
記住我



For this literature review, we searched MEDLINE (PubMed) and Embase, while clinicaltrials.gov was searched for ongoing clinical studies. The following search terms included in the title were used: “cardiac work,” “constructive work,” “global longitudinal strain,” “global work index,” “myocardial work,” “myocardial work efficiency,” “non-invasive myocardial work,” in combination with “pressure-strain loops” in the title or abstract. Relevance and credibility of all the sources were considered, and the final decision on inclusion was reached through a consensus of the following screening authors: DA, TR, AF, and AA. Review articles, case reports, comments, and author replies were excluded. The cited references were published within the last 8 years. A narrative synthesis with a tabulation system was used to analyze studies for their diverse research designs, methods, and implications.
Clinical applicationsIn the present review, we focused on the state of the art regarding non-invasive myocardial work assessment in several clinical fields: in CRT recipients, in patients with ischemic cardiac disease, mitral valve repair, heart failure with reduced (HFrEF) and those with heart failure and preserved ejection fraction (HFpEF) or HFpEF-like syndromes (hypertrophic cardiomyopathy, cardiac amyloidosis) (Fig. 5).
Fig. 5
Current scientific articles on myocardial work divided according to different clinical subtopics
Furthermore, we searched for ongoing clinical trials focusing on non-invasive myocardial work assessed by pressure-strain loops.
Cardiac resynchronization therapyCardiac resynchronization therapy (CRT) is an effective therapy that aims to restore mechanical efficiency to the failing LV by resynchronizing the contraction of the left and right ventricle, resulting in a reduction of both morbidity and mortality [39]. According to the 2016 ESC guidelines for the diagnosis and treatment of heart failure, CRT is taken into account with a class I a recommendation in symptomatic patients with heart failure (HF) in sinus rhythm with a QRS duration ≥ 150 ms and left bundle branch block (LBBB) as well as with an LVEF ≤ 35% despite optimal medical therapy (OMT); in patients with HFrEF regardless of their NYHA class who indicate for ventricular pacing and high degree AV block (including patients with atrial fibrillation) [40].
However, the number of patients who do not respond to CRT remains high (30–35%) [41]. Estimating CRT response is difficult as there is a lack of a globally accepted CRT response definition. Mostly, CRT response is identified by a ≥ 10–15% reduction of LV end-systolic volume (LVESV), assessed by echocardiography 6 months after device implantation, as a sign of LV reverse remodeling [42]. Current patient selection criteria utilize the surface 12-lead ECG to identify electromechanical delay; here, the presence of left bundle branch block morphology is considered to be a predictor of response to CRT [39]. However, it is becoming increasingly clear that QRS duration is an inadequate predictor of CRT response, since LV dyssynchrony is not uncommon in patients with a narrow QRS, proving how electrical dyssynchrony does not always correlate to mechanical delay [43]. In such cases, mechanical dyssynchrony may be, in fact, the result of abnormalities in regional contractility of the LV and loading conditions which can be better assessed through further imaging techniques, rather than ECG. However, although some echocardiographic dyssynchrony parameters have proven to be valuable in predicting CRT response in numerous, single-center studies [44, 45], the multi-center PROSPECT trial showed how such predictors are burdened with low sensitivity and specificity [42]. Therefore, as of today, no imaging technique is accepted for the identification of CRT responders, as also pointed out by 2016 ESC heart failure guidelines, which discourage the use of echocardiographic dyssynchrony criteria for the selection of patients [40]. Lastly, some clinical evaluations have also been proposed to detect CRT responders: male sex and ischemic etiology were shown as good predictors to less favorable CRT response [46, 47]. Nonetheless, when they were considered together with baseline LV volumes, they proved to be no longer independent variables [48]. Regarding the use of pressure-strain analysis, Galli et al. could show that GCW and GWW were associated with a positive response to CRT [36, 38]. GCW and GWW at baseline were significantly higher in CRT-responders in comparison to non-responders. After 6 months of follow up, CRT responders presented an increase in GCW and a reduction in GWW associated with LV reverse remodeling. Based on the findings of Russel et al. indicating that pressure strain measurements reflect cardiac metabolism, Galli et al. hypothesized that higher GCW at baseline represents a higher contractile reserve and is therefore able to predict positive CRT response, whereas decreased amount of GCW could be associated with reduced myocardial viability, limiting the beneficial effects of CRT [22, 36, 49, 50]. Furthermore, Ciampi et al. previously showed that the existence of contractile reserve assessed by dobutamine stress echocardiography is associated with a better prognosis, which is independent of the presence of LV dyssynchrony, as LV stimulation recruits viable myocardium [50]. There are several methods for the assessment of myocardial viability available, e.g., stress echocardiography, cardiac magnetic resonance, and nuclear imaging. Non-invasive estimation of myocardial work by pressure-strain analysis could provide a simple, easily accessible and cost-saving additive method. Additionally, Galli et al. confirmed a predictive value of GWW for positive CRT response, postulating that GWW might stand for a recruitable energy waste which could be significantly reduced in positive CRT responders [36]. The combination of GCW > 1057 mm Hg% and GWW > 364 mm Hg% showed very good specificity with low sensitivity [36]. Hence, myocardial work indices can be used to identify CRT responders, but patients might also benefit from CRT if GCW and GWW are below the mentioned cut-off values [36]. However, given the existence of numerous independent mechanisms influencing CRT response, the study suggests that the combination of clinical, electrocardiographic, and echocardiographic data in particular might be more useful to detect CRT responders [50,51,52,53,54,55]. In an earlier study by Vecera et al., also septal wasted work, especially in combination with the wall motion score index (WMSI), strongly predicted CRT response [56]. These results were confirmed in a study by Zhu et al. using a 3D echocardiography and 3D speckle tracking imaging analysis to simultaneously obtain left ventricular global and segmental principal strain and volume. Here, the measurement of baseline septal myocardial WW helped to enable a better patient selection for CRT (the more septal wasted at baseline, the higher probability of response to CRT was achieved) [57]. Also, there are preliminary data indicating that preserved GWE and GCW before CRT are associated with improved long-term outcome [37, 58]. Recently, Duchenne et al. could demonstrate that the acute redistribution of regional myocardial work after CRT device implantation from the lateral to the septal wall appeared to be strongly related to long-term reverse remodeling. Proper patient selection should consider the presence of loading inhomogeneities for a successful resynchronization therapy [59] (Table 2). In a study by Kostyukevich et al., CRT responders had significantly larger septal WW and lateral CW compared to non-responders at baseline. Plus, on multivariate analysis, baseline lateral CW was independently associated with CRT response (CW > 881 mm Hg%) [60]. Moreover, CRT responders demonstrated a significant improvement in septal CW and WW as well as a decrease and an increase in lateral CW and WW respectively [60].
Table 2 Non-invasive myocardial work and cardiac resynchronization therapy (CRT)In conclusion, even though pressure strain loops and related indexes cannot be used on their own to assess CRT candidates, they represent a novel method that shows promising results in the prediction of CRT response and long-term outcomes.
Ischemic heart diseaseIn patients with non-ST-elevation myocardial infarction (NSTEMI), Boe et al. could show that the non-invasively estimated myocardial work index (MWI) was able to detect acute coronary occlusion, being superior to all other echocardiographic parameters used, including strain analysis [33]. Patients with NSTEMI represent a very heterogonous group in which timing of invasive therapy is not well defined [61, 62]. The identification of acute coronary occlusion in patients with NSTEMI could be beneficial in identifying patients who would benefit from direct or early revascularization [33].
In a further study, Edwards et al. validated that non-invasively assessed global myocardial work at rest allowed to detect subclinical coronary artery disease (CAD) in patients with preserved LVEF and no regional wall motion abnormalities (RWMAs) [34]. Interestingly, global myocardial work was even more sensitive in detecting subclinical coronary disease than global longitudinal strain (GLS), also in patients only suffering from a single-vessel disease [34]. GLS has a predominant contribution from the longitudinal arranged endocardial layer and therefore detects early ischemia-induced cardiac dysfunction since the subendocardium is more sensitive for reduced perfusion [63,64,65,66,67,68,69,70]. Other echocardiographic parameters that represent radial thickening as LVEF or RWMAs are less sensitive for the early derangement of myocardial function caused by ischemia [71, 72]. Here, global myocardial work performed even better than GLS underlining the sensitivity of myocardial work for myocardial oxygen consumption which seems to be reduced in early stages of CAD where LVEF is still preserved, and RWMAs are still absent [34].
In a retrospective analysis by El Mahdiui et al., a reduced myocardial work efficiency could be confirmed in patients with recently revascularized ST-elevation myocardial infarction and patients with heart failure with reduced ejection fraction [73]. However, there was no alteration of myocardial work efficiency in patients with no structural heart disease or patients presenting typical cardiovascular risk factors in comparison to healthy individuals [73] (Table 3).
Table 3 Ischemic heart disease and further applications of non-invasive myocardial workChronic heart failureAccording to the current ESC Heart Failure Guidelines from 2016, heart failure represents a clinical diagnosis, which is characterized by typical symptoms and signs as well as increases of natriuretic peptide (BNP or NT-proBNP) [40].
Furthermore, echocardiographic determination of left ventricular function is necessary for the diagnosis of heart failure. Currently, left ventricular ejection fraction (LVEF) and also the assessment of left ventricular filling pressure by using the ratio of early transmitral flow and myocardial relaxation (E/e′ ratio) are the recommended parameters of choice [40].
The prognostic accuracy of LVEF, while significant in the circumstance of an LVEF < 40%, appears to be low in the case of HFpEF [74]. Additionally, LVEF is known to be significantly load dependent.
Today, myocardial strain measurements are well implemented in the daily clinical routine offering more precise, reproducible, and comprehensive information regarding LV mechanics and function. Clinical implications of myocardial strain assessment are diverse.
Notably, global longitudinal strain (GLS) was shown to be associated with outcome in symptomatic heart failure patients with reduced and preserved LVEF, and furthermore a stronger predictor of outcome than LVEF, especially in patients with preserved LVEF [75,76,77,78].
However, like LVEF, strain parameters prove to be dependent on afterload, resulting in a possible misinterpretation of the true contractile function [33, 79].
The estimation of myocardial work fixes this weakness by implementing the estimated LV pressure as described earlier.
In the setting of HFrEF, Wang et al. could show that global myocardial work (GMW) was a better prognosticator than both GLS and LVEF, where reduced values of GMW are significantly associated with death or poor outcome [80].
In a group of patients with acute myocardial infarction and heart failure with preserved or mid-range ejection fraction, it was shown that both GLS and Global Myocardial Work Index (GWI) are reduced in the majority of individuals. Some patients presented normal GWI despite abnormal GLS, emphasizing the importance of implementing blood pressure in the assessment of myocardial function [81].
Moreover, global constructive work (GCW) has been proven to be a better estimate of LV contractile response to physical effort, and hence a better measure of exercise capacity, in HFpEF than GLS. Its exertional increase in patients treated for 6 months with spironolactone is considered to be associated with improvement in functional capacity [82].
Heart failure patients with reduced ejection fraction treated with sacubitril/valsartan showed signs of LV reverse remodeling by common echocardiographic parameters as well as a significant improvement of constructive work and myocardial work efficiency during a follow up of 12 months. Wasted work, on the contrary, did not appear to be greatly affected [83, 84]. Also, GCW could predict long-term outcome in patients with HFrEF receiving sacubitril/valsartan. Not only was a GCW ≤ 910 mmHg at baseline associated with a more advanced disease state, higher values for LV end-diastolic and end-systolic volume and more reduced LVEF but also a significant predictor of major adverse cardiac events (MACEs) before start of therapy [83]. Figure 6 demonstrates how changes in pressure-strain curves according to the LVEF range can be easily derived through the non-invasive assessment of MW by STE.
Fig. 6
Measurement of myocardial work indices by 2D echocardiography; representative pressure strain–loops, bull’s eye plots of myocardial work index, and bar graphs showing GCW and GWW in control subjects (A) and subjects with HFmrEF (B), HFpEF (C), and HFrEF (D). GCW global constructive work, GWW global wasted work, HFmrEF heart failure with mid-range ejection fraction, HFpEF heart failure with preserved ejection fraction, HFrEF heart failure with reduced ejection fraction
Hedwig et al. described the relation between global work index (GWI) and known prognostic parameters of echocardiography (GLS and LVEF), cardiopulmonary exercise test (Peak O2 consumption and VE/VCO2 slope), and NT-pro-BNP in patients with heart failure [85]. In particular, a GWI < 500 mmHg% could predict significant left ventricular remodeling, impaired LVEF, low exercise capacity, and high NT-pro-BNP levels, indicating dismal prognosis [85] (Table 3).
Further applications of non-invasive myocardial workRecently, Chan et al. described various patterns of non-invasively assessed myocardial work by pressure-strain analysis in healthy patients and in those suffering from arterial hypertension or dilated cardiomyopathies [86]. Especially patients suffering from arterial hypertension presented exciting results: In comparison to the control group, high systolic blood pressure (> 160 mmHg) led to a significant increase of GWI with no changes in MW efficiency, whereas GLS showed normal results [86]. These results confirm that usual STE-parameters as GLS are not able to reflect the increased cardiac energy demand to counteract increased afterload. Besides, in the cohorts of ischemic and not-ischemic dilated cardiomyopathy, there was a significant reduction of GWI and GWE due to an increase in wasted myocardial work and a reduction of constructive myocardial work [86].
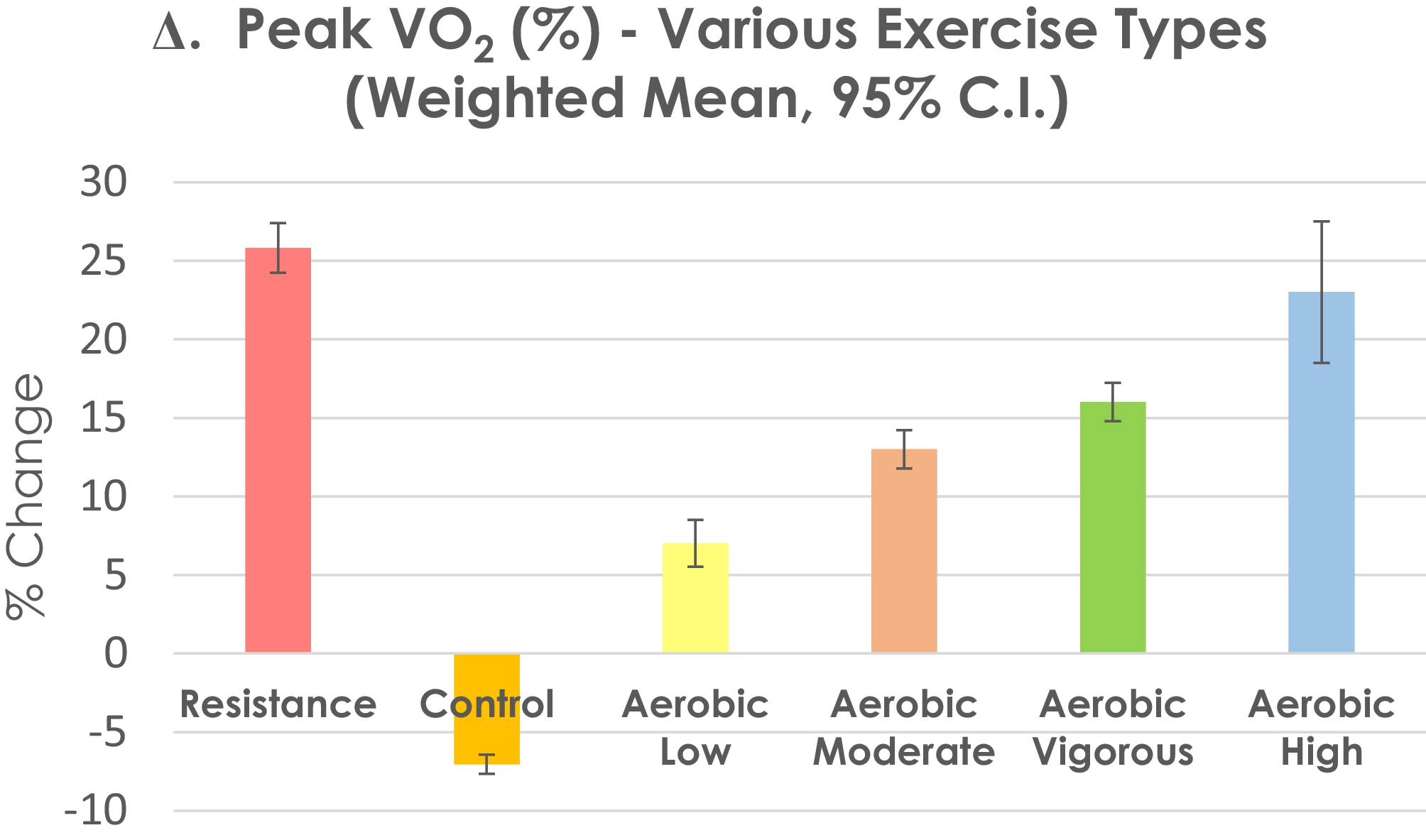
Schrub et al. could also show in patients with dilated cardiomyopathy that the presence of left ventricular dyssynchrony assessed by echocardiography as septal flash or apical rocking leads to a significant reduction to global myocardial work efficiency due to an increase of wasted work [87]. These findings were especially present in the myocardial septum. Furthermore, the septal work efficiency was the only predictor of exercise capacity (VO2 peak) in these patients [87].
Galli et al. were the first to investigate pressure-strain analysis in patients with non-obstructive hypertrophic cardiomyopathy [35]. Here, global constructive work appeared to be significantly impaired in comparison to healthy individuals, despite no significant changes in LVEF [35]. At a multivariable regression analysis, GCW emerged as the main predictor of LV fibrosis assessed by late gadolinium enhancement [
留言 (0)