Main findings
Our study did not reveal a significant effect of having Raynaud’s phenomenon on work ability, when analyzed using multiple linear regression. Women with Raynaud’s phenomenon reported a slightly higher job retainment compared to those without the condition, and generally long working hours. There were no statistically significant differences in sick leave occurrence or duration.
Interpretation and comparison with other studies
The prevalence of RP in the present surveys was comparable with the roughly 12% that was reported in a Finnish population-based study [4]. The condition was more common among women, which is also in line with previous research [10]. Further, the mean age of onset of 31 years for women and 36 years for men was quite similar to the results of a meta-analysis on longitudinal studies on RP (10 studies; 639 subjects), where the mean age of onset was 34 years [22].
The present study did not show any significant effect of RP status on work ability in the multiple linear regression models, when also using age, BMI, physical workload, cardiovascular disease, and perceived stress as covariates. However, in unadjusted analyses, there was a significant positive effect of RP status on work ability among women. Also, the results of longitudinal analyses suggested that men with incident RP had a slightly lower work ability than healthy subjects, while women with remitted RP reported a lower work ability than those with persistent disease. It is plausible that RP is indeed a hindrance for work, especially in manual outdoor occupations where exposure to ambient and contact cold, as well as hand-arm vibration, can trigger vasospastic attacks. This might reduce the work capacity in tasks requiring grip force and manual dexterity, and motivate the worker to seek a heated environment in order to regain full use of the hands. Such manual outdoor occupations are common among working men in northern Sweden, as evidenced both by the descriptive analyses on occupation in this study (Table 1), as well as official statistics from the Swedish Work Environment Authority [23]. In contrast, women with RP reported long working hours and a higher job retainment than their healthy counterparts. These finding are harder to explain, but may be due to the fact that RP does not pose a hindrance for indoor work with low physical demands, that were common among women in the study population. It is also possible that the work participation facilitation was more efficient for women with RP, since they reported a higher access to occupational health care. As shown in Table 4, the large majority of those who changed the main livelihood had retired, and only a few percent had changed into another field of work. This is at least in part explained by the age composition of the study sample, in which a large proportion had reached the general retirement age of 65 years by the time of follow-up. Among subjects with RP who had changed field of work, a distinct transition from outdoor to indoor tasks during the follow-up time could not be discerned. However, this subgroup contained few responding subjects and revealed a large variation regarding new occupations, and these facts limit what conclusions could be drawn.
Importantly, most subjects reported a good work ability, regardless of having RP or not. Neither were there any significant effects on sick leave parameters. In this context, it is important to recall that most subjects reported a mild state of RP, regarding both attack frequency, distribution of paleness, and disease progression over time. Thus, it is reasonable to assume that the condition only had a minor impact on work ability. However, concern has been raised if the WAS sufficiently captures limitations in work ability for conditions that only affect the hands [14], since it only gives a rough measure of the global work ability. A more specific item for measuring hand disability, such as the hand disability index of the Stanford Health Assessment Questionnaire [24], might have revealed larger differences between groups. Also, since the WAS relates the current work ability to the lifetime best, there is a risk that perceived effects on work ability are attenuated among subjects with long-standing conditions, such as RP.
Regarding the effects of other factors on work ability, the present study showed a significant effect of age on the WAS. A previous Swedish study on work ability among vibration-exposed workers subjects, where the prevalence of RP was 30% among men and 50% among women, reported an effect of age and distribution of neurosensory symptoms, but not vascular symptoms [16]. The β coefficient for age ranged from − 0.07 to − 0.09, closely resembling the results in the present study. Our study demonstrated a negative impact of high BMI on the WAS, however in the adjusted analyses only statistically significant among women. A high BMI has also previously been associated to poorer work ability, most likely due to reduced physical capacity, although overweight could also be a proxy marker for other disease [12]. In the present study, high perceived stress negatively affected work ability, with a stronger association among women. This is in line with previous research that has shown associations between stress levels and work ability, as well a greater susceptibility for stress among women [12, 13].
Limitations
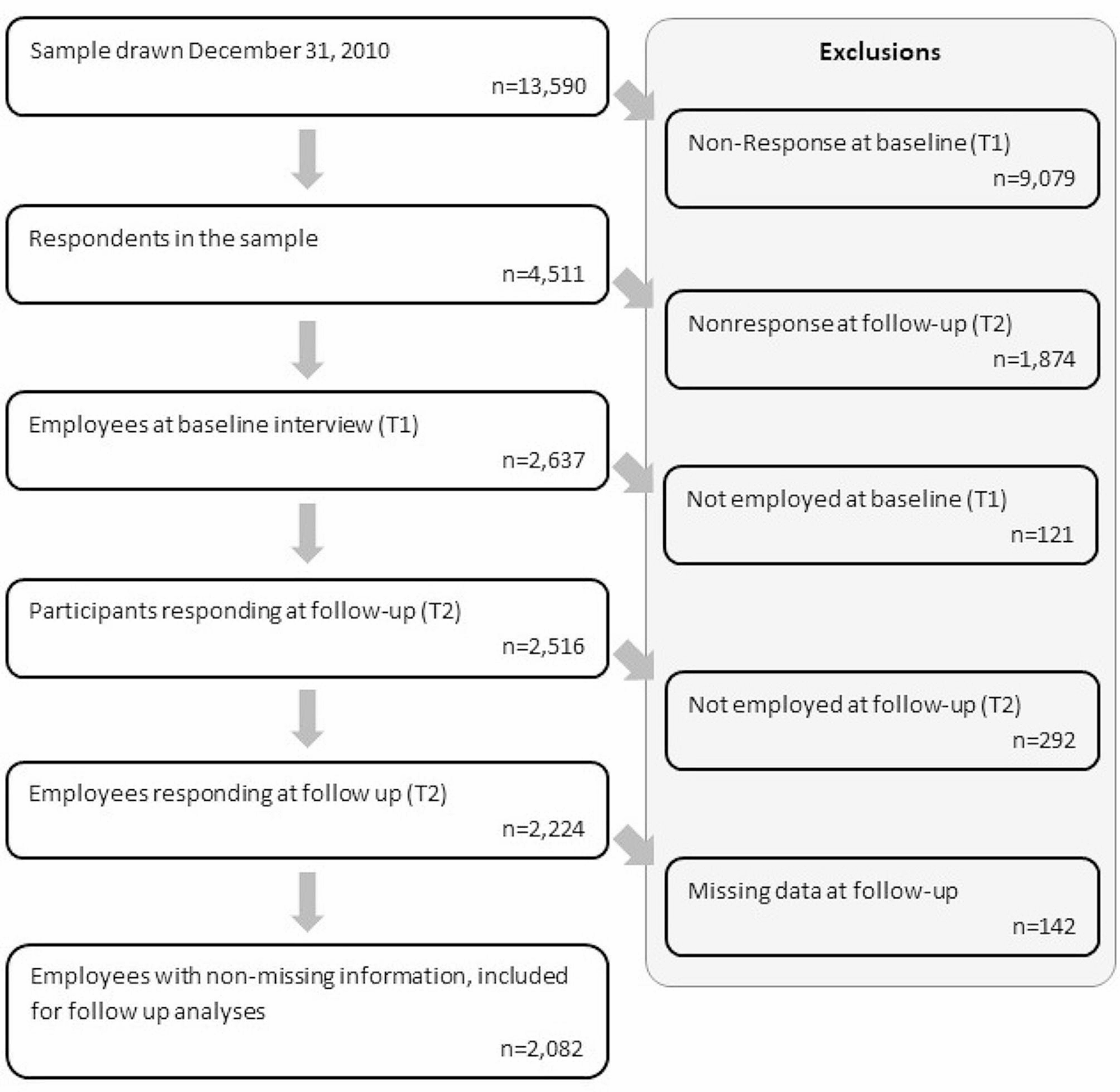
There was a large proportion of survey non-responders, and an underrepresentation of younger age groups among responders (as presented in Additional file 1) that could have affected the generalizability of the results and introduced a sampling bias. Although socioeconomic status may affect work ability, the present study collected no data on such parameters, other than occupational title. The validity of the diagnosis of RP can be questioned, since it was based on a single questionnaire item, although supported by a previously developed color chart that has previously been shown to increase both sensitivity and specificity in comparison with only posing questions [19, 25]. Using more specific criteria, or performing a thorough examination by a physician, would likely have increased the diagnostic accuracy. However, such clinical investigation was not feasible due to the large study size. Furthermore, the surveys were not designed to separate between primary and secondary RP, and it is plausible that secondary RP might negatively affect work ability more so than primary RP. Also, the underlying conditions of patients with diseases giving rise to secondary RP could have had a larger impact on work ability than the symptoms of RP in itself. Thus, in future studies on work ability in this context, more attention should be given to the etiology of RP. Finally, the low explained variance proportions of the multiple linear regression models suggest that there are other important factors that affect work ability that were not investigated in our study.
Strengths
To the authors’ knowledge, this is the first population-based prospective study on work ability among subjects with RP. The study was performed in a Scandinavian setting, where the condition is quite common. The surveys were detailed and enabled longitudinal analyses with six years of follow-up time. Also, both surveys were distributed during the same late-winter season, so that cold exposure, which often serves as a trigger for vasospastic symptoms, would be comparable. Also, since previous studies have reported on differences in RP between women and men [10, 26], all analyses were stratified by gender.





留言 (0)