
記住我

HIV is a global health and social issue that asymmetrically affects the population and has varying impacts at different life stages for individuals, families, and communities. In 2019, 778 new cases of HIV were diagnosed in Portugal, with the proportion 2.3 times higher in men than in women (Directorate-General of Health [DGS], 2020). The mean age of recently diagnosed persons living with HIV (PLWH) was 38.0 years, and 24.1% of individuals were 50 years or older. The highest diagnosis rates occurred among the 25- to 29-year age group. Considering the 749 new cases diagnosed in 2019, a stratified analysis revealed that in 729 (97.3%), transmissions occurred through risky sexual behaviors and 16 transmissions were associated with injection drug use (IDU). Between 2000 and 2019, 65% of new infections in Portugal were related to sexual behaviors (DGS, 2020).
Adverse Experiences and Risk BehaviorsExposure to potentially traumatic events (PTEs)—sexual abuse, childhood neglect, and domestic violence—is prevalent in societies worldwide, is associated with extensive costs to individuals and societies, and is a significant global public health concern (e.g., Magruder et al., 2017). The effects of trauma extend far beyond its immediate psychological and physical effects; trauma can change an individual's biology and behavior throughout life, with a significant impact on interpersonal and intergenerational relationships (Kimberg & Wheeler, 2019). PTEs can include exposure to war, interpersonal violence, disasters, sudden loss, serious illness, and other overwhelming and disturbing events (Kleber, 2019).
Over the past few decades, adverse experiences in childhood (e.g., sexual abuse and neglect) and/or adulthood (e.g., domestic violence) have received attention from the scientific community as predictors of health risk behaviors (e.g., VanderEnde et al., 2018). Felitti et al. (1998) described the relationship between exposure to adverse individual experiences (e.g., psychological, physical, and sexual abuse) and family adverse experiences (e.g., exposure to violence against one's mother, mental health problems and suicide in one's family, or the imprisonment of family members), risk health behaviors, and adult illness. The study by Felitti et al. (1998) documented that adverse experiences tend to co-occur and that there is a positive association between the frequency of exposure to trauma and the risk of disease and the adoption of health-damaging behaviors in adulthood. Felitti et al. (1998) also found that the co-occurrence of four or more types of adverse experiences in childhood increased the possibility of adopting risk behaviors, namely, alcohol and drug use and suicide attempts, by 4–12 times; the risk of smoking by 2–4 times; and having multiple sexual partners and contracting sexually transmitted infections twofold. Other studies (Larkin et al., 2012; Ports et al., 2016; Thompson et al., 2015; Wade et al., 2016) state that young adults with at least one adverse childhood experience (ACE) report an increased lifetime experience of psychological problems/disorders, drug use, and/or court involvement.
Adverse childhood experiences are also associated with a twofold to fourfold increase in drug use in adolescence and an increased risk of alcohol or drug use in adulthood (Dube et al., 2003). Consistently, other studies revealed that ACEs are a significant predictor of alcohol and drug use in adolescence (Meeker et al., 2021; Musa et al., 2018) and in adulthood (Hughes et al., 2017), especially of IDU (Hughes et al., 2017). A meta-analysis estimating the prevalence of childhood trauma among people with substance use disorder found the occurrence of each subtype of childhood trauma across all substance use disorder samples to vary from 31% for sexual abuse or emotional neglect to 38% for emotional abuse. The authors conclude that ACEs are prevalent among substance use disorder samples (Zhang et al., 2020). According to Stein et al. (2017), ACEs are associated with youth drug use (e.g., opioid) and with a greater probability of experiencing an overdose in one's lifetime. Approximately half of the participants of this study (persons seeking inpatient opioid treatment) had experienced at least four of the 10 assessed ACEs. In addition, a study conducted in Vietnam on men living with HIV found that having witnessed interparental violence as a child was associated with risky behaviors in adulthood, including problematic alcohol use, multiple sexual partners, and was significantly related to perpetrating intimate partner violence in adulthood (Hershow et al., 2020).
For sexual risk behaviors, child sexual abuse is the most studied predictor and is a significant indicator, in adulthood, of having more sexual partners (Muldoon et al., 2018), engaging in sexual relations in exchange for money or sex work (Henny et al., 2007), inconsistent use of condoms during sexual activity, having unprotected sex (e.g., VanderEnde et al., 2018), and experiencing early sexual contact (Muldoon et al., 2018; Musa et al., 2018). Accordingly, a meta-analysis that studied the relationship between childhood maltreatment and risky sexual behaviors (Wang et al., 2019) concluded that childhood sexual abuse was significantly associated with the risk of having an early sexual debut, of having multiple sexual partners, of having transactional sex and having unprotected sex.
Regarding adverse experiences in adulthood, women who experience multiple forms of victimization are more likely to engage in risky sexual behaviors, such as having an increased number of sexual partners and engaging in substance use before sexual intercourse (Walsh et al., 2012). In addition, women who have experienced violent forms of trauma (e.g., physical aggression from one's partner) or nonviolent trauma (e.g., loss of a child to foster care) are more likely to engage in crack use; those who witnessed a physical assault were more likely than to have exchanged sex (Brown-Peterside et al., 2002). A study of 104 women living with HIV concluded that more than 90% reported having experienced lifetime trauma, including an average of 4.2 adverse experiences. The number of traumatic experiences was found to be positively associated with mental health outcomes (e.g., depression, anxiety, and posttraumatic stress disorders) and with potentially harmful alcohol and drug use (Cuca et al., 2019). Another study with 3,084 currently married women in Nepal concluded that the experience of intimate partner violence was associated with HIV-risk behaviors, namely, multiple sex partners, inconsistent condom use, partner with known HIV risks, and inability to negotiate safer sexual practices (Shrestha & Copenhaver, 2016). Family-related variables, such as attachment, safety, family communication, and exposure to family violence, are also associated with risky sexual behavior (Secor-Turner et al., 2013). From a systematic review, Kirby and Lepore (2007) found that living in chaotic and unpredictable family environments—family violence, drug use, or physical abuse in childhood—are associated with risky sexual behavior in adolescence. In addition, a recent systematic review stated that adolescent alcohol use was associated with sibling and peer alcohol use, parental alcohol use or abuse, parental separation, and a single mother family (Bozzini et al., 2021). Another systematic review of 19 studies on the relationship between marital violence and HIV revealed that the co-occurrence of physical and sexual victimization is significantly associated with a diagnosis of HIV (Li et al., 2014).
There is a vast amount of empirical knowledge on the prevalence of trauma in PLWH and on its impact on behavior and health, with rates of trauma in PLWH ranging from 10% to 90%, the association of which increases the likelihood of HIV risk behavior (e.g., Brezing et al., 2015). In addition, Singer and Clair (2003) described the phenomenon of SAVA (syndemic of substance abuse, violence, and AIDS) from the early 2000s. According to the authors, there is a synergistic interaction between disease and social conditions at the biological and population levels. According to this body of evidence, researchers and health and social institutions have reflected on the need for trauma-informed care approaches to adopt multilevel interventions to improve the health and resilience of PLWH (e.g., Brezing et al., 2015; Sales et al., 2016; Substance Abuse and Mental Health Services Administration [SAMHSA], 2018). To address the needs of PLWH, the National Alliance of State and Territorial AIDS Directors, 2018 presented a trauma-informed approach toolkit for HIV that considered the relationship between intersectional factors influencing a person's health outcomes at various levels, including the structural, community, interpersonal, and individual levels, and the potential of how these traumas may lead to an HIV diagnosis and related negative health outcomes. According to this approach, past and ongoing traumatic experiences have an impact along the HIV continuum and contribute to whether a person who contracts HIV is diagnosed, is given access to and retains care, and maintains viral suppression.
The literature shows that early and cumulative adverse experiences throughout life assume a preponderant role in the adoption of health risk behaviors, particularly about the transmission of infectious diseases. Studies usually focus on adverse experiences occurring in only one stage of life (e.g., childhood), however, while disregarding the potential cumulative effects of these experiences throughout life. Samples of women or men to analyze different risk behaviors are largely used (e.g., more studies of women are related to risky sexual behaviors) while not assuming a comparative position between the two sexes. However, the comparison of adverse experiences in PLWH based on HIV risk behavior (sexual, IDU) and experiences of childhood and adulthood adversity, including different risk behaviors, has not been widely considered. Therefore, the central objective of this study is to characterize the history of exposure to adverse experiences throughout life (childhood and adulthood) in PLWH in northern Portugal. Specifically, the study aims to understand patterns of trauma exposure in men and women living with HIV in northern Portugal and to identify which of these adverse experiences are associated with risk behaviors for HIV infection (i.e., sexual exposure and IDU).
Methodology Design, Participants, and Data CollectionThis is a cross-sectional retrospective study of a sample of 328 PLWH, ages 18 or older, who received care through integrated specialized services for HIV in seven hospitals in northern Portugal. A statistical power analysis was performed a priori for sample size estimation based on statistical data on HIV numbers in Portugal available at the time of the study (DSG, 2015). These data report a ratio of 2.6 male PLWH to each female PLWH and report the sexual transmission mode and IDU to apply to 65% and 35% of PLWH, respectively. With an alpha of 0.05 and power of 0.95, the projected sample size needed for a large effect size (GPower 3.1 software) was approximately N = 144 for the logistic regression analysis to test the adverse lifelong experiences associated with HIV transmission mode (sexual vs. IDU).
The study was submitted and approved by the National Data Protection Commission (770/2010) and ethics committee of Hospital of Braga (126/2014). After ethical approval, the principal researcher contacted the doctors responsible for the infectious disease or internal medicine services of each of the seven hospitals. With the doctors' consent, the researcher, a psychologist with training in interviewing persons with a history of trauma, remained in the hospital on days with scheduled medical appointments for PLWH. During a medical appointment, a doctor informed his or her patients of the ongoing study and referred them to the researcher if they were interested in participating.
The researcher involved in data collection, a psychologist with clinical training who could therefore—in cases of emotional activation—take special care in the stabilization of the subject and refer to specialized intervention—if the participant agreed—presented the study's objectives. After obtaining written informed consent, data were collected, which lasted an average of 30 min. Data collection occurred between November 2014 and February 2015. There was no compensation for participating in the study, and all procedures were performed in accordance with the ethical standards of institutional and national research committees and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Measures Sociodemographic and health questionnaireThis questionnaire is divided into three main parts focused on (a) personal and family variables; (b) socioprofessional variables; and (c) health conditions, comorbidities, and transmission modes (Maia et al., 2014).
History of adversity in childhood questionnaireWe used the Portuguese version of the “Family ACE Questionnaire,” which retrospectively assesses the occurrence of different types of adverse experiences in childhood (Silva & Maia, 2008). We used the short version of the questionnaire validated for Portuguese population, with 17 questions, which allowed us to identify 10 types of adverse experiences. Scores range from 0 if the participant does not report any category of adversity to 10 if the participant reports all types of adversity. In previous studies, validity testing revealed high kappa coefficients for physical, emotional, and domestic violence (ranging from 0.56–0.72) and scores between 0.46 and 0.86 for the other categories (Dube et al., 2004). For this sample, the Cronbach alpha value was measured as 0.87 for the total instrument.
List of life eventsThis measure presents 16 items corresponding to the same number of PTEs in adulthood (e.g., fires, accidents, physical or sexual violence, and death; Portuguese version from Maia & Fernandes, 2002). For each event, the participant is asked to select one of the following: It happened to me; I saw it happening; I knew it happened; or Does not apply. Scores range from 0 (if the participant does not report any type of adversity) to 16 (if the participant reports experiencing all types of adversity). For our sample, the Cronbach alpha value is 0.85.
Statistical Analysis PlanThe data were analyzed with Statistical Package for Social Sciences version 27.0. Descriptive statistics, chi-square tests, and t tests were performed to analyze the differences between men and women and the sexual transmission mode versus IDU mode with respect to ACEs and adverse adulthood experiences. We used the Fisher exact test when cells had expected frequencies of <5 and measured effect sizes.
Logistic regression was performed to identify the ACE and adulthood adverse experiences associated with the HIV sexual transmission mode versus the IDU mode. In the first model, the individual variables related to sex and age were tested. In a second model, we added ACEs (psychological abuse, physical abuse, emotional neglect, physical neglect, family substance use, and parents' imprisonment) and the total number of ACEs experienced. In the third model, individual adverse experiences during adulthood that significantly differed between the two groups (life-threatening injury/illness; sudden, unexpected death of a loved one; threats with weapon; physical assault, causing injuries/hurting someone; witnessed sudden, unexpected death of a loved one; and witnessed violent death) and the total number were tested.
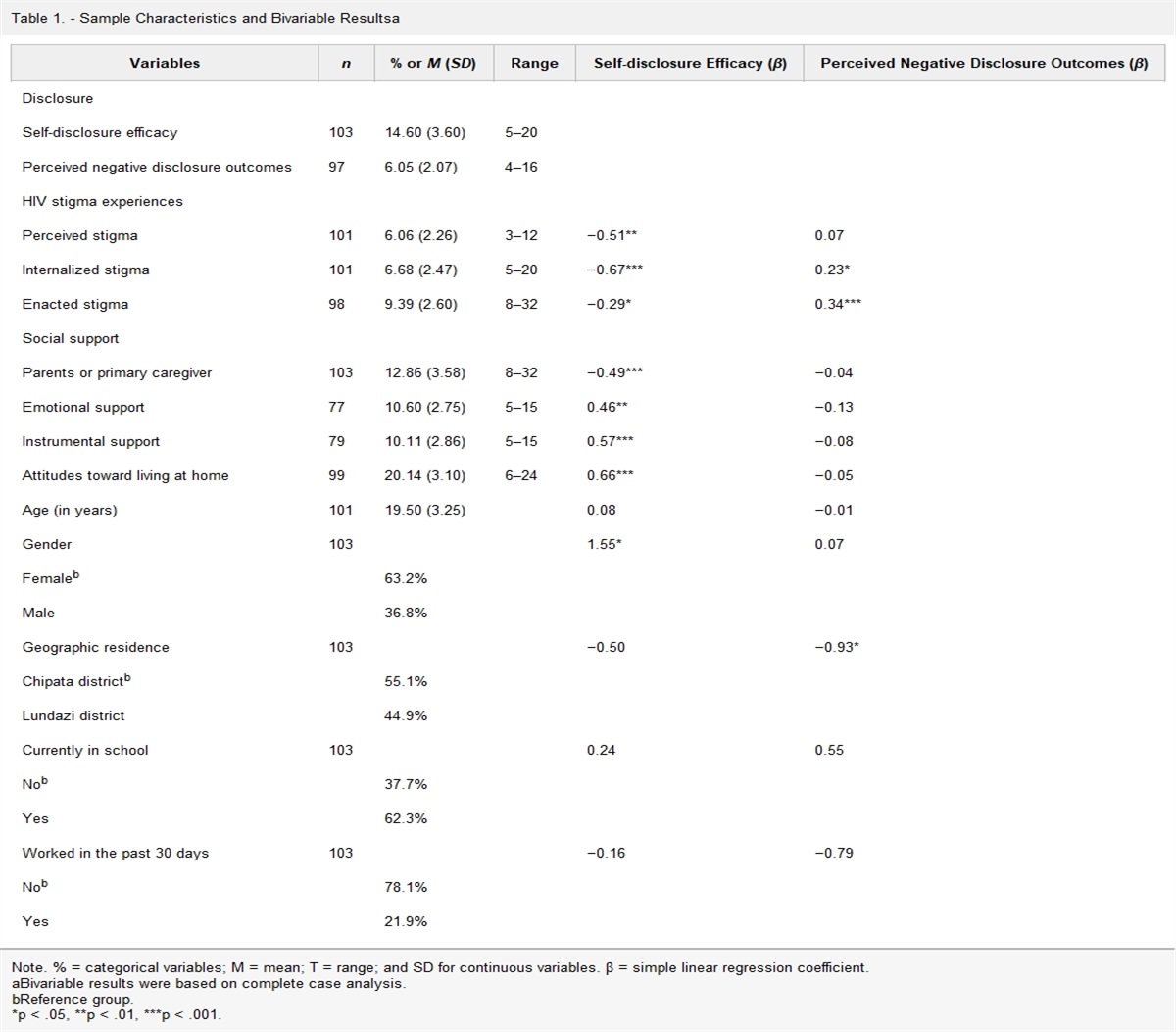
ResultsThe participants included 328 PLWH. Most of the participants were men (n = 261; 79.6%); the mean age of the participants was 45.64 (SD = 11.26; Min = 21; Max = 85), whereas participants had been living with a known HIV diagnosis for a mean of 10.34 years (SD = 6.41; Table 1). This number is representative of people living in northern Portugal with HIV during the studied period.
Table 1. - Sociodemographic Description of Participants Total Sample Men Women χ2 (ϕ or Cramér's V) Sexual Injection Drug Use χ2 (ϕ or Cramér's V) n = 328 n = 261 n = 67 n = 233 n = 95 n (%) n (%) n (%) n (%) n (%) Sex Men 261 (79.6) — — 182 (71) 79 (83.2) 1.0 (0.06) Women 67 (20.4) — — 51 (21.9) 16 (16.8) Nationality Portuguese 314 (96.6) 252 (96.6) 62 (92.5) 2.10 (0.08) 220 (95.2) 94 (100) Foreign 14 (3.4) 9 (3.4) 5 (7.5) 14 (4.8) — Marital status Single 132 (40.4) 107 (41.20) 25 (37.30) 8.69* (0.16) 92 (39.7) 40 (42.1) 12.24* (0.19) Married/civil union 141 (43.1) 112 (43.1) 29 (43.3) 106 (45.7) 34 (36.8) Divorced/separated 43 (13.1) 32 (12.3) 11 (16.4) 25 (10.8) 2 (2.1) Widow 11 (3.4) 9 (3.5) 2 (3.0) 9 (3.9) 18 (18.9) Academic completed qualifications Primary school 239 (73.1) 195 (75.0) 44 (65.7) 6.80** (0.14) 161 (69.4) 78 (82.1) 8.50* (0.16) High school 54 (16.5) 36 (13.8) 18 (26.9) 40 (17.2) 14 (14.7) Higher education 34 (10.4) 29 (11.2) 5 (7.5) 31 (13.4) 3 (3.2) Employment status Employed 107 (32.6) 91 (34.9) 16 (23.9) 17.27** (0.23) 88 (37.7) 19 (20.0) 15.10** (0.21) Unemployed 102 (32) 71 (27.2) 21 (31.3) 73 (31.3) 32 (33.7) Retired/pensioner 116 (35.4) 99 (37.9) 30 (44.80) 72 (30.9) 44 (46.3) Total Sample Men Women χ2 (ϕ or Cramér's V) Sexual Injection Drug Use t (d) n = 328 n = 261 n = 67 n = 233 n = 95 M (SD) M (SD) M (SD) M (SD) M (SD) Age 45.64 (11.26) 47.29 (11.29) 39.11 (11.49) 5.51*** (0.76) 46.0 (12.64) 44.77 (6.81) 0.81 (0.11) Time since diagnosis 10.34 (6.41) 10.48 (6.62) 9.82 (5.57) =-.75 (0.10) 9.05 (6.08) 13.5 (6.16) 5.88***(0.72) Risk behaviors Life alcohol use No 151 (47.3) 110 (43.1) 41 (64.1) 8.99** (0.17) 129 (57.1) 22 (23.7) 29.53*** (0.30) Yes 168 (52.7) 145 (56.9) 23 (35.9) 97 (42.9) 71 (76.3) Life tobacco use No 101 (31.6) 76 (29.7) 25 (39.1) 2.08 (0.08) 98 (43.2) 3 (3.2) 48.74*** (0.39) Yes 219 (68.4) 180 (70.3) 39 (60.9) 129 (56.8) 90 (96.8)*p < .05; **p < .01; ***p < .001.
Compared with the male participants, the female participants were significantly younger, and a higher proportion had a high school education and were unemployed or retired. As the main causes of HIV, the participants cited unprotected sex (n = 233; 71.0%) or sharing materials associated with IDU (n = 95; 29.0%). Considering the two categories of transmission self-identified by the participants (sexual and IDU), comparative analyses were performed on the two groups (Table 1). A higher proportion of IDU participants were single or widowed, had fewer academic qualifications, were unemployed or retired, and engaged in alcohol or tobacco use. IDU participants knew of their HIV diagnosis for the longest amount of time.
Adverse Childhood ExperiencesParticipants reported, on average, 1.93 (SD = 2.49) childhood adverse experiences. There were significant differences between men and women related to the number of ACEs reported (t(326) = 3.45, p = .001, d = 0.61). Women reported a higher number of ACEs (M = 4.39, SD = 4.98) than men (M = 2.17, SD = 3.22). Regarding HIV transmission mode, there were no significant differences related to the number ACEs reported (t(326) = −1.86, p = .063, d = .23), although IDU participants reported more experiences (M = 2.33, SD = 2.65) than participants who reported sexual HIV transmission (M = 1.77, SD = 2.41).
A detailed description of ACE by sex and HIV transmission mode is presented in Table 2. A significantly higher proportion of women reported physical abuse, sexual abuse, physical and emotional neglect, exposure to domestic violence, and family alcohol use than men. Overall, a higher proportion of IDU participants reported the different types of adverse experiences than those with sexual risk behavior, with the exception of exposure to domestic violence, sexual abuse, and parental divorce.
Table 2. - Childhood Adverse Experiences by Sex and HIV Transmission Mode Adverse Childhood Experiences Total (n = 328) Sex χ2 (Φ) HIV Transmission Mode χ2 (Φ) Men (n = 261) Women (n = 67) Sexual (n = 233) Injection Drug Use (n = 95) n (%) n (%) n (%) n (%) n (%) Psychological abuse 88 (26.8) 64 (24.5) 24 (35.8) 3.47* (0.10) 53 (22.7) 35 (36.8) 6.83* (0.15) Physical abuse 66 (20.1) 46 (17.6) 20 (29.9) 4.96** (0.12) 42 (18.0) 24 (25.3) 3.75* (0.10) Sexual abuse 12 (3.7) 6 (2.3) 6 (9.0) 6.70** (0.14) 9 (3.9) 3 (3.2) 0.09 (0.02) Physical neglect 68 (20.7) 47 (18.0) 21 (31.3) 5.77** (0.13) 40 (17.2) 28 (29.5) 6.22* (0.14) Emotional neglect 48 (16.6) 12 (12.3) 16 (23.9) 5.76** (0.13) 28 (12.0) 20 (21.1) 4.41* (0.12) Exposure to domestic violence 81(24.7) 55 (21.1) 26 (38.8) 9.02*** (0.17) 54 (23.2) 27 (28.4) 0.99 (0.06) Parents' mental health problems 34 (10.5) 24 (9.3) 10 (15.2) 1.88 (0.08) 20 (8.7) 14 (15.1) 2.94 (0.09) Family alcohol use 73 (22.6) 48 (18.70) 25 (37.9) 11.70****(0.19) 45 (19.6) 28 (30.1) 4.21* (0.11) Parents' imprisonment 8 (2.5) 4 (1.6) 4 (6.1) 4.41* (.12) 3 (1.3) 5 (5.4) 4.55* (0.12) Parents' divorce 34 (10.4) 14 (5.4) 20 (29.9) 34.41 (0.32) 22 (9.4) 12 (12.9) 0.74 (0.05) Number of adverse childhood experiences 0 179 (54.6) 144 (56.7) 27 (40.9) 132 (56.7) 47 (49.5) 1 23 (7.0) 20 (7.9) 3 (4.5) 18 (7.7) 5 (5.3) 2 18 (5.5) 14 (2.4) 6 (6.1) 13 (5.6) 5 (5.3) 3 6 (1.8) 6 (2.4) - 5 (2.1) 1 (1.1) 4 20 (6.1) 13 (5.1) 7 (10.6) 13 (5.6) 7 (7.4) 5 14 (4.3) 11 (4.3) 3 (4.5) 10 (4.3) 4 (4.2) 6+ 68 (20.7) 46 (18.1) 22 (33.2) 42 (18.0) 26 (27.4)Regarding the number of life adverse experiences in adulthood, participants reported, on average, 3.74 (SD = 1.97). There were no significant differences between men and women in the number of adverse adulthood experiences (t(326) = 1.33, p = .19, d = 0.21); men reported an average of 4.07 (SD = 2.47) experiences, whereas women reported an average of 4.61 (SD = 3.13) experiences. In contrast, significant differences were found as a function of the mode of infection (t(326) = −5.94, p <.001, d = 0.72) with those infected by IDU reporting more events (M = 4.71, SD = 1.61) than those who were sexually infected (M = 3.35, SD = 1.97).
Table 3 presents adverse adulthood experiences by sex and self-reported HIV transmission mode. More women reported experiencing a fire or explosion, persecution, the sudden or unexpected death of a loved one, sexual assault, and witnessing the sudden or unexpected death of a loved one. Almost one-third of the women and one-third of the men reported having six or more adulthood adverse experiences.
Table 3. - Adverse Adulthood Experiences by Sex and HIV Transmission Mode Adverse Adulthood Experiences Total (n = 328) Sex χ2 (Φ) Transmission Mode χ2 (Φ) Men (n = 261) Women (n = 67) Sexual (n = 233) Injection Drug Use (n = 95) n (%) n (%) n (%) n (%) n (%) Fire or explosion 80 (24.4) 55 (21.1) 25 (37.3) 7.23** (0.15) 55 (23.6) 25 (26.3) 0.27 (0.03) Motor vehicle accident 220 (67.1) 181 (69.3) 39 (58.2) 2.30 (0.09) 149 (63.9) 71 (74.7) 3.56 (0.10) Other serious accident 87 (26.5) 72 (27.6) 15 (22.4) 0.74 (0.05) 57 (24.5) 30 (31.6) 1.75 (0.07) Persecution 58 (17.7) 41 (15.7) 17 (25.4) 3.42* (0.10) 36 (15.5) 22 (23.2) 2.75 (0.09) Run over 71 (21.6) 55 (21.1) 16 (23.9) 0.25 (0.03) 47 (20.2) 24 (25.3) 1.03 (0.06) Robbery 127 (38.7) 106 (40.6) 21 (31.3) 1.93 (0.08) 85 (36.5) 42 (44.2) 1.70 (0.07) Life-threatening injury/illness (other than HIV) 119 (36.3) 95 (36.4) 24 (35.8) 0.08 (0.01) 72 (30.9) 47 (49.5) 10.07** (0.18) Sudden, unexpected death of a loved one 193 (58.8) 147 (56.3) 46 (68.7) 3.35* (0.10) 126 (54.1) 67 (70.5) 7.54* (0.15) Assault with a weapon 102 (31.1) 83 (31.8) 19 (28.4) 0.30 (0.03) 61 (26.2) 41 (43.2) 9.08* (0.17) Physical assault 129 (39.3) 97 (37.2) 32 (47.8) 2.51 (0.09) 71 (30-5) 58 (61.1) 26.44*** (0.28) Sexual assault 25 (7.6) 11 (4.2) 14 (20.9) 21.97*** (0.25) 17 (7.3) 8 (8.4) .12 (0.02) Caused the serious injury/death of another person 53 (16.2) 41 (15.7) 12 (17.9) 0.20 (0.03) 27 (11.6) 26
留言 (0)