
記住我


Fifteen patients were available for this study (twelve men and three women; see Table 1) who had received both [18F]F-FDG PET/CT and [68 Ga]Ga-FAPI-46 PET/CT between March and November 2020. All patients had histologically confirmed HNCs prior to imaging and had been referred by the local multidisciplinary board for radio(chemo-/immuno)therapy, in most cases (14 out of 15 cases) because they had reached inoperable stages of disease (UICC stages III and IV). One patient had a resectable tumor (laryngeal carcinoma, cT2 cN0) but preferred radiochemotherapy over operation for better functional preservation of the voice. Most patients (93.3%) had a histopathological diagnosis of SCC, and 33.3% were HPV-positive.
Table 1 Patient characteristicsBiodistributionFor [68 Ga]Ga-FAPI-46, the highest uptake was observed in the primary tumor region (n = 15, median SUVmax 14.8, range: 9.26–26.6) with the second highest in the nodal metastasis (n = 23) (median SUVmax 9.47, range 1.83–24.9). Uptake in visceral metastasis (n = 7) was 7.05 (median SUV max, range: 1.8–25.0) while in bone metastasis (n = 3), it was 7.45 (median SUVmax, range: 4.0–14.2). Background uptake was assessed in liver (median SUVmean 1.13, range: 0.4–3.03) and in the bloodpool (median SUVmean 1.49, range: 0.97–2.56).
For [18F]F-FDG, the highest uptake was observed in the primary tumor (median SUVmax 13.4, range: 5.68–21.9) and next highest in lymph node metastasis (n = 23) (median SUVmax 6.17, range 1.73–20.9).
The median SUVmax in visceral metastasis (n = 7) was 5.57 (range: 2.62–11.1) while in bone metastasis (n = 3), it was 2.59 (median SUVmax, range: 1.41–2.75).
Background uptake in the liver was 2.58 (median SUVmax, range 1.35–3.88) on FDG and 1.13 (median SUVmax, range 0.4–3.03) on [68 Ga]Ga-FAPI-46 PET/CT. The uptake in the mediastinal bloodpool was 2.12 (median SUVmax, range 1.26–2.88) for FDG and 1.49 (median SUVmax, range 0.97–2.56) for FAPI. Table 2 shows biodistribution measurements for [68 Ga]Ga-FAPI-46 PET/CT and FDG PET/CT. Tumor-to-background ratios are presented in Table 3 and Fig. 1.
Table 2 Tracer uptake (SUVmax) in tumor lesionsTable 3 Tumor-to-background ratio (TBR)Fig. 1
Uptake measurements in 49 lesions. Left part: SUVmax by site for FDG (blue box) and FAPI (yellow box) in tumorous lesions. Right part: Tumor-to-background (TBR) ratios (SUVmax/SUVmean) for FDG (median 2.94; blue box) and FAPI (median 8.70; yellow box; p < 0.001). The statistical comparison was performed by a Wilcoxon paired rank test. NS. not significant; ***p < 0.001.
Lesion-Based Comparison of [18F]F-FDG PET/CT and [68 Ga]Ga-FAPI-46 PET/CTA total of 49 lesions were recorded. Of these, 40 (82%) were FDG+ and 41 (84%) were positive by FAP+. There were five (10%) FAP+/FDG− lesions and four (8%) FAP−/FDG+ lesions. This may be the result of tumor heterogeneity, since FAP displays CAFs and FDG tumor metabolism. Thus, [68 Ga]Ga-FAPI-46 PET/CT may not always be superior to [68F]F-FDG PET/CT as an imaging technique for all different tumor entities and differentiation grades. While knowledge of [68 Ga]Ga-FAPI-46 PET/CT remains incomplete, we recommend imaging with both tracers to obtain comprehensive diagnostic information. Disease stage identified by FAPI PET/CT was mostly concordant with FDG PET/CT. Compared to conventional imaging alone, five patients (33%) were upstaged following imaging by FAPI-PET/CT. All of these had visible lesions on FDG PET/CT as well.
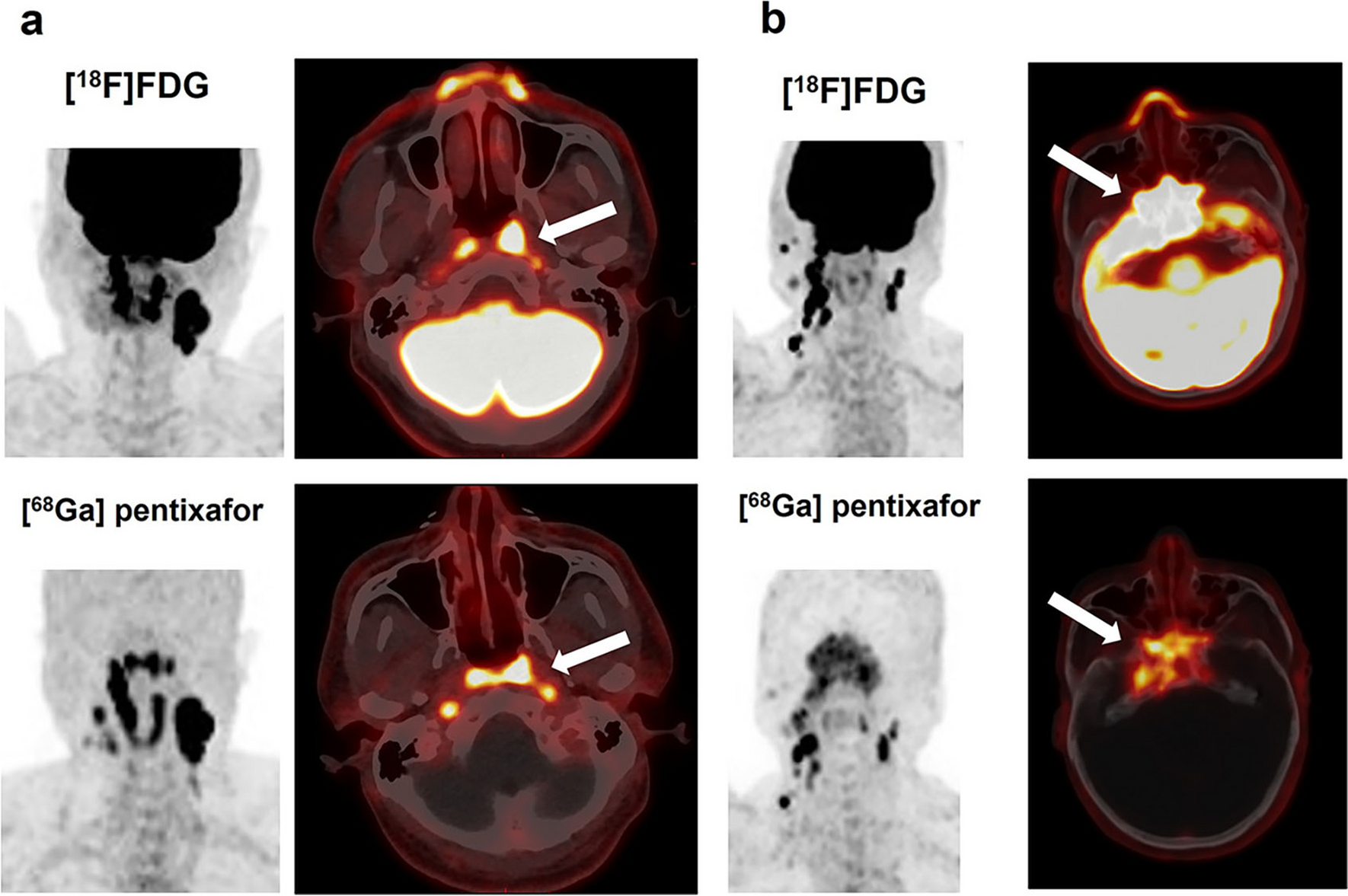
In one case, a patient with nasopharyngeal cancer was upstaged with newly emerged nodal metastasis on both sides of the neck, noticed only in the FAP scans (see Fig. 2). [68 Ga]Ga-FAPI-46 PET/CT also revealed one cervical lymph node metastasis in close proximity to the cervical spinal cord (at C4 level) that would have been missed in the [18F]F-FDG scans. Standard cervical radiation would have left out this tumor manifestation with a subsequent high risk of recurrent or progressive disease in that region.
Fig. 2
Cervical nodal metastasis with high FAPI uptake and low FDG uptake maximum intensity projections (A, B) and axial fusion images of a 73-year-old male with nasopharyngeal cancer prior to radiation therapy. The patient was upstaged with newly emerged nodal metastasis on both sides of the neck, noticed only in the FAP scans (C, D; white arrows). [.68 Ga]-FAPI PET/CT also revealed one cervical lymph node metastasis in close proximity to the cervical spinal cord (at C4 level) that would have been missed in the FDG-scans (E, F; yellow arrows).
In two patients, we observed unspecific focal FAP-uptake in bone (in the clavicle and in a patient’s rib, see Fig. 3). As there was no correlation in the CT scan and no [18F]F-FDG uptake, we decided not to upstage these patients solely on the basis of the bone uptake in the FAP-scans.
Fig. 3
False-positive uptake in FAP-scans in a patient’s left rib. Maximum-intensity projections and axial fusion images of a 37-year-old male with nasopharyngeal cancer prior to radiation therapy. The patient had FAP uptake in the left 9th rib rated as benign (red arrow). Neither the FDG scan nor conventional imaging was suggestive of bone metastasis.
Target Volumes (GTVs)Target volumes were defined using VARIAN Eclipse software. Conventionally created GTVs (CONV-GTV, based on imaging information from MRI and CT) took up a median volume of 37.7 ml (range 5.3–80.3) (see Table 4; Fig. 4). Contoured GTVs based on imaging information from the FDG PET/CT (FDG-GTV; median 42.5 ml, range 6.5–98.1) were not significantly different to the CONV-GTVs (p = 0.95). The GTV created on the basis of [68 Ga]Ga-FAPI-46 PET/CT (FAPI-GTV; median 57.3 ml, range 11–107 ml) was significantly larger than CONV-GTV with a median increase of 9.2 ml (range − 12.0 to 58.1; p = 0.003) and FDG-GTV with a median increase of 7.2 ml (range − 12.0 to 66.6; p = 0.024). There was no case in which FAPI-GTV was smaller than the CONV-GTV. A few patients had [68 Ga]Ga-FAPI-46-uptake in their primary tumor regions, which would not have been covered by the CONV-GTV.
Table 4 Volumetric comparison of different gross tumor volumes (GTV)Fig. 4
GTVs (ml) based on different imaging methods in 15 patients Grey box: GTV based on conventional imaging, mean volume: 39.2 ml (SD 20.3), yellow box: GTV based on FDG PET/CT, mean volume: 41.1 ml (SD 29.1) and blue box: GTV on the basis of FAPI PET/CT, mean volume: 57.9 ml (SD 33.4) (see Table 1). The statistical comparison was performed by a Wilcoxon paired rank test. NS not significant; *p < 0.05; **p < 0.01.
We observed a greater extent of FAP-uptake in primary tumor sites with higher tumor-to-background ratios and in some cases detected additional (contralateral) lymph nodes as well as further suspicious distant lesions.
Radiotherapy GTV and OutcomeFAPI-based GTVs were considered in ten patients (67%). Reasons for findings not being recorded as FAPI-positive lesions were FAPI-PET signal beyond morphological tumor volume considered as halo (n = 2), benign uptake surrounding tracheal stoma (n = 1), low FAPI-PET signal without MRI correlate (n = 1), and unclear pulmonary lesions confirmed as metastasis in a follow-up scan (n = 1). Final GTVs used for radiotherapy demonstrated very strong correlation with FAPI-GTV (rho = 0.72; p = 0.004), strong correlation with FDG-GTV (rho = 0.56; p = 0.0134), and strong but not statistically significant correlation with CONV-GTV (rho = 0.48; p = 0.0564, see Table 4). Outcome data is limited by heterogenous follow-up, as aftercare was not always performed at our institution. However, a minimum of 6 months of follow-up was available for all patients. After a median of 14.8 months of documented follow-up, five (33%) patients experienced progression. Of these, all patients had out-of-field progression at a median of 10.1 months. Only one patient had progression in a FAPI-positive region at baseline 4.5 months after the start of RT. This was a pulmonary lesion positive in both FDG- and FAPI-PET, retrospectively confirmed as lung metastasis. Three patients (20%) died during follow-up.
留言 (0)