
記住我

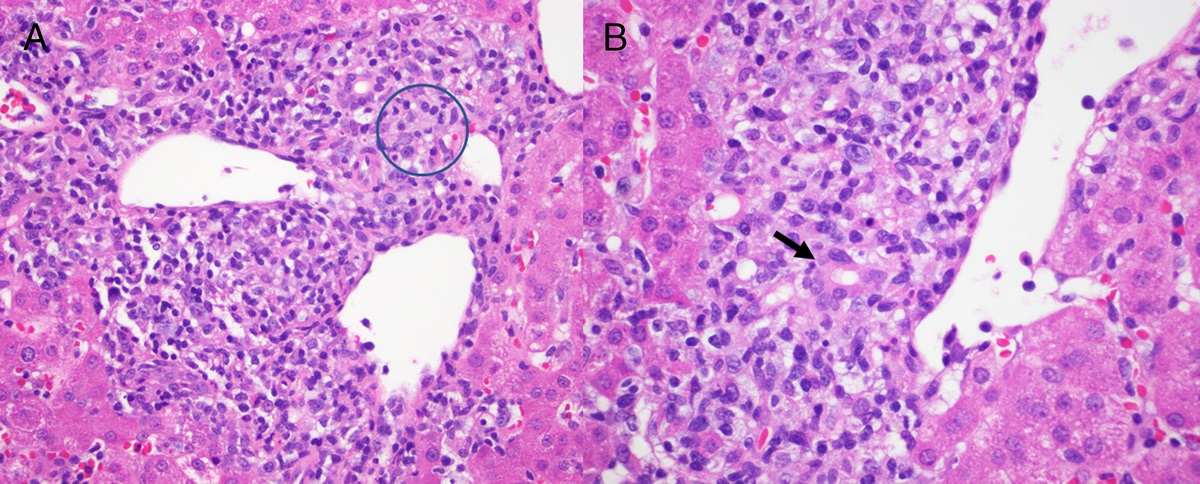

A 57-year-old woman presented to her gastroenterologist for dysphagia. She underwent an esophagogastroduodenoscopy, which revealed a hiatal hernia, mild antral gastritis, retained food debris in the esophagus, and possible Candida esophagitis. The remainder of the stomach and the duodenum were endoscopically unremarkable. Biopsies of the esophagus and gastric antrum were performed (case 1). Multiple fragments within the stomach biopsy revealed mild chronic inactive gastritis; however, 1 fragment of adenocarcinoma was present among the multiple benign gastric tissue fragments (Fig. 1). No benign tissue was attached to the tumor fragment. Given the discordance between the histologic findings and the benign endoscopic findings, an investigation of possible tissue contamination ensued.
 FIGURE 1:
FIGURE 1: Case 1 with contaminating tumor fragment (arrow) among multiple fragments of benign gastric mucosa. Upper left inset shows a medium power view of the contaminating tumor fragment (H&E stain, original magnification ×20; inset, ×200).
First, the fragment of malignant gastric tissue was confirmed to be within the paraffin tissue block after review of a hematoxylin and eosin (H&E)–stained recut slide. Next, the case was shared with multiple pathologists who reviewed the H&E slides with contaminating tumor to develop a differential diagnosis for the tumor type/organ of origin. The pathologists favored gastric or gastroesophageal junction origin, followed by a duodenal or pancreaticobiliary source.
A search to identify the source case of contaminating tissue using the electronic medical record laboratory information system (LIS) included review of the surgical pathology cases collected, grossly examined, processed, and embedded near the date of the contaminated gastric biopsy. Two-hundred thirty-four surgical pathology cases with malignant diagnoses spanning a 7-day period including dates before and after the biopsy were further filtered to 58 cases that were collected, grossed, and processed on the same date or the day before the contaminated gastric biopsy case. Pathology reports from all 58 cases were reviewed, and the slides from the 13 cases of adenocarcinoma were reviewed. In addition, slides from the 100 blocks embedded immediately before the contaminated block and the 50 blocks after were reviewed.
Upon histologic review, 1 case (case 2) was favored to represent a possible source of contamination and was composed of 3 biopsy specimens: an esophageal mass, distal esophageal mass, and gastric cardia mass. Endoscopy from this case described an ulcerated and friable mass extending from the distal esophagus to the gastric cardia. Histologically, adenocarcinoma involved 16 tissue fragments (Fig. 2) from the 3 specimens and had a similar appearance to the tumor fragment from case 1. Case 2 was collected, grossly examined, processed, and embedded in a relatively short period before case 1.
 FIGURE 2:
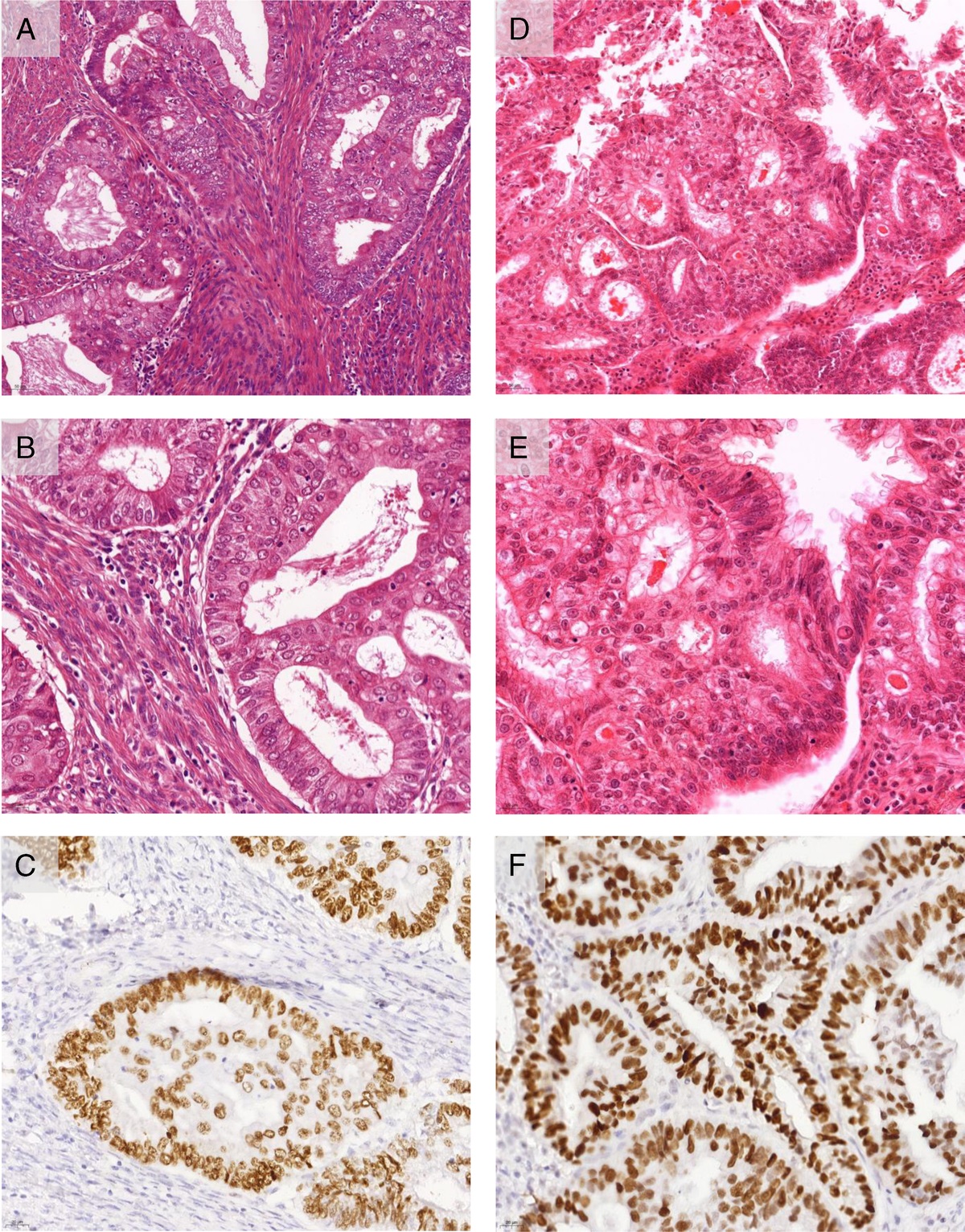
FIGURE 2: Case 2 showing multiple tumor fragments of gastroesophageal junction adenocarcinoma. Upper left inset shows a representative high-power view of the adenocarcinoma, which is morphologically similar to the contaminating tumor fragment in case 1 (H&E stain, original magnification ×20; inset, ×400).
Blocks from both cases were sent for DNA genotyping by evaluation of 15 short tandem repeat loci and a sex determination locus. Different genetic profiles were identified between the single fragment of adenocarcinoma and the fragments of benign gastric mucosa in case 1. In addition, case 2 had an identical genotype at all loci to the contaminating fragment of adenocarcinoma from case 1. Given the times and dates of collection, grossing, processing, and embedding of these 2 cases, it was favored that contamination most likely occurred at specimen collection or gross examination.
DISCUSSIONThe general sequence of events pertaining to surgical pathology specimens includes specimen collection, transport to the laboratory, accessioning, gross examination, processing, embedding, microtomy, staining, and coverslipping. Reported contamination rates within surgical pathology are reported up to 2.9%.1,2 In 1 study, neoplasm comprised 12.7% of contaminating tissues.1
Tissue contaminants are readily identified morphologically by the pathologist when the tissues originate from a different organ/anatomic site; however, morphologic distinction becomes increasingly difficult or even impossible when the tissues are from the same site. The attuned pathologist in case 1 recognized that the histologic findings were discrepant with the endoscopic findings and ultimately prevented a false-positive diagnosis.
Ideally, the investigation should evaluate all steps of the chain of custody from specimen collection to coverslipping, although laboratories may not have the capabilities within their electronic medical record or LIS to efficiently obtain these data. Our institution is utilizing the Epic (Verona, Wis) Beaker LIS, which provides good specimen-tracking capability in real time. Every task is logged with a time stamp, performing user, and location, providing direct oversight of the hands that touch the specimen container, tissue cassettes, paraffin blocks, and glass slides. When the LIS does not have good tracking capabilities, possessing an external mechanism of specimen-tracking system that may or may not interface with the LIS becomes of critical importance. In the past, our institution had used the Roche (Basel, Switzerland) Vantage workflow solution, and such third-party products provide an alternate and reasonably effective mechanism. Although the primary function of specimen-tracking systems is to provide measurable quality improvements in histology by reducing the number of process steps and the increasing productivity, it also provides the tracking data that become extremely important in cases of investigations for tissue contaminants, missing specimens, blocks, and slides.
Once a case is identified as a likely source of contamination, the simplest method of comparison is histologic evaluation. Other methods of determining tissue identity include immunohistochemical testing of blood cell antigens, human leukocyte antigen genotyping, and recently a digital pathology solution using an image search tool database.3–6 Currently, molecular genetic fingerprinting techniques are commonly used to resolve issues of tissue specimen identity.7–12
Benign mucosal biopsy contaminants (eg, 1 fragment of benign duodenum with multiple fragments of squamous mucosa in a specimen labeled “esophagus”) can occur and are presumed to represent contamination during the biopsy procedure. If the contaminating tissue is benign or otherwise without pathologic abnormality, a diagnosis can be rendered; however, there still may be value in investigating the source of these contaminants.13 Although most such contaminants do not impact patient care and may even be commonplace occurrences, it is imperative for a high-quality laboratory to make some effort to track these on a routine basis. Defining a source for these errors whether in the preanalytic workspace (operating room, endoscopy suites, etc) or the analytic workspace (specimen grossing or embedding) becomes quite critical.
The field of pathology is a service branch for the hospital, and any error in the preanalytic workspace is almost always initially blamed on analytic workspace, which is the laboratory. The laboratory may spend many hours each month to track down the source of these errors despite good specimen-tracking system capabilities. The source of these errors may be a single employee within the operating/endoscopy room, pathologists' assistant, or histotechnologist, but until data are collected systematically and continuously, the laboratory may spend countless hours in aggregate over a long period performing root-cause analysis for a serious safety event.
Laboratories have policies and procedures in place to prevent cross contamination at each step of processing. Several steps can be taken to prevent cross contamination within the surgical pathology laboratory, which are well described elsewhere.13 The use of biopsy bags or lens paper for small, delicate specimens is common practice, and these materials could also be utilized for large friable tissues. Grossing should proceed in an organized fashion with one specimen container at a time, double-checking that the specimen, paperwork, and cassettes match. When available, utilizing barcode scanning technology at any step within the laboratory is another tool to reduce errors.
Our presumption that the contaminating tissue in case 1 originated from another case with a malignant diagnosis allowed for efficient identification of potential sources; however, if the contaminating tissue fragment was the only tumor fragment from a different patient, it is unlikely we would have discovered the source of contamination. Even if we had not successfully identified the source of contamination case, we still could have proven with genotyping that the tumor fragment was from a different patient than the benign gastric fragments in the block.
In any instance of tumor tissue contamination, one must consider the possibility of a second patient with a false-negative pathologic diagnosis. This concern may be somewhat alleviated by the common occurrence of multiple tumor fragments in biopsies of a malignancy. In addition, if a clinician is sampling a highly suspicious mass, a benign pathologic diagnosis may lead to a phone call to the pathologist and/or rebiopsy of the mass.
Identifying the problem of tissue contamination and addressing it immediately are of utmost importance. Setting this case aside for later in the day may not be a good idea. Once the problem is identified, an immediate plan needs to be initiated. Utilizing the LIS to identify cases grossed by the pathologists' assistant and cases embedded by the histotechnologist in the preceding time periods should be followed by systematically reviewing the lists of cases to narrow down to potential candidates and reviewing those histology slides to find the closest match. One should also search for all cases originating from the particular operating room, endoscopy suite, or doctor's office on that particular and preceding day(s). Reviewing patients' charts and matching suspected clinical findings with the contaminant in question should be a quick and early assessment. Performing these actions within the first few days and finding the source of error quickly become of vital importance, especially when dealing with a cancer contaminant. Notifying a clinician of a potential contaminant should be an action of last resort after all these investigations prove futile.
CONCLUSIONHistologic tumor contaminants of the same tissue type can be difficult to identify as extraneous tissue. Errors may occur in the preanalytic space (operating rooms, endoscopy rooms, doctor's offices) or in the analytic workspace (grossing or embedding stations), and systematically ruling out these sources is important. The source of error should be detected ideally within 72 hours, or even earlier if possible, to avoid impact to patient care, as patients may receive unnecessary second procedures and treatment with risk of significant morbidity resulting from an incorrect diagnosis or potential for incorrect diagnosis being listed on the pathology report due to incomplete or poor workup.
Overall, the combination of clinical-histologic discordance, histologic assessment, review of surgical pathology laboratory processing logs in a focused time period, and molecular diagnostics allows for identification of contaminating tumor tissue.
REFERENCES 1. Gephardt GN, Zarbo RJ. Extraneous tissue in surgical pathology: a College of American Pathologists Q-Probes study of 275 laboratories. Arch Pathol Lab Med 1996;120:1009–1014. ProQuest. 2. Layfield LJ, Witt BL, Metzger KG, et al. Extraneous tissue: a potential source for diagnostic error in surgical pathology. Am J Clin Pathol 2011;136(5):767–772. 3. Ritter JH, Sutton TD, Wick MR. Use of immunostains to ABH blood group antigens to resolve problems in identity of tissue specimens. Arch Pathol Lab Med 1994;118:293–297. 4. Lagaaij EL, Cramer-Knijnenburg GF, Van der Pijl JW, et al. Rapid verification of the identity of questionable specimens using immunohistochemistry with monoclonal antibodies directed against HLA-class I antigens. Histopathology 1997;31:284–288. 5. Shibata D. Identification of mismatched fixed specimens with a commercially available kit based on the polymerase chain reaction. Am J Clin Pathol 1993;100:666–670. 6. Pantanowitz L, Michelow P, Hazelhurst S, et al. A digital pathology solution to resolve the tissue floater conundrum. Arch Pathol Lab Med 2021;145(3):359–364. 7. Tsongalis GJ, Wu AH, Silver H, et al. Applications of forensic identity testing in the clinical laboratory. Am J Clin Pathol 1999;112:93–S103. 8. Worsham MJ, Wolman SR, Zarbo RJ. Molecular approaches to identification of tissue contamination in surgical pathology sections. J Mol Diagn 2001;3(1):11–15. 9. Hunt JL, Swalsky P, Sasatomi E, et al. A microdissection and molecular genotyping assay to confirm the identity of tissue floaters in paraffin-embedded tissue blocks. Arch Pathol Lab Med 2003;127(2):213–217. 10. Venditti M, Hay RW, Kulaga A, et al. Diagnosis of ectopic tissue versus contamination by genetic fingerprinting in a routine surgical pathology specimen. Hum Pathol 2007;38(2):378–382. 11. Pfeifer JD, Zehnbauer B, Payton J. The changing spectrum of DNA-based specimen provenance testing in surgical pathology. Am J Clin Pathol 2011;135(1):132–138. 12. Bossuyt V, Buza N, Ngo NT, et al. Cancerous ‘floater’: a lesson learned about tissue identity testing, endometrial cancer and microsatellite instability. Mod Pathol 2013;26(9):1264–1269. 13. Hodgson AJ, Shang YM, Boulianne P, et al. A practical approach to investigating cross-contaminants in the anatomical pathology laboratory. Int J Surg Pathol 2020;28(7):700–710.
留言 (0)