
記住我

Coronavirus disease 2019 (COVID-19) is associated with adverse outcomes among vulnerable populations, including older adults (i.e., 65+ years old), those with underlying cardiovascular, metabolic, or respiratory conditions, or persons with suppressed immune systems (e.g., people living with HIV [PLWH]; Khalili et al., 2020). Some studies have reported that compared with the general population, PLWH are more likely to experience adverse health outcomes on contracting SARS-CoV-2 (e.g., decreased sleep quality, increased depression and anxiety, and elevated substance use; Dyer et al., 2021; Hochstatter et al., 2021; Marbaniang et al., 2020). Moreover, in comparison with PLWH not receiving antiretroviral therapy (ART), those who are on ART have been reported to have a favorable prognosis for COVID-19 (Del Amo et al., 2020; Mirzaei et al., 2021).
Although guidelines have been developed for the care and prevention of COVID-19 among PLWH (Centers for Disease Control and Prevention, 2020; National Institutes of Health, 2020; UNAIDS, 2020b), the pandemic has affected HIV care continuity and, subsequently, the health status of PLWH because of stay-at-home orders and restricted access to public transportation (Hogg, 2018; Jiang et al., 2020; Shiau et al., 2020). In addition, the COVID-19 pandemic has resulted in the isolation of PLWH and adversely affected their employment status, which could lead to increased experiences of psychoemotional stress and adverse mental health outcomes (Jiang et al., 2020; Shiau et al., 2020).
Additional concerns exist around redirecting HIV resources and international/national funds to COVID-19, therefore reducing the capacity and reach of HIV services (Adepoju, 2020; Jiang et al., 2020). Although the UNAIDS 90-90-90 targets (Bain et al., 2017) were not met in 2020, the diversion of HIV health care resources to COVID-19 may reduce any recent progress and achievements made in meeting these goals (UNAIDS, 2020d). Our understanding of the impact of COVID-19 on HIV care and services continues to grow. Initial UNAIDS reports suggest that the impact of the pandemic has been most detrimental and concerning for PLWH living in low- and middle-income countries (LMICs) because of pre-existing inadequacies of the HIV care infrastructures (UN News, 2020; UNAIDS, 2020a,2020c).
In the Eastern Mediterranean region, Iran has the largest epidemic of COVID-19 (2,855,396 COVID-19 cases and 79,056 deaths, as of May 25, 2021) and HIV (59,000 adults and children living with HIV in 2019; Karamouzian et al., 2017; World Health Organization, 2021). The HIV epidemic in Iran is concentrated among key at-risk populations, such as people who inject drugs and female sex workers; however, injection drug use remains the primary mode of HIV transmission among new incident cases of HIV (SeyedAlinaghi et al., 2021).
Our understanding of the impact of COVID-19 on PLWHs' health and their lived experiences during the ongoing pandemic remains limited in Iran. We therefore conducted this qualitative study to interview PLWH in Kerman and improve our understanding of how COVID-19 has affected their lives.
Methods SettingThis qualitative study was conducted in Kerman Province. Kerman is the largest Iranian province, with a population of more than 3.1 million people (Statistical Center of Iran, 2016). As of 2016, 1,100 PLWH were estimated to live in Kerman Province (Hooshyar et al., 2018). Although provincial-level statistics on COVID-19 are unavailable, limited data suggest that the incidence in Kerman was lower than in other provinces. As of June 2020, the seroprevalence of antibodies against SARS-CoV-2 was 17.1% nationwide and 8.2% in Kerman (Poustchi et al., 2020).
Participants were recruited from the voluntary counseling and testing center (VCT) of Kerman city between August and October 2020. This center is the only governmental HIV treatment center that provides free HIV treatment in the city of Kerman and offers services such as confidential HIV tests, pre-test and post-test counseling, and health promotion interventions to prevent HIV acquisition and transmission. For PLWH, the center facilitates their access to HIV care and ART, helps them to disclose their HIV status to family members, provides emotional and psychological support, and educates them on coping strategies to deal with HIV-related stigma and discrimination.
SampleParticipants were recruited through convenience sampling. We recruited PLWH who were receiving services at the VCT and provided verbal informed consent for participation in the study.
ProceduresThis qualitative study was designed and conducted by an experienced team of HIV researchers with close working relationships with the community of PLWH in Kerman, Iran. The interviews were conducted by a graduate student (i.e., the first author) who had previous training on and experience with conducting in-depth interviews for research studies.
The first author approached VCT patients who were previously known to her and briefly described the aims and scope of the study. Consenting individuals were invited to participate in the interview after receiving their service for the day or to book an appointment for a later visit at the VCT. Semistructured, face-to-face interviews were conducted in Persian in a private well-ventilated room in the VCT while following the recommended COVID-19 prevention guidelines (e.g., mask wearing and physical distancing between the interviewer and the interviewees).
The interviews began with a detailed description of the study's objectives and an overview of interview procedure. During the interview, participants were asked to talk about their personal lived experiences of accessing HIV care and services since the beginning of the COVID-19 pandemic. The interview guide questions were informed by an in-depth literature review. Three HIV experts involved in the care and provision of clinical and psychosocial services to PLWH and affiliated with the office of infectious diseases control in Kerman University of Medical Sciences evaluated and modified the questions. The interview questions included but were not limited to “Have you had access to health care services during the COVID-19 pandemic?,” “What effects has the COVID-19 pandemic had on your social interactions?,” and “How has the COVID-19 pandemic affected your household income?” The interviewer probed and asked additional clarifying questions as the interview proceeded. Each interview lasted approximately 30 min. Interviews were audio-recorded, and field notes were taken. All recorded interviews were kept in a password-protected file and transferred to a local password-protected server accessible only to the research team. Participants were given an honorarium of 500,000 IRRs (equivalent to $3 USD) to compensate them for their time and transportation costs.
Data AnalysisData were analyzed using an inductive content analysis approach (Bengtsson, 2016) to allow for themes to emerge from the data. Interviews were transcribed verbatim, anonymized, and securely filed by the interviewer on the day of the interview. The transcripts were initially read and re-read by the first and senior authors, and discrepancies in interpretation of transcripts were settled through discussion with coauthors. Participants' accounts were organized into patterns, and then to major open codes and concepts reflecting their experiences, and discussed at weekly online team meetings. During the thematic analysis, a map of initial themes and corresponding subthemes was created (Thomas, 2006). Throughout the data collection period, interpretations were developed about recurring and contradictory codes within the data, and revisions were made as new data were collected. This approach allowed us to identify distinct themes. The analysis focused on the most frequent themes identified in the data, as well as divergent cases. The coauthors met weekly to check codes and themes for consistency and accuracy and to address potential ambiguities. Sampling was continued until thematic saturation was reached, and no new themes were found during the interview coding and thematic analysis. In addition, data collection was continued for three more interviews to ensure and confirm that no new themes emerged and no additional relevant information was provided in the interviews (Saunders et al., 2018). MAXQDA 10 software (MAXQDA Software, n.d.) was used to manage and analyze the data.
TrustworthinessTo maintain trustworthiness, we followed the four criteria of credibility, transferability, dependability, and conformability (Lincoln & Guba, 1985). Data credibility was established by team discussions, member checking, examining referential adequacy, and confirming interpretations and thematic findings against the raw data. Thick descriptions by repeated independent reflections and discussion within the research team helped ensure transferability and confirmability. All steps of the research process were documented to provide a clear audit trail, and participants' direct quotes were used to present the findings. Also, study processes and products were externally audited to increase the dependability of the data.
Ethical ConsiderationsParticipants were assured that their information would remain confidential and that their care at the VCT would not be affected by their participation in the study. Participants could terminate the interview whenever they wanted. Given the stigma around HIV in Kerman, coupled with participants' concerns about “signing documents,” only verbal informed consent was obtained from the participants. Participants also consented to audio-recording of the interviews. No patient information or experiences were shared with the VCT staff, and all the information collected was stored in the research institute's private server, inside a password-protected folder. The ethics committee of Kerman University of Medical Sciences reviewed and approved the study protocol (Ethical code: IR.KMU.REC.1398.631).
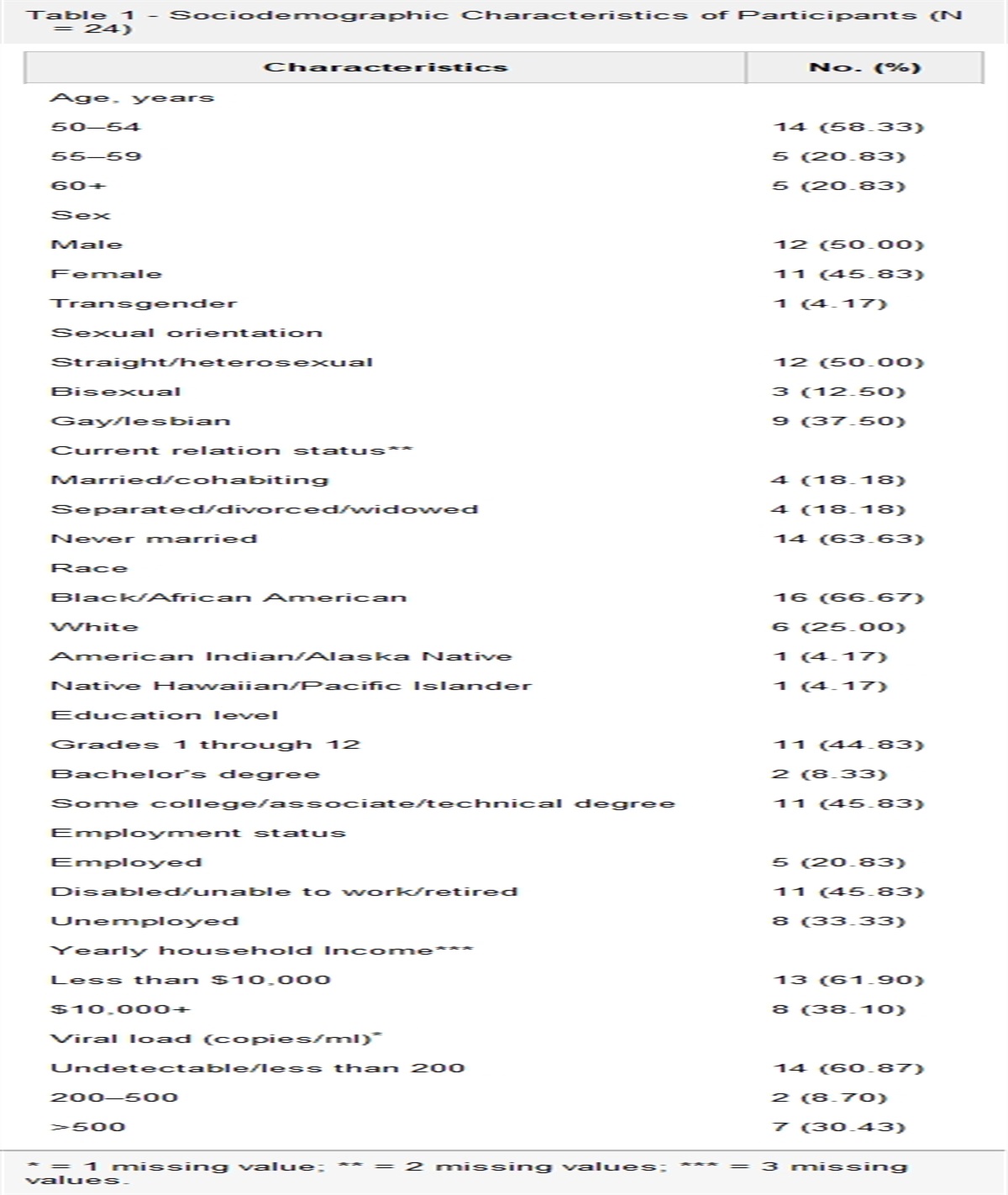
ResultsA total of 21 potential participants were approached, and 18 (85.7%) consented to participate. Three people refused to participate because of time constraints. The mean (SD) age of the participants was 43.7 (7.5) years. Most participants had an educational level of high school or less (66.7%), were married (44.4%), were unemployed (72.2%), and had a monthly income of less than or equal to $20 USD (Table 1). None of the participants reported having tested positive for SARS-CoV-2 by the interview date.
Table 1. - Demographic Characteristics (N = 18) Characteristics Number (%) Age (M ± SD) Total (43.7 ± 7.5) Men (45.8 ± 6.4) Women (42.0 ± 8.1) Age group, year 30–40 4 (22.2) 41–50 11 (61.1) 51–60 3 (16.7) Gender Men 8 (44.4) Women 10 (55.6) Marital status Married 8 (44.4) Single 4 (22.2) Separated/widowed 6 (33.4) Education High school or less 12 (66.7) High school diploma or academic 6 (33.3) Occupation Unemployed 5 (27.8) Housewife 8 (44.4) Other occupations 5 (27.8) Monthly income (USD)a ≤20 12 (66.7) 21–40 4 (22.2) ≥41 2 (11.1)aAverage income in Kerman: $219 (USD) in 2019.
The impact of COVID-19 on PLWH was classified into six themes: COVID-19–related knowledge and preventive practices, misconceptions about COVID-19, psychosocial effects, fear of seeking health care services, limited access to health care services, and the impact of COVID-19 on socioeconomic status. Details related to participants' pseudonyms, age, and educational level are provided in brackets after each quote.
COVID-19 Knowledge and Preventive PracticesMost participants were knowledgeable about COVID-19 symptoms and routes of transmission and that living with HIV might put them at a higher risk of adverse COVID-19–related outcomes. Participants had primarily accessed their information through media, the COVID-19–related educational campaigns on the national TV and radio channels, and the VCT center.
A married woman who was worried about her health during the COVID-19 pandemic said,
I follow the media and news as much as possible. I know that people with diseases like diabetes and high blood pressure are at a higher risk of severe outcomes. Of course, as someone living with HIV, I am more at risk than others, because my immune system is weak. (Leila, 42 years old, high school diploma)
Some participants highlighted the role of VCT centers in providing them with accurate information about COVID-19. An unemployed man who was knowledgeable about COVID-19 preventative measures said,
During the COVID-19 pandemic, whenever I visited the VCT, they emphasized on using masks. They also provided helpful information about proper hand washing and respiratory etiquette. (Asghar, 52 years old, primary school degree)
Preventive measures were closely followed when participants accessed HIV care. Indeed, participants reported adhering to guidelines about physical distancing, washing hands, and wearing masks, even when they could hardly afford them. A married woman who was experiencing financial problems said,
Although I lost my job because of the pandemic and face lots of financial hardship, buying masks is a must. I always wear a mask when I go out because I know that the virus can transmit through breathing, and I should follow the public health guidelines as much as possible. (Atoosa, 38 years old, high school diploma)
Two men seemed to worry not only about their own health but the health of their family and close friends. For example, a single man described his worries about his family contracting SARS-CoV-2 as a primary motive for practicing physical distancing while seeking care,
The virus can be transmitted from a person to another and some patients may be asymptomatic. That is why we must maintain physical distancing. You cannot tell if someone is positive or not. Therefore, every time during the epidemic, when I am going to get my medicines, I keep my distance from other clients and wear a face mask. I know if I get infected, the health of my family and those around me will definitely be in danger. (Paymaan, 41 years old, high school diploma)
Misconceptions About COVID-19Two unemployed men had significant misconceptions about using drugs and masks to prevent COVID-19 during the pandemic. Misconceptions were more frequent in older (>40 years of age) and less educated (<high school diploma) PLWH.
Some of the misconceptions reflected the widespread misunderstanding that COVID-19 does not affect people with substance use disorders. Indeed, a single man declared to have increased his substance use since the beginning of the pandemic because he believed it would protect him against COVID-19, in addition to its mood-altering effects. He said,
I have heard from peers that opioids can prevent COVID-19 and addicts do not get infected. So, I have increased my opium use during this time as a protective behaviour. It also helps me cope with all the shit I am going through. (Asghar, 52 years old, primary school degree)
One of the participants was a man who was married, had lost his trust in public health messaging, and questioned the validity of preventative recommendations about SARS-CoV-2 transmission. He said,
We are just told to wear a mask, but I believe these [masks] are useless and cannot prevent us from getting infected. If we are supposed to get sick, this will happen and the masks are unhelpful, because I have seen a lot of people around me who used masks and followed public health guidelines, but eventually got COVID-19. (Hassan, 42 years old, high school diploma)
Other participants, however, had a higher self-perceived risk for contracting SARS-CoV-2 because of their pre-existing behaviors and made some behavior modifications to reduce their risk. For example, a married housewife woman said,
Given that I smoke hookah, my lungs are not in a good shape. Therefore, I have to be very careful, and that is why I have reduced hookah smoking. (Mojgan, 32 years old, high school diploma)
Psychosocial EffectsPsychosocial effects were quite challenging for the participants. Participants reported mental distress because of limited social interactions, bans on hosting/attending social events, and fear of contracting SARS-CoV-2.
A married woman who had a busy social life before the pandemic experienced anxiety and insomnia because of COVID-19. She said,
Before COVID-19, I frequently visited my friends, family members, and even my neighbors. Meeting them made me think less about my problems and positively impacted my mood. However, during the COVID-19 pandemic, I cannot easily and frequently meet them and feel very lonely and depressed. On the other hand, I think to myself, if somebody is infected with COVID-19 in our gatherings, I will be terribly upset. In general, during this period, being isolated from family and friends have led to my difficulty sleeping and increased anxiety. (Elham, 39 years old, university degree)
Another man explained how his fear of contracting SARS-CoV-2 has adversely affected his life.
During this time, even if I have a simple fever, I get so stressed out and panic that I might have COVID-19. One day, I woke up with the minor symptoms of the common cold but called my doctor immediately to get tested for COVID-19. The doctor advised me to seek COVID-19 testing if the symptoms did not subside. I ended up feeling better the next day and did not go for a test. I was extremely fearful that day. (Mohammad, 45 years old, primary school degree)
Fear of Seeking Health Care ServicesParticipants' fear of contracting SARS-CoV-2 affected their seeking of health care services. Three women mentioned that they had limited their health care service usage, especially governmental services, during the pandemic. They reported limiting their use of both general health care and HIV treatment services.
A housewife and married woman reported how she had preferred to endure her pain and rely on self-medication, rather than health care, during the pandemic. She said,
I had a painful toothache, but I did not go to the health center. I took an antibiotic and pain medications to deal with my toothache. I was so afraid of acquiring the [SARS-CoV-2] virus. (Nasrin, 40 years old, high school diploma)
Another woman talked about her negative perceptions of public health care settings and how she preferred to seek care in private settings because they were less crowded, despite the higher costs associated with private health care services. She said,
Once, I had a severe stomachache. However, as my immune system is weakened because of HIV, I was afraid to go to the public health centers. Those places are dangerous and super crowded. I decided to go to a private clinic, which cost me a fortune. (Mojgan, 32 years old, high school diploma)
Reluctance to seek HIV care was also reported by a participant who had delayed obtaining her ART medication because of her fear of the VCT setting. This married woman said,
I was afraid of going to the VCT to get my HIV medicine. I thought it would be crowded, so if I went there, I would definitely get the infection. However, when I went to the VCT, I realized that my fears were unfounded. Because I got an appointment in advance and received the service in a few minutes. (Zohreh, 41 years old, high school diploma)
Limited or Inconvenient Access to Health ServicesCOVID-19 had serious implications for patients' access to health care because of disruptions in the public transport system.
A single and unemployed man explained how he could not receive services at the VCT because of the COVID-19–related delays in the public transit system. He said,
One day I wanted to go to the VCT for a blood test. I had to wait for a long time, but the bus was a no show and taxis were basically non-existing. Therefore, I could not complete my test that day. Public transit sucks because of COVID-19. (Asghar, 52 years old, primary school degree)
These concerns were also reflected in another single man's experience who complained about the reduced availability of public transit in the city and how inconvenient it has been for him to access care. He said,
I often went to the VCT center by public transport. However, during the COVID-19 pandemic, their working hours are reduced, and sometimes even public transportation is shut down for a few weeks. I cannot walk due to my illness [HIV] and other disabilities. It is really frustrating. (Mehdi, 41 years old, middle school degree)
Socioeconomic StatusSeveral participants mentioned that the impact of COVID-19 on their livelihood and financial stability has been enormous. Most had lost their already low-wage jobs or had a partner who was laid off because of COVID-19.
A married housewife woman explained how her family was having a hard time making ends meet and keeping a roof over their heads.
My husband is a bus driver assistant. Since the beginning of the pandemic, the rate of intercity travel has declined drastically, and people rarely travel by bus because of their fear of potential exposure to COVID-19 inside the bus. Therefore, my husband was laid off. We did not have enough money to pay the rent or afford our basic needs. We even struggle with putting food on the table. We had to borrow money from my brother whom also lost his job a few months into the pandemic. (Atoosa, 32 years old, high school diploma degree)
Another married woman who used to babysit to support herself and her family described how she lost her job because of COVID-19.
I was a babysitter. The baby's parents wanted me to stay with them 24/7 to ensure that I am not exposed to COVID-19 or bring the virus into their home. I obviously could not accept that as I am married and have a family of my own. I therefore, lost my job. (Asal, 38 years old, high school degree)
DiscussionThis is the first qualitative study to describe the lived experiences of PLWH during the COVID-19 pandemic in Iran. In summary, participants were generally knowledgeable about preventative measures against COVID-19; however, they did endorse certain misconceptions. The COVID-19 pandemic has negatively affected PLWHs' use of and access to health care services. Participants experienced emotional distress because of their isolation and socioeconomic deprivation posed by the government's restrictive policies and regulations since the beginning of the pandemic.
We found that participants were knowledgeable about COVID-19 and its routes of transmission and related preventive measures. Sufficient COVID-19–related knowledge among PLWH can be attributed to community education through the media and online platforms. Although some participants held misconceptions about some of the public health guidelines (e.g., effectiveness of face masks), others assumed opioids help protect them against COVID-19. The finding about the protective effect of opioids and COVID-19 is particularly concerning in the context of Kerman, where there is a social tolerability and acceptance toward opioid use (Zolala et al., 2016).
Misconceptions, possibly stemming from widespread COVID-19 misinformation and the attendant infodemic (Erku et al., 2020; Orso et al., 2020), have also been reported in other studies among the general population in Iran (Bastani & Bahrami, 2020). Indeed, a study conducted in Kerman that made flawed claims about the protective role of opium use against COVID-19 was distributed widely across different social media platforms before it was retracted (Khoshab & Rajabalipour, 2020). WHO has emphasized the importance of tackling misinformation and disinformation in the COVID-19 era by ensuring that public health messages are based on evidence, information is translated into actionable behavior change, and the information needs of specific communities are understood (Eysenbach, 2020; Zarocostas, 2020). These approaches could be incorporated into health care provision for PLWH to ensure they are adequately equipped to protect themselves against SARS-CoV-2. Although some approaches already exist in Iran (e.g., guidelines and protocols, educational websites and mobile phone applications, COVID-19 information call centers, and educational programs in national media and statewide TV), there is room for improvement and expansion of these approaches (Raoofi et al., 2020).
We found that PLWHs' mental health was adversely affected by several factors, including stress, anxiety, insomnia, home isolation, loss of social support, and financial hardships. Although these experiences are not unique to PLWH (Thombs et al., 2020; Xiong et al., 2020), they are additionally affected by pre-existing social and financial vulnerabilities. Although similar studies of the impact of COVID-19 on PLWH in Iran or other Middle Eastern countries are unavailable at the time of writing this article, our findings are comparable with studies elsewhere that have documented elevated anxiety and stress because of reduced access to care and disruption of adherence to treatment (Ballivian et al., 2020; Joska et al., 2020).
Several participants reported that their access to health care services was inconvenient and adversely affected during the COVID-19 pandemic. Although some preferred to stay at home because of their fear of contracting SARS-CoV-2 and willingly avoided seeking care, others had difficulty accessing care because of reductions in public transit. Reduced access to HIV care is of utmost concern, given the increased risk of opportunistic infections among PLWH and elevated risk of HIV transmission among people whose access to ART is reduced or disrupted (Osler et al., 2020; Shiau et al., 2020; Takada et al., 2020). Although one immediate response is to provide PLWH with the required amount of ART for several months and telemedicine care, this option is not feasible in many LMICs.
Participants also reported financial losses related to the pandemic. In the years before the pandemic, the number of Iranians living in poverty had been increasing, and the country's economy had significantly contracted partly because of economic sanctions in the United States (The World Bank, 2020). The pandemic has exacerbated these economic conditions by driving unemployment and skyrocketing inflation rates (Nada, 2020). A national survey of 1,563 Iranian adults conducted in April 2020 reported that 50.7% of the participants had their income slashed, 42% had their businesses closed, and 13.5% had lost their jobs (Nada, 2020). Our participants predominantly came from a resource-limited background and reported severe losses related to COVID-19, including food and housing insecurity. Our findings suggest that the pandemic may disproportionately affect resource-limited PLWH in Iran because most are not employed by the government and do not have a stable salary (Minister of Health & Wellness, 2020). Therefore, the government should take measures to improve the well-being of PLWH during the COVID-19 pandemic, including providing support packages (e.g., medication and food packages) for this particular group. Moreover, delivering ART and food packages to their doorstep may help reduce their dependence on public transit and address their concerns about seeking care at VCT centers.
LimitationsOur findings were based on a convenience sample of persons referred to a VCT center in Kerman; thus, generalizability may be limited. People who do not have access to the VCT center in Kerman or reside in other parts of the country may report different experiences. For example, the clients of the VCTs are generally of low socioeconomic status, and their experiences may differ from those of higher socioeconomic status who have access to HIV care and services in the private health care sector. Moreover, given the evolving nature of COVID-19 in Kerman, the impact and experiences of the study participants reflect a snapshot in time and may not reflect other periods or their current situation. We did not explore the gender-specific experiences of PLWH and did not collect data on duration of HIV infection. Future studies that consider gender and length of infection are needed. We also do not have information about how or if the number of clients receiving services at the VCT dropped after the COVID-19–related restrictions were implemented. In addition, we did not ask the participants about the length of their bus ride or distance between home and VCT. Such information would be beneficial to collect in future studies examining PLWHs' access to care facilities. Finally, given the COVID-19–related restrictions and concerns, we did not share the study report with the participants for validity testing.
ConclusionIn Kerman, the COVID-19 pandemic has had many negative effects on PLWH. Restrictive measures, social isolation, and financial hardships may disproportionately affect this low-resource population and limit their access to and use of health care services. Our findings support investments to strengthen the HIV care infrastructure to maintain the well-being of PLWH during these challenging times. Disruptions in PLWHs' access to HIV care and treatment may not only increase morbidity and mortality but could also diminish recent progress in HIV testing, treatment, and achieving viral suppression.
DisclosuresThe authors report no real or perceived vested interests related to this article that could be construed as a conflict of interest.
Author ContributionsAll authors on this article meet the four criteria for authorship as identified by the International Committee of Medical Journal Editors (ICMJE); all authors have contributed to the conception and design of the study, drafted or have been involved in revising this manuscript, reviewed the final version of this manuscript before submission, and agree to be accountable for all aspects of the work. Specific roles are listed below: Conceptualization: Z. Jaafari, H. Sharifi, and M. Karamouzian; Data curation: Z. Jaafari and M. Karamouzian; Formal analysis: Z. Jaafari, S. Eybpoosh, H. Sharifi, and M. Karamouzian; Funding acquisition: H. Sharifi; Investigation: Z. Jaafari, S. Eybpoosh, H. Sharifi, and M. Karamouzian; Methodology: Z. Jaafari, H. Sharifi, and M. Karamouzian; Project administration: Z. Jaafari, H. Sharifi; Resources: H. Sharifi, and M. Karamouzian; Software: Z. Jaafari; Supervision: H. Sharifi and M. Karamouzian; Validation: Z. Jaafari, S. Eybpoosh, H. Sharifi, and M. Karamouzian; Writing—original draft: Z. Jaafari and M. Karamouzian; Writing—review and editing: Z. Jaafari, S. Eybpoosh, H. Sharifi, and M. Karamouzian. Key Considerations Targeted education interventions are needed to counter misconceptions about mask wearing or the protective effects of substance use against coronavirus disease 2019 (COVID-19) among people living with HIV (PLWH). Medication and food packages are essential to be delivered to PLWH who are experiencing financial hardship as a result of COVID-19–related restrictions. National policies are needed to address PLWHs' reduced use of and access to health care services because of COVID-19–related restrictions.
AcknowledgmentsThe authors are thankful to the staff of VCT centers in Kerman city, as well as all individuals who participated in this study. Kerman University of Medical Sciences provided financial support to this project (Grant Number: 98001029; PI: Hamid Sharifi).
References Adepoju P. (2020). Tuberculosis and HIV responses threatened by COVID-19. The Lancet HIV, 7(5), e319-e320. https://doi.org/10.1016/s2352-3018(20)30109-0 Bain L. E., Nkoke C., Noubiap J. J. N. (2017). UNAIDS 90-90-90 targets to end the AIDS epidemic by 2020 are not realistic: Comment on “Can the UNAIDS 90-90-90 target be achieved? A systematic analysis of national HIV treatment cascades.” BMJ Global Health, 2(2), e000227. https://doi.org/10.1136/bmjgh-2016-000227 Ballivian J., Alcaide M. L., Cecchini D., Jones D. L., Abbamonte J. M., Cassetti I. (2020). Impact of COVID–19-related stress and lockdown on mental health among people living with HIV in Argentina. JAIDS Journal of Acquired Immune Deficiency Syndromes, 85(4), 475-482. https://doi.org/10.1097/QAI.0000000000002493 Bastani P., Bahrami M. A. (2020). COVID-19 related misinformation on social media: A qualitative study from Iran. Journal of Medical Internet Research, [Preprints]. https://doi.org/10.2196/18932 Bengtsson M. (2016). How to plan and perform a qualitative study using content analysis. NursingPlus Open, 2, 8-14. https://doi.org/10.1016/.jnpls.2016.01.001 Centers for Disease Control and Prevention. (2020). What to know about HIV and COVID-19. https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/hiv.html Del Amo J., Polo R., Moreno S., Díaz A., Martínez E., Arribas J. R., Jarrín I., Hernán M. A. (2020). Incidence and severity of COVID-19 in HIV-positive persons receiving antiretroviral therapy: A cohort study. Annals of Internal Medicine, 173(7), 536-541. https://doi.org/10.7326/M20-3689 Dyer J., Wilson K., Badia J., Agot K., Neary J., Njuguna I., Kibugi J., Healy E., Beima-Sofie K., John-Stewart G. (2021). The psychosocial effects of the COVID-19 pandemic on youth living with HIV in Western Kenya. AIDS and Behavior, 25(1), 68-72. https://doi.org/10.1007/s10461-020-03005-x Erku D. A., Belachew S. A., Abrha S., Sinnollareddy M., Thomas J., Steadman K. J., Tesfaye W. H. (2020). When fear and misinformation go viral: Pharmacists' role in deterring medication misinformation during the'infodemic'surrounding COVID-19. Research in Social and Administrative Pharmacy, 17(1), 1954-1963. https://doi.org/10.1016/j.sapharm.2020.04.032 Eysenbach G. (2020). How to fight an infodemic: The four pillars of infodemic management. Journal of Medical Internet Research, 22(6), e21820. https://doi.org/10.2196/21820 Hochstatter K. R., Akhtar W. Z., Dietz S., Pe-Romashko K., Gustafson D. H., Shah D. V., Krechel S., Liebert C., Miller R., El-Bassel N. (2021). Potential influences of the COVID-19 pandemic on drug use and HIV care among people living with HIV and substance use disorders: Experience from a pilot mHealth intervention. AIDS and Behavior, 25(2), 354-359. https://doi.org/10.1007/s10461-020-02976-1 Hogg R. S. (2018). Understanding the HIV care continuum. The Lancet HIV, 5(6), e269-e270. https://doi.org/10.1016/s2352-3018(18)30102-4 Hooshyar S. H., Ranjbar E., Sharifi H., Shafiei M., Tayeri K., Haghdoost A., Rutherford G. W., Mirzazadeh A. (2018). Evaluating the HIV continuum of care and treatment in a low prevalence city in Iran: Kerman HIV-Friendly City initiative. East African Journal of Applied Health Monitoring and Evaluation, 7(2)1-10. http://eajahme.com/evaluating-the-hiv-continuum-of-care-and-treatment-in-a-low-prevalence-city-in-iran-kerman-hiv-friendly-city-initiative/. Jiang H., Zhou Y., Tang W. (2020). Maintaining HIV care during the COVID-19 pandemic. The Lancet HIV, 7(5), e308-e309. https://doi.org/10.1016/s2352-3018(20)30105-3 Joska J. A., Andersen L., Rabie S., Marais A., Ndwandwa E.-S., Wilson P., King A., Sikkema K. J. (2020). COVID-19: Increased risk to the mental health and safety of women living with HIV in South Africa. AIDS and Behavior, 24(10), 2751-2753. https://doi.org/10.1007/s10461-020-02897-z Karamouzian M., Madani N., Doroudi F., Haghdoost A. A. (2017). Improving the quality and quantity of HIV data in the Middle East and North Africa: Key challenges and ways forward. International Journal of Health Policy and Management, 6(2), 65-69. https://doi.org/10.15171/ijhpm.2016.112 Khalili M., Karamouzian M., Nasiri N., Javadi S., Mirzazadeh A., Sharifi H. (2020). Epidemiological characteristics of COVID-19: A systematic review and meta-analysis. Epidemiology and Infection, 148. https://doi.org/10.1017/s0950268820001430 Khoshab H., Rajabalipour M. (2020). The relationship between opium use and coronavirus infection: A brief research report from Iran. Coronaviruses, 1(1). https://doi.org/10.2174/2666796701999200607202523 Lincoln Y. S., Guba E. G. (1985). Naturalistic inquiry. India: Sage Publication, Inc. Marbaniang I., Sangle S., Nimkar S., Zarekar K., Salvi S., Chavan A., Gupta A., Suryavanshi N., Mave V. (2020). The burden of anxiety among people living with HIV during the COVID-19 pandemic in Pune, India. BMC Public Health, 20(1), 1-9. https://doi.org/10.1186/s12889-020-09656-8 MAXQDA Software. (n.d.). MAXQDA 10. https://www.maxqda-press.com/ Minister of Health & Wellness. (2020). National HIV/STI/TB programme. https://hstu.moh.gov.jm/media/reports/ Mirzaei H., McFarland W., Karamouzian M., Sharifi H. (2021). COVID-19 among people living with HIV: A systematic review. AIDS and Behavior, 25(1), 85-92. https://doi.org/10.1007/s10461-020-02983-2 Orso D., Federici N., Copetti R., Vetrugno L., Bove T. (2020). Infodemic and the spread of fake news in the COVID-19-era. European Journal of Emergency Medicine. 27(5), 327-328. https://doi.org/10.1097/MEJ.0000000000000713 Osler M., Cornell M., Ford N., Hilderbrand K., Goemaere E., Boulle A. (2020). Population‐wide differentials in HIV service access and outcomes in the Western Cape for men as compared to women, South Africa: 2008 to 2018: A cohort analysis. Journal of the International AIDS Society, 23(S2), e25530. https://doi.org/10.1002/jia2.25530 Poustchi H., Darvishian M., Mohammadi Z., Shayanrad A., Delavari A., Bahadorimonfared A., Eslami S., Javanmard S. H., Shakiba E., Somi M. H. (2020). SARS-CoV-2 antibody seroprevalence in the general population and high-risk occupational groups across 18 cities in Iran: A population-based cross-sectional study. The Lancet Infectious Diseases, 21(4), 473-481. https://doi.org/10.1016/S1473-3099(20)30858-6 Raoofi A., Takian A., Sari A. A., Olyaeemanesh A., Haghighi H., Aarabi M. (2020). COVID-19 pandemic and comparative health policy learning in Iran. Archives of Iranian Medicine, 23(4), 220-234. https://doi.org/10.34172/aim.2020.02 Saunders B., Sim J., Kingstone T., Baker S., Waterfield J., Bartlam B., Burroughs H., Jinks C. (2018). Saturation in qualitative research: Exploring its conceptualization and operationalization. Quality & Quantity, 52(4), 1893-1907. https://doi.org/10.1007/s11135-017-0574-8 SeyedAlinaghi S., Taj L., Mazaheri-Tehrani E., Ahsani-Nasab S., Abedinzadeh N., McFarland W., Mohraz M., Mirzazadeh A. (2021). HIV in Iran: Onset, responses, and future directions. AIDS, 35(4), 529-542. https://doi.org/10.1097/qad.0000000000002757 Shiau S., Krause K. D., Valera P., Swaminathan S., Halkitis P. N. (2020). The burden of COVID-19 in people living with HIV: A syndemic perspective. AIDS and Behavior, 24(8), 2244-2249. https://doi.org/10.1007/s10461-020-02871-9 Statistical Center of Iran. (2016). Detailed results of the general population and housing census 2016. http://kerman.mporg.ir Takada S., Ettner S. L., Harawa N. T., Garland W. H., Shoptaw S. J., Cunningham W. E. (2020). Life chaos is associated with reduced HIV testing, engagement in care, and ART adherence among cisgender men and transgender women upon entry into jail. AIDS and Behavior, 24(2), 491-505. https://doi.org/10.1007/s10461-019-02570-0 The World Bank. (2020). The Iranian authorities have adopted a comprehensive strategy encompassing the market-based reforms reflected in the government's 20-year vision and its sixth development plan for the full five-year period from 2016/17 to 2021/22. https://www.worldbank.org/en/country/iran/overview Thomas D. R. (2006). A general inductive approach for analyzing qualitative evaluation data. American Journal of Evaluation, 27(2), 237-246. https://doi.org/10.1177/1098214005283748 Thombs B. D., Bonardi O., Rice D. B., Boruff J. T., Azar M., He C., Markham S., Sun Y., Wu Y., Krishnan A. (2020). Curating evidence on mental health during COVID-19: A living systematic review. Journal of Psychosomatic Research, 133. https://doi.org/10.1016/j.jpsychores.2020.110113 UN News. (2020). Global HIV toll likely to be far higher owing to COVID-19, warns UNAIDS. https://news.un.org/en/story/2020/11/1078622 UNAIDS. (2020b). Rights in a pandemic – Lockdowns, rights and lessons from HIV in the early response to COVID-19. https://www.unaids.org/en/re
留言 (0)