CL is recognized as one of the most frequent skin diseases occurring after traveling in endemic areas [14]. The diagnosis may be also a challenge because unusual presentations can occur [15] and parasitological detection, which is often the most available method, usually relies on technical expertise. Taking all this into consideration, travel clinics and referral centers must be prepared to offer not only a prompt but an accurate diagnosis.
All the cases presented here were positive for Leishmania. As a laboratory in a non-endemic area, we continue promoting the use of different methods, eluding subjectivism or inexperience, so parasitological and molecular tools are currently utilized during the diagnostic process. It is known that a combination of laboratory methods increased the sensitivity for diagnosis and also provides the possibility to identify the infecting species [4].
Our results indicated that each case had at least one positive parasitological result whereas molecular detection of DNA was possible in all of them, using more than one target (hsp70 and rDNA genes) which makes the final diagnostic robust. It is not surprising that weak DNA product had been obtained after PCR-F in case 17–03, due to the amplicon’s size. While PCR-N is 593 bp length, PCR-F is 1286 bp, a feature that can affect diagnostic sensitivity, as it has been previously reported by our group [16].
In regards to typification, the species identified corresponded with those reported in the countries where the infected persons stayed, and the results were concordant according to the RFLP scheme used. The results of PCR-F/RFLP-BccI in case 17–03 are remarkable. According to the hsp70 and hsp20 sequences analysis, L. panamensis and L. guyanensis were previously considered as a monophyletic group [17]. Nevertheless, both of them could be distinguished using BccI as a restriction enzyme for PCR-F product [18], which was validated in the differentiation of isolates and clinical samples from some endemic countries [19, 20]. However, the pattern obtained after PCR-F/RFLP was not unequivocal, as it showed bands expected for both entities: L. panamensis and L. guyanensis. Considering that L. panamensis have not been reported in the territories visited by patient 17–03, where L. guyanensis, L. braziliensis and L. amazonensis are main species involved in CL [21], one possible explanation could be that this patient suffering of a mixed infection of L. guyanensis and other species. Another possibility is that the pattern observed corresponds to a different L. guyanensis population, agreeing with the significant genetic diversity associated with this species reported, for example, infecting miners in that country [22, 23]. As the detection of polymorphism within each species varies according to the genetic markers used, it is possible that further studies, using multilocus sequencing, could shed light on this matter.
Concerning treatment, different protocols were used mainly due to availability of drugs (due to supply chain), since leishmaniasis is a non-endemic diseases with sporadic cases. Then, the selected drug was personalized for each case according dosage and duration of therapy, the clinical aspect of the lesions, and the response of each patient. In addition, a strict follow up of clinical parameters were performed in all cases. We acknowledge that international guidelines exist [24]; specially in non-endemic settings as Cuba where the medical expertise treating leishmaniasis is limited. However, the lower accessibility to drugs in the international market impact into the treatment management. In this context, some alternatives of treatment as were presented, such as the use of a lipid complex of amphotericin B produced in India.
Nevertheless, is evident that for CL a systemic treatment and drugs with different effectiveness against Leishmania is considered mandatory. In this regard, in the analyzed cases, drugs targeting ergosterol were used, including amphotericin B that binds to membrane sterols, forming complexes that arrange into ion channels and increase membrane permeability [25] or fluconazole that interfere with ergosterol biosynthesis by inhibiting the C-14 demethylation of sterols in Leishmania [26]. In addition, the use of lipid complex of amphotericin B (Ampholip®) represents an advantage, such as: (i) deliver the drug on-site, (ii) minimizing the dosage by many folds, and (iii) reducing the side effects related to drug toxicity, which is preferable over using conventional amphotericin B [27].
Althoutgh cure was achieved for all treated patients, response was very different. However, we can not determined the real causes of this due to the influence of different factors; among them: (i) time elapse between infection and treatment start, (ii) severity of disease when treatment started, (iii) clinical characteristics related with single/multiple or nodule/ulcerated lesion, and (iv) immunological status of patients. Nevertheless, longer and complex treatment was administered to L. braziliensis (case 17–01). It is known that L. braziliensis is the main causal agent of CL and MCL in the Americas [28] with the greatest relative abundance in Colombia and frequently results in therapeutic failure [29]. Recently, a study to determine drug susceptibility profiles of amphotericin B and fluconazole in cultured isolates of Old World and New World Leishmania spp., showed reduced susceptibility to drugs against New World species compared with Old World strains. In particular, some clinical isolates of L. braziliensis and L. panamensis displayed lower susceptibility compared with reference strain [30]. Nevertheless, therapeutic response is highly variable across the American continent, which could relate with virulence or aggressive behaviour of cinculating strain [31]. In addition, probably spontaneous resolution in patients instead of treatment-dependent responsed is not depreciable.
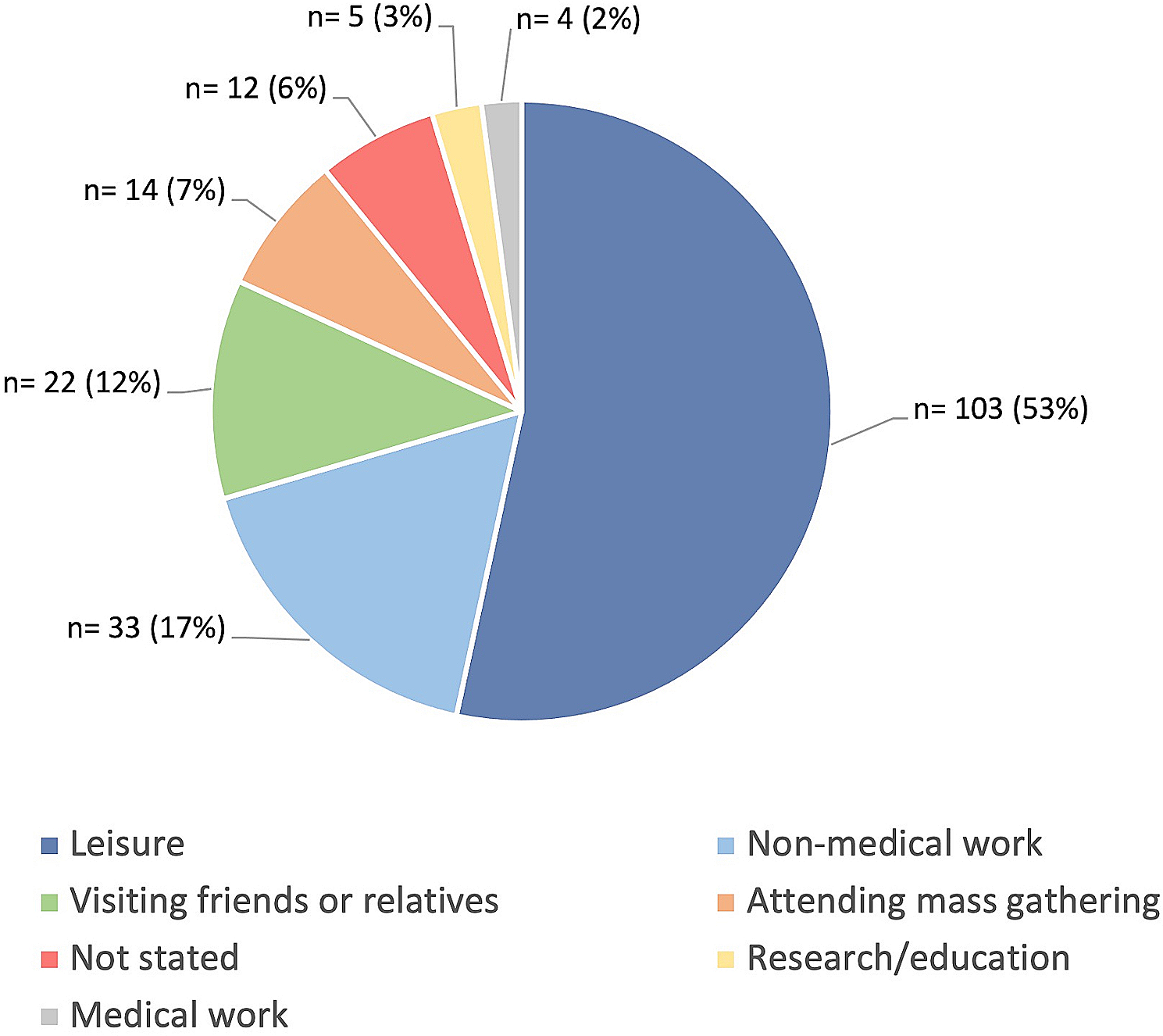
According to World Health Organization (WHO), leishmaniasis remains as a group of diseases without current control measures. Prophylactic vaccines do not exist nor vector control is effective in most of the settings with a predominant peridomiciliary transmission where these parasitoses are endemic [32, 33], which makes harder the task. Besides, it has been recently recognized that “in an interconnected world, change is occurring across social, environmental and climatic scales affecting human, animal and natural systems” [32] and leishmaniasis is not an exception. Among the multiple epidemiological features surrounding the possible occurrence of leishmaniasis, the human movement between low- and high-risk areas is also important, mainly when uncontrolled displacements take place. In this study, 4 out of 5 cases departed from a country where Leishmania is not present, to enter a whole region where the disease is highly distributed [1, 6, 34]. Even more, some of the countries with the highest number of CL cases reported in Latin America, such as Brazil, Peru, Colombia, and Panama [6], were intruded on by most of these persons on their route, increasing, in particular, their risk. As it was described for all the cases (except 17–05), the persons infected traveled rural areas unsafely and slept outdoors without protection. All five cases spent partial or complete journeys in the forest or the jungle; without protecting from insect bites capable of transmitting leishmaniasis or another vector-borne disease. Remarkably, the interviews corroborated that none of the travelers knew about the disease nor other probable infections transmitted by vectors, except for dengue. Therefore, unknowingly they disregarded that possibility and displaced under inappropriate protection measures and totally vulnerable to a serie of transmissible diseases. These cases can serve as an example of the serious risks assumed by persons that decide to travel, in particular, by irregular routes, whatever be the reason.
In Cuba, there is currently no evidence about the presence of recognized Lutzomyia species that could transmit Leishmania parasite [35]. However, considering the ecology of sandflies, it is unlikely that phlebotomus could enter the country with travelers, adapt to new ecology conditions and expand their habitat. Although the possibility of the disease spreading certainly is low, notification of imported cases is necessary in the age of globalization.
A recent retrospective analysis between 2006 and 2016 showed that in 10 years only 5 patients with positive Leishmania infection were confirmed out from 16 suspicious cases. Thus, it may cautiously be assumed to our best knowledge that this series of 5 cases during 2017 (1 year), constitute the great majority of imported cases/year diagnosed and treated in Cuba. In several non-endemic countries, the number of cases has increased in the past decade. In particular, some reports from Europe, like Belgium [36], Poland [37], and Sweden [4], are showing an increase in cases imported from America. In parallel, the human movement towards of the island, not only causes an increment in leishmaniasis (as described herein), same challenge has been also evidenced in other non-endemic parasitic diseases such as trypanosomiasis [38] and malaria [39].



留言 (0)