
記住我

Sexually transmitted infection (STI) is an important public health problem worldwide that affects approximately 498.9 million people and is associated with high morbidity and mortality rates (Francis et al., 2018; Mohammed et al., 2016; Ramjee et al., 2015). Causes of STI include penile–vaginal intercourse at an early age, multiple sexual partners, unprotected penile–vaginal intercourse experiences, and inconsistent or incorrect condom usage (Young et al., 2018).
Condoms are included in the World Health Organization's list of essential items in the reproductive health and perinatal care category (World Health Organization, 2019). Data show that condoms effectively prevent 70–90% of HIV infections when used consistently and correctly (Siegler et al., 2012; Smith et al., 2015; Westercamp et al., 2010; Yamamoto et al., 2018), yet the rate of condom use among sexually active men varies between 55% and 90% (Lachowsky et al., 2016; Paul et al., 2019; Smith et al., 2015). Although the most effective method of preventing STI is the consistent and correct use of condoms, it is clear that the rate of condom usage is not at the desired level worldwide (Francis et al., 2018; Selvey et al., 2018).
The Multi-Factor Attitude toward Condoms Scale (MFACS) is a reliable and valid instrument to measure individuals' attitudes toward condoms (Reece et al., 2010) that has been used in multiple studies of strategies to increase condom use in at-risk populations (Choi et al., 2020; Hollub et al., 2011); however, a Turkish version of the MFACS has not been developed and validated. This omission is significant because condom use among married couples in Turkey has been reported to be as low as 19.1% (Turkey's Demographic and Health Survey, 2018). The purpose of this study was to translate the MFACS into Turkish and test its reliability and validity in a sample of Turkish outpatient clients.
Methods Ethical ApprovalBefore the study was conducted, ethical approval was received from the Ethics Committee of the institution that served as the study's setting (approval number: 46418926-19/111). After institutional ethics approval, the approval of the Medical Specialist Education Board was obtained from the Provincial Directorate of Health. All participants gave written informed consent.
SettingThe study was conducted in the Obstetrics and Gynecology and Urology outpatient clinics of a tertiary education and research hospital located in Ankara, Turkey.
SampleEligibility criteria included age 18–49 years, sexually active, and ability to speak and read Turkish. The sample size was calculated to ensure adequate power for the study analyses. Because the MACFS consists of 14 items, we sampled 20 participants (10 men and 10 women) for each item to meet the minimum requirements for conducting factor analysis (10 participants per item; Lyu et al., 2017; Norman & Streiner, 2008; Tsang et al., 2017). Additionally, we oversampled to control for a projected attrition rate of 20%, for a final sample size of 336 (168 men and 168 women). Although the retest sample size was planned to include at least half of the participants, the vast majority of the participants invited to retest declined, which resulted in a retest sample size of 56 participants who completed the questionnaire at baseline and 2 weeks later. The 56 participants who participated in the retest were considered sufficient to test the reliability of the scale according to published guidelines (Polit, 2014; Tabachnick & Fidell, 2007).
Instruments Demographic characteristicsThe authors developed an 11-item demographic instrument that collected data related to gender, age, education, marital status, and economic status (Reece et al., 2010; Wang et al., 2019; Wulandari et al., 2018).
Sexual knowledge and experienceThe authors developed an 18-item knowledge and experience questionnaire that measured age at first penile–vaginal intercourse, number of sexual partners, knowledge of STI, and knowledge and experiences regarding correct condom usage. The items measured variables previously shown to correlate with condom attitudes (Reece et al., 2010; Wang et al., 2019; Wulandari et al., 2018).
Multi-Factor Attitude toward Condoms ScaleThe MFACS was developed by Reece et al. (2010) to measure individuals' attitudes toward condoms. The MFACS is based on cognitive and affective dimensions underlying the conceptualization of attitudes and consists of 14 items across three subscales: perceived effectiveness (3 items), affective (6 items), and manageability (5 items). Each item on the MFACS is scaled as a seven-point semantic differential that assesses condom as an object and contains opposite pole adjective clauses (Figure 1). The MFACS yields both total and subscale scores; each item is reverse scored before calculating total and subscale scores. The total MFACS score ranges from 14 to 98 and is calculated by summing the three subscale scores. Higher total MFACS scores and subscale scores indicate more positive attitudes toward condoms.
 Figure 1.:
Figure 1.: Multi-Factor Attitude toward Condoms Scale 7-point semantic scale (Reece et. al., 2010).
ProceduresAll individuals who came to Obstetrics and Gynecology and Urology outpatient clinics for any reason between February and June of 2019 were invited to participate in the study. Informed consent was obtained from participants who met the eligibility criteria. After the first survey administration, the survey was readministered 2 weeks later to the 56 participants who agreed to participate in the retest (28 women and 28 men).
Forward and Backward Translations ProcessWe used as a standard method to translate the English version of the MFACS to Turkish (Beaton et al., 2000). The forward and backward translations process was conducted in six stages.
Stage 1Three parallel forward translations from English to Turkish were conducted by three native Turkish speakers who were fluent in English and who were specialists in urology, women's health and gynecology, and public health nursing. All specialists prepared a report for their translations, including their rationale for their choices.
Stage 2The three forward translations and reports developed in Stage 1 were compared by three different specialists (one in women's health and gynecology, one in public health nursing, and one in Turkish language) to explore discrepancies in the chosen words and the rationale for these choices. The specialists discussed wording and reached consensus on the Turkish translation.
Stage 3The Turkish translation developed in Stage 2 was translated backward to English by three different specialists from Stages 1 and 2, thus ensuring blinding to the previous translations. The specialists held expertise in urology, women's health and gynecology, and public health nursing. All received high scores on the national English examination and had previously lived in the United States. The specialists evaluated the translation for content fidelity to the original version and reached a consensus.
Stage 4The semantic and cultural equivalence of the back translation to the original scale was examined by the authors and the nine specialists who participated in Stages 1 through 3. To assess semantic equivalence, words were evaluated for equivalence of meaning and grammar. To assess cultural equivalence, the expressions of the back translation were revised and cultural equivalence to the original text was ensured. Finally, the authors and all the specialists reviewed all forward and backward translations and reached a consensus on a prefinal version for field testing.
Stage 5The prefinal version of the scale was administered to 30 clinic patients. The authors interviewed each patient about what they thought was meant by each item and the chosen response. They were also asked if the questions were easy to understand and if the wording was unfamiliar, uncommon, or uncomfortable. Their responses were recorded and transcribed and assessed in Stage 6.
Stage 6The authors and nine specialists evaluated patient responses from Stage 5 and, after reaching consensus, revised the Turkish translation accordingly.
Statistical AnalysisThe normality of the distributions of total and subscale scores was analyzed using the Kolmogorov–Smirnov test. Validity assessments included calculation of the content validity index and explanatory factor analysis for construct validity. Reliability was assessed by the item-total correlation, Cronbach α value, item analysis, and 2-week test-–etest correlation analysis.
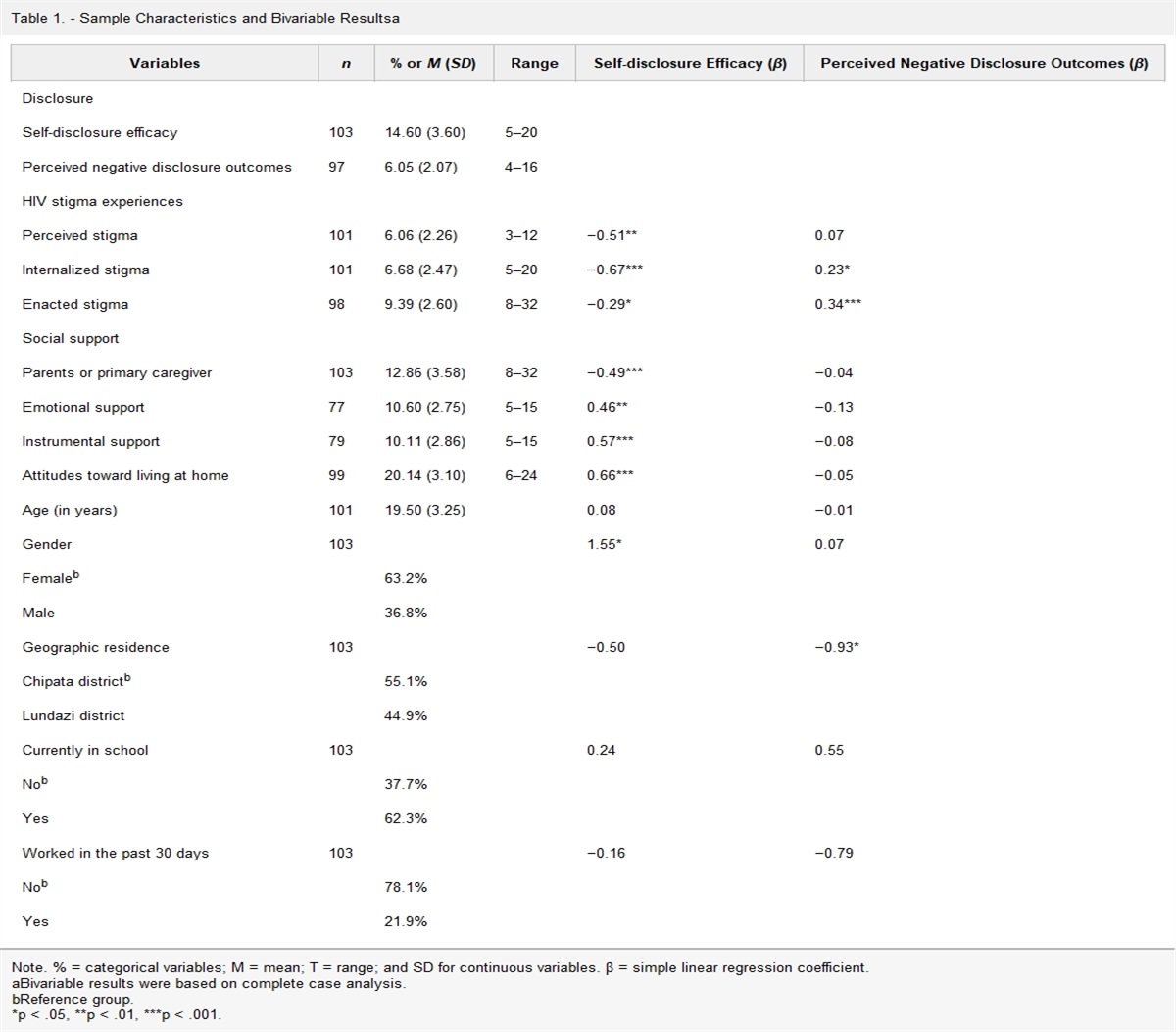
Results Characteristics of the ParticipantsThe mean age of the female participants (n = 168) was 32.73 ± 6.93 years, whereas the mean age of the male participants (n = 168) was 31.02 ± 7.67 years. Most participants were married (n = 243; 71.7%). Female participants were more likely to report monogamy than males (88.7% vs. 28%) as measured by number of lifetime sexual partners (Table 1).
Table 1. - Participants' Demographics and Sexual Knowledge and Experience (N = 336) Variables Female (n = 168) Male (n = 168) n % n % Education status (years) ≤8 45 26.8 31 18.5 >8 123 73.2 137 81.5 Marital status Married 158 94.0 85 50.6 Single 10 6.0 83 49.4 Level of income (TL) <3,000 80 47.7 82 48.8 ≥3,000 88 52.3 86 51.2 Have you received previous training on STI? Yes 103 61.3 110 65.5 No 65 38.7 58 34.5 How many different people have you ever had penile–vaginal intercourse with? I do not want to answer 15 8.9 43 25.6 Monogamous 149 88.7 47 28.0 Two people and more 4 2.4 78 46.4 Do you use condoms for family planning method? Yes 61 36.3 62 36.9 No 107 63.7 106 63.1 Do you know how to use condoms in the right way? Yes 114 67.9 163 97.0 No 54 32.1 5 3.0 Have you used condoms in your last sexual relationship? Yes 74 44.0 96 57.1 No 94 56.0 72 42.9Note. STI = sexually transmitted infection; TL = Turkish lira.
To assess content validity, the Turkish MFACS items were assessed by 10 bilingual academicians from Women's Health and Gynecology and Public Health Nursing departments from 10 different state universities in various Turkish cities. The academicians compared the original item in English and its Turkish translation and scored the relevance and scope of the translation as 1 = not relevant, 2 = slightly relevant, 3 = quite relevant, or 4 = highly relevant. Using the Lawshe technique, a Content Validity Index value of 0.98 for the translated MFACS was obtained (Ayre & Scally, 2014; Sousa & Rojjanasrirat, 2011). No items were removed from the scale as a result of the content validity assessment.
Construct Validity Explanatory factor analysisTo determine the sampling adequacy of the data set for factor analysis, Kaiser–Meyer–Olkin and Bartlett tests were performed. The sampling adequacy was confirmed with a Kaiser–Meyer–Olkin test value of 0.865 (χ2 of 3,072.182; p = .001). The MFACS explanatory factor analysis performed with oblimin with Kaiser normalization rotation yielded eigenvalues greater than 1, and three factors were identified that explained 71.0% of the total variance (Table 2). The three subscales had factor loads that ranged between 0.67 and 0.91. It was determined that the ninth item in the affective subscale of the original MFACS (“I would describe a condom as neat/messy”) loaded on Factor 2, whereas the 14th item in the manageability subscale of the original MFACS (“I would describe a condom as easy/hard to use”) loaded on Factor 1 (Table 3). All Factor 3 items matched the perceived effectiveness subscale (Figure 2).
Table 2. - Explanatory Factor Analysis Factors Eigen value Variance (%) Factor 1 3.970 28.35 Factor 2 3.308 23.63 Factor 3 2.662 19.01 Total 9.94 71.0Note. STI = sexually transmitted infection.
 Figure 2.:
Figure 2.: Explanatory factor analysis: scree plot.
Reliability Item analysis and internal consistencyThe item-total correlation was assessed using Pearson correlations. Each item showed a positive correlation to the total scale ranging from 0.18 to 0.66. The total scale Cronbach α was .82 and did not fall below .80 when any item was removed. Thus, all 14 items were retained (Table 4).
Table 4. - Item-Total Correlation Analysis MFACS Item-Total Correlation If Item Deleted Cronbach α Item 1 Effective/not effective at preventing pregnancy .56 .80 Item 2 Effective/not effective at preventing STIs .60 .80 Item 3 Effective/not effective at preventing HIV .63 .80 Item 4 Convenient/inconvenient to use .18 .83 Item 5 Easy/hard to obtain .18 .83 Item 6 Not embarrassing/embarrassing .18 .83 Item 7 Easy/difficult to discuss with a partner .25 .83 Item 8 Easy/difficult to use .63 .80 Item 9 Comfortable/uncomfortable .66 .80 Item 10 They increase/decrease sexual pleasure .56 .80 Item 11 Something my friends like/hate .51 .81 Item 12 Something my sexual partners like/hate .45 .81 Item 13 Exciting/dull .59 .80 Item 14 Neat/messy .40 .82Note. MFACS = Multi-Factor Attitude toward Condoms Scale; STI = sexually transmitted infection.
Cronbach α values for the total and subscale scores were similar between the first and second administrations, and positive correlations were found between test and retest scores for the total MFACS total and subscales (p < .05; Table 5).
Table 5. - Two-Week Retest Reliability Analyses MFACS Item Number Test (n = 336) r p-Value Retest (n = 56) Min Max Cronbach α Mean ± SD Mean ± SD Min Max Cronbach α Perceived effectiveness 3 3 21 .92 16.18 ± 4.95 .35 .008 17.89 ± 3.23 9 21 .80 Affective 5 5 35 .85 19.38 ± 7.55 .56 .001 17.16 ± 7.83 5 35 .86 Manageability 6 6 42 .90 30.18 ± 9.50 .33 .01 32.00 ± 9.17 6 42 .91 MFACS total 14 23 98 .82 65.74 ± 14.66 .40 .002 67.05 ± 13.63 32 98 .82Note. Max = maximum value; MFACS; Multi-Factor Attitude toward Condoms Scale; Min = minimum value; r = Spearman correlation.
The criterion-related validity of the Turkish MFACS was supported by significant correlations of total and subscale scores with received training on STI, knowledge of condom usage, and using condom in the last sexual relationship (p < .05). No significant difference was found between female and male participants' total and subscale scores (>0.05; Table 6).
Table 6. - Comparison of the MFACS Total and Subscale Scores Based on Sexual Knowledge and Experience (N = 336) MFACS Have You Received Previous Training on STI? z p-Value Yes (n = 213) No (n = 113) Mean ± SD Mean ± SD Perceived effectiveness 16.35 ± 5.38 15.89 ± 4.09 2.337 .019 Affective 25.24 ± 7.69 23.29 ± 7.05 2.321 .020 Manageability 25.29 ± 8.47 24.64 ± 6.70 1.848 .050 MFACS total 66.88 ± 15.88 63.82 ± 12.13 2.776 .006 Do You Know How to Use Condoms Correctly? z p-Value Yes (n = 277) No (n = 59) Perceived effectiveness 16.48 ± 5.20 14.79 ± 3.21 4.195 .001 Affective 24.98 ± 7.81 22.39 ± 5.46 3.058 .002 Manageability 25.69 ± 8.22 22.03 ± 4.80 4.834 .001 MFACS total 67.15 ± 14.96 59.22 ± 11.22 4.896 .001 Did You Use a Condom in Your Last Sexual Relationship? z p-Value Yes (n = 170) No (n = 166) Perceived effectiveness 16.96 ± 5.20 15.39 ± 4.55 4.373 .001 Affective 25.55 ± 7.15 23.48 ± 7.74 2.769 .006 Manageability 26.49 ± 8.61 23.58 ± 6.70 4.931 .001 MFACS total 68.99 ± 16.36 62.45 ± 11.89 5.736 .001 Female (n = 168) Male (n = 168) z p-Value Perceived effectiveness 16.42 ± 4.15 15.95 ± 5.63 0.533 .978 Affective 24.07 ± 6.24 24.99 ± 8.60 1.278 .594 Manageability 25.52 ± 6.69 24.58 ± 8.86 0.050 .201 MFACS total 66.00 ± 12.78 65.52 ± 16.39 0.027 .960Note. MFACS = Multi-Factor Attitude toward Condoms Scale; STI = sexually transmitted infection; z = Mann–Whitney U test.
Our findings support the reliability of the Turkish MFACS. We found a high level of internal consistency, as evidenced by a Cronbach α value of 0.82 and moderate to high item-total correlations for most items, which is consistent with previous reports (Hollub et al., 2011; Reece et al., 2010). Only moderate retest reliability estimates were found. Given that attitudes toward condom use have shown within-person variability over a 30-day period (Kiene et al., 2008), it is possible that the moderate correlations reflect construct, rather than measurement, instability. Neither the original MFACS development study (Reece et al., 2010) nor the Chinese translation study (Choi et al., 2020) measured retest scores, precluding comparisons with our findings.
We also found evidence of construct validity with the finding of three-factor solution, which aligned with the three instrument subscales and explained 71% of the variance. Similar to our findings, Reece et al. (2010) reported a three-factor solution that explained 61.44% of the total variance. We found that Item 9 in the affective subscale of the original MCFAS loaded on the factor that corresponded to the manageability subscale. Additionally, Item 14 in the manageability subscale of the original MCFAS loaded on the factor that corresponded to the affective subscale. It is not unexpected that items on a translated instrument will move to different factors due to nuances in meanings that reflect different sociocultural values and religious beliefs (Choi et al., 2020; McMillan & Worth, 2011; Smerecnik et al., 2010; Smith, 2017; Zhang et al., 2004).
ConclusionThe Turkish version of the MFACS is a valid and reliable measure of attitudes toward condoms. Its psychometric properties support its use in interventional studies to favorably modulate condom attitudes to increase their use.
DisclosuresThe authors report no real or perceived vested interests related to this article that could be construed as a conflict of interest.
Author ContributionsS. Ozdemir was responsible for conceptualizing the study, including development of the methodology, and provided leadership, carried out the statistical analyses, and wrote the original draft, as well as reviewing and revising the manuscript. E. Oz was responsible for data visualization and contributed to the original draft as well as the revised version of the manuscript. K. E. Karasahin was responsible for language editing and contributed to the original draft and the revised version of the manuscript. B. K. Bicer was responsible for applying the statistical analyses and reviewed, and revised the manuscript.Key Considerations Determining individuals' attitudes toward condoms is an important step in increasing the use of condoms, thereby protecting sexual health and preventing sexually transmitted diseases. The Turkish version of the Multi-Factor Attitude toward Condoms Scale (MFACS) is a valid and reliable instrument that can be used in behavioral change studies. The Turkish version of MFACS will advance the design of tailored behavioral change interventions to increase condom use.
AcknowledgmentsThe authors express their gratitude to all volunteers who took part in this study.
References Ayre C., Scally A. J. (2014). Critical values for Lawshe's content validity ratio: Revisiting the original methods of calculation. Measurement and Evaluation in Counseling and Development, 47(1), 79-86. https://doi.org/10.1177/0748175613513808 Beaton D. E., Bombardier C., Guillemin F., Ferraz M. B. (2000). Guidelines for the process of cross-cultural adaptation of self-report measures. Spine, 25(24), 3186-3191. https://doi.org/10.1097/00007632-200012150-00014 Choi E. P. H., Fong D. Y. T., Wong J. Y. H. (2020). The use of the Multidimensional Condom Attitude Scale in Chinese young adults. Health Quality of Life Outcomes, 18(331), 1-12. https://doi.org/10.1186/s12955-020-01577-9 Francis S. C., Mthiyane T. N., Baisley K., Mchunu S. L., Ferguson J. B., Smit T., Crucitti T., Gareta D., Dlamini S., Mutevedzi T., Seeley J., P
留言 (0)