots for all outcomes: symptomatic COVID-19, severe COVID-19, hospitalization related with COVID-19, death related to COVID-19, different lineages of SARS-CoV-2, and according to age groups. Additionally, Peters’ regression test was performed to calculate publication bias for these outcomes. The results of Peters’ regression test showed that there was no evidence of publication bias for the association of COVID-19 vaccination and symptomatic (p = 0.1686), severe COVID-19 (p = 0.6302), hospitalizations related with COVID-19 (p = 0.9579), deaths related to COVID-19 (p = 0.2800), and against different lineages of SARS-CoV-2 (p = 0.7430), according to age groups (p = 0.5421), because p for outcomes was greater than 0.05.
留言 (0)