
記住我







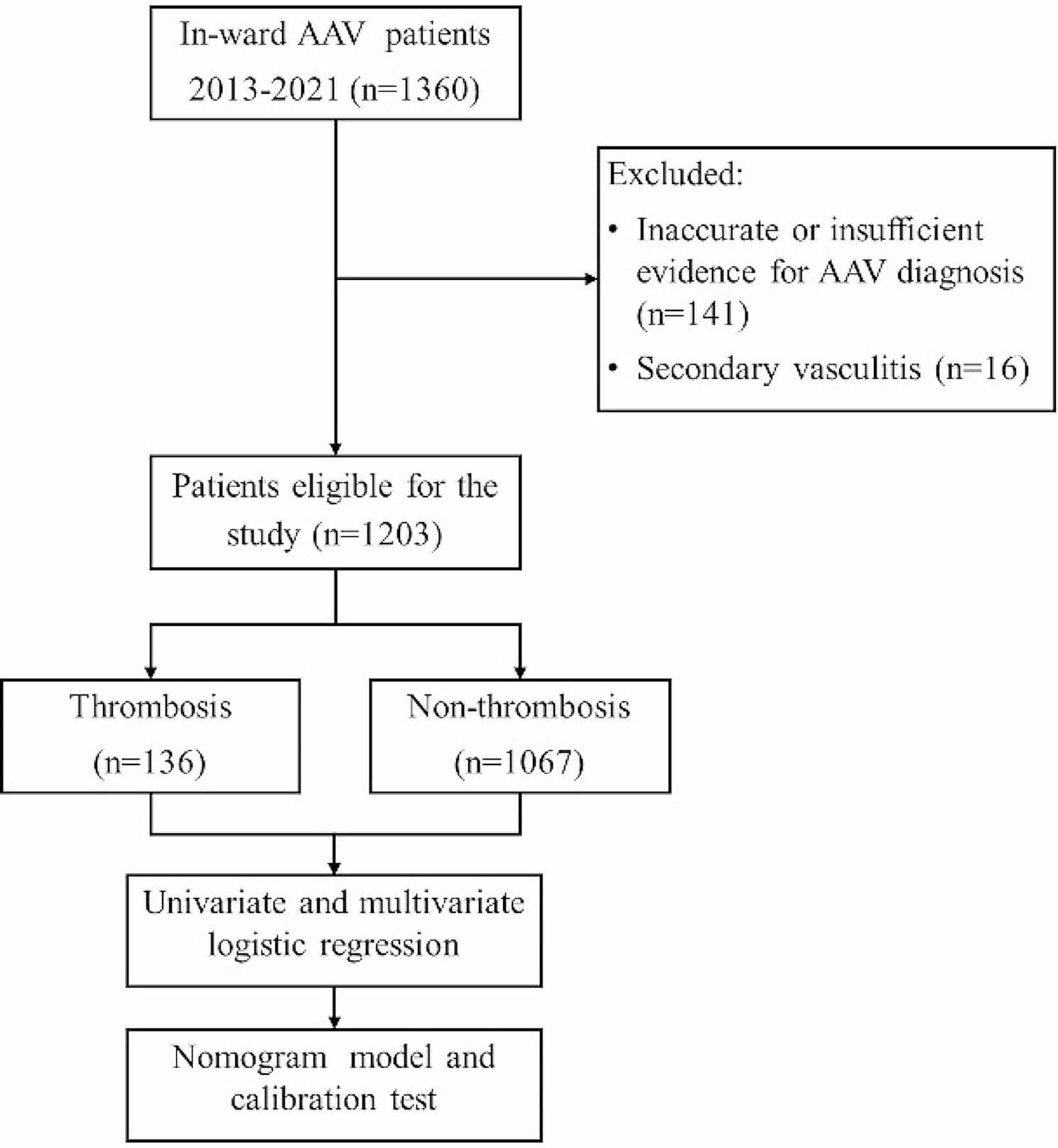
The present study retrospectively enrolled 70 severe acute respiratory failure patients receiving VV ECMO with hemorrhage risk in the First Affiliated Hospital of Zhengzhou University immediately from June 2012 to Sept 2020. 70 enrolled patients were divided into survival group (n = 25) and non-survival group (n = 45) (Fig. 1). In this study, the low heparin protocol was defined as 3000 units of heparin intravenously at the time of ECMO initiation and no ongoing heparin administration, as long as Δp were kept below 30 mmHg and Ppost-MLO2 were over 200 mmHg. ECMO system used was BE-PLS 2050 (Maquet, Rastatt, Germany). The cannulation of femoral vein and jugular vein were 17–25 French (Fr) cannulas.
Fig. 1
Inclusion criteria were: 1) VV-ECMO support longer than 24 h; 2) potentially hemorrhage risk (trauma, history of gastrointestinal or airway hemorrhage, and after surgery). The exclusion criteria were as follows: 1) aged<18 years old; 2) pregnancy; 3) irreversible multiple organ failure; 4) uncontrolled metastatic malignancy; 5) severe craniocerebral injury; 6) active bleeding; 7) preexisting indication for therapeutic anticoagulation; 8) contraindication to heparin; 9) missing informed consent.
ACT was measured at the initiation(0 h), 0.5 h, 1 h, 2hs, 4hs, 8hs, 16hs, 24hs, 48hs, 72hs, 96hs, 120hs, 144hs, 168hs, 192hs and 216hs after ECMO running. APTT, international normalized ratio (INR), D-dimer and Fibrinogen were measured at 0 h, 0.5 h, 8hs, 16hs, 24hs, 48hs, 72hs, 96hs, 120hs, 144hs, 168hs, 192hs and 216hs. The levels of platelet and lactate dehydrogenase (LDH) were measured at 0 h, 0.5 h, 24hs, 48hs, 72hs, 96hs, 120hs, 144hs, 168hs, 192hs and 216hs. The blood flow rate, the Δp and Ppost-MLO2 of membrane lung were recorded at 0.5 h, 1 h, 2hs, 4hs, 8hs, 16hs, 24hs, 48hs, 72hs, 96hs, 120hs, 144hs, 168hs, 192hs and 216hs. The routine Doppler of heart and thrombosis (inferior vena cava, deep and superficial arteries and veins of both lower extremities, jugular arteries and veins, as well as inside and outside the cannula) was repeated once a day in the patients during the ECMO assisted. The time of ECMO assisted, mechanical ventilation and intensive care unit (ICU) stay were collected. The severity of the illness was assessed based on the sepsis-related organ failure assessment (SOFA) score before ECMO initiation. Finally, the complications were recorded.
EndpointsThe primary endpoint was 30-day ICU mortality. Secondary endpoints were symptomatic thromboembolic events, ECMO oxygenator change and severe bleeding complications. The severe bleeding was defined as need for intervention or ≥ 10 red blood cell transfusions [8].
Routine threshold for platelet transfusion was < 50 × 109/L but could be individualized depending on the clinical situations. Fibrinogen or cryoprecipitate could be infused when the level of blood fibrinogen was less than 2 g/L. When the level of D-dimer was too high, tranexamic acid could be used in combination with the condition.
Oxygenator change was considered in the following situations: 1) decreasing Ppost-MLO2<200 mmHg with increasing transmembrane pressure gradient or Δp (=Ppre-ML- Ppost-ML)>30 mmHg; 2) increasing Ppost-MLCO2>40 mmHg and Ppre-MLCO2- Ppost-MLCO2<10 mmHg; 3) apparent circuit thrombosis with thrombi>5 mm; 3) rising D-dimers with progressive thrombocytopenia and hyperfbrinolysis with increasing transmembrane pressure gradient and 4) unexplained haemolysis with increasing transmembrane pressure gradient [9].
Statistical analysisAll collected data were statistically analyzed using SPSS 21.0 (Armonk, NY: IBM Corp.). Measurement data were expressed by the mean ± standard deviation (SD), and the two groups compared by analysis of variance. Count data were expressed by frequency (composition ratio), and comparison between groups was by χ2 test or Fisher’s exact test. P<0.05 indicates that the difference is statistically significant. The binary Logistic regression was conducted to analyze whether coagulation and hemolysis indicators have relationships with ICU mortality.
ResultsBaseline characteristics of VV ECMO patientsThe characteristics of 70 enrolled patients are shown in Table 1. The longest heparin-free time was 216 h, and the mean heparin-free time was 102 h. Compared with survivors, the non-survivors were showed higher baseline SOFA score ( 8 (6.5–11) vs. 5 (4–6), p = 0.001, Table 1), longer time in ICU (17.16 ± 9.95d vs. 23.15 ± 10.72d, p = 0.022, Table 1) and lower platelet counts in 0 h, 0.5 h, 24 h, 48 h and 96 h after ECMO applied (all p < 0.05; Table 1, Fig. 2). However, there was no significant differences between survivors and non-survivors in ACT, APTT, INR, D-dimer, Fibrinogen, LDH, blood flow rate, Δp and Ppost-MLO2 of all different time point (all p < 0.05; Table 1, Figs. 2 and 3).
Table 1 Baseline characteristics of acute respiratory failure patients assisted with VV-ECMOFig. 2
Compared of coagulation indicators in different time points between survivors and non-survivors. (A): ACT; (B): APTT; (C): INR; (D): Platelet; (E): D-dimer; (F): Fibrinogen; (G): LDH. The red arrows indicate statistical significance
Fig. 3
Compared of ECMO-related indicators in different time points between survivors and non-survivors. (A): blood flow rate; (B): Δp; (C): Ppost-MLO2
Besides, the cause of death has no relationship with thrombotic disease including pulmonary embolism, acute myocardial infarction or renal thrombosis in the present study.
Description and comparison of complications of VV ECMOThe percentage of thrombosis complications was 54.3% (38/70) including 3 oxygenator changed but there was no significant difference of complications in survival and non-survival groups ( all p>0.05, Table 2). In detail, the survivors were suffered 5 cases of membrane lung thrombosis, 4 cases of lower extremity venous thrombosis, 4 cases of venous cannula thrombosis, 1 case of ECMO circuit thrombosis and 1 case of oxygenator change. The non-survivors were appeared 11 cases of membrane lung thrombosis, 7 cases of lower extremity venous thrombosis, 3 cases of venous cannula thrombosis and 2 cases of oxygenator change. However, there was no bleeding complication occurred.
Table 2 Comparison of the complications of the survivors and non-survivors of acute respiratory failure patients assisted with VV-ECMOExplanations of oxygenator changed casesThe capacity of oxygen uptake was calculated as PpostO2, the capacity of carbon dioxide removal was showed as PpreCO2-PpostCO2, and the blood flow obstruction was described as Δp (Ppre-ML- Ppost-ML). The oxygenator changed case 1: BFR = 3.7 L/min (BFR of the last day was 4.3 L/min at the same rotating speed), SpostO2=89.2%, PpostO2=61 mmHg (< 200 mmHg), PpostCO2 = 49 mmHg, PpreCO2 = 40.2 mmHg, PpreCO2 -PpostCO2 = 8.8 mmHg (< 10 mmHg), Δp= 51 mmHg (> 30 mmHg). The oxygenator changed case 2: BFR = 3.8 L/min (BFR of the last day was 4.2 L/min at the same rotating speed), SpostO2 = 98%, PpostO2 = 82 mmHg (< 200 mmHg), PpostCO2 = 30.7 mmHg, PpreCO2 = 36 mmHg, PpreCO2 -PpostCO2 = 5.3 mmHg (< 10 mmHg), Δp = 39 mmHg (> 30 mmHg). The oxygenator changed case 3: BFR = 3.9 L/min (BFR of the last day was 4.2 L/min at the same rotating speed), SpostO2 = 96.2%, PpostO2 = 63 mmHg (< 200 mmHg), PpostCO2 = 31 mmHg, PpreCO2 = 37 mmHg, PpreCO2 -PpostCO2 = 6 mmHg (< 10 mmHg), Δp = 34 mmHg (> 30 mmHg).
The relationship between indicators and ICU mortalityThe baseline levels of ACT, APTT, INR, platelet, D-dimer, Fibrinogen, LDH and SOFA score were choose as variables for the binary Logistic regression analysis of VV ECMO supported patients’ ICU mortality. As shown in Fig. 4, only the baseline SOFA score was significantly associated with ICU mortality (2.754 (1.486–5.103), p < 0.001, Fig. 4).
Fig. 4
The binary Logistic regression analysis of mortality
留言 (0)