
記住我


A 4-year-old girl was brought to an ophthalmologist by her parents for evaluation of a new-onset eye abnormality. The patient had also been reporting more frequent headaches with occasional associated emesis. The ophthalmologist noted exophthalmos, and a funduscopic examination revealed papilledema. The patient was sent to the emergency room for imaging and further evaluation. Magnetic resonance imaging of the brain revealed a large, well-circumscribed cystic and solid tumor in the right frontal lobe and basal ganglia region with diffusion restriction and vasogenic edema (Figs. 1A, B). The lesion also contained abnormal metabolic peaks on spectroscopy. The imaging-based differential diagnosis included supratentorial ependymoma, atypical teratoid/rhabdoid tumor, glioblastoma, and pleomorphic xanthoastrocytoma.
 FIGURE 1:
FIGURE 1: Coronal (A) and axial (B) imaging demonstrates a large cystic and solid tumor in the right frontal lobe/basal ganglia region. In both images, a large peritumoral septated cyst is identified with varying protein content. There is peripheral vasogenic edema also present.
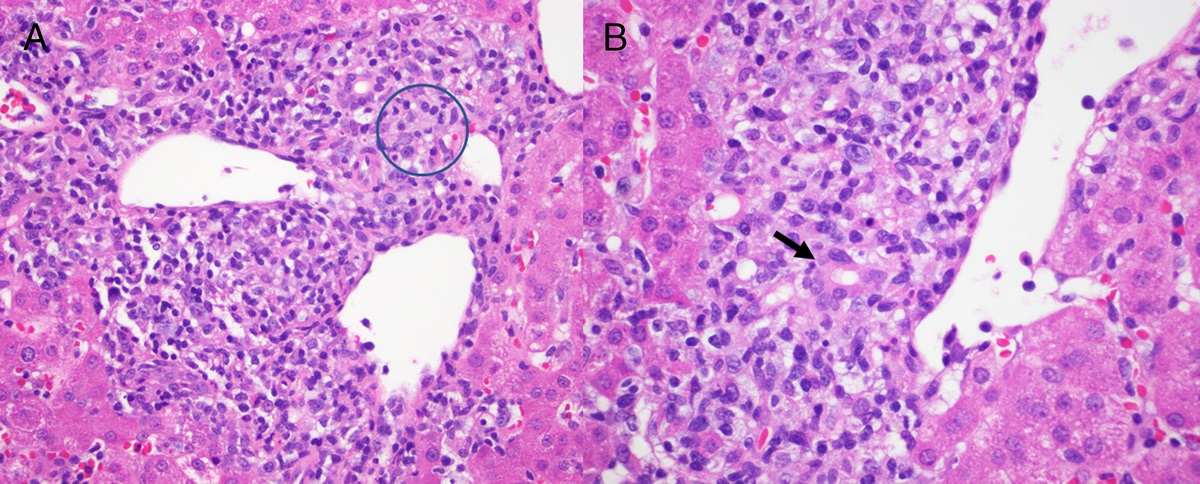
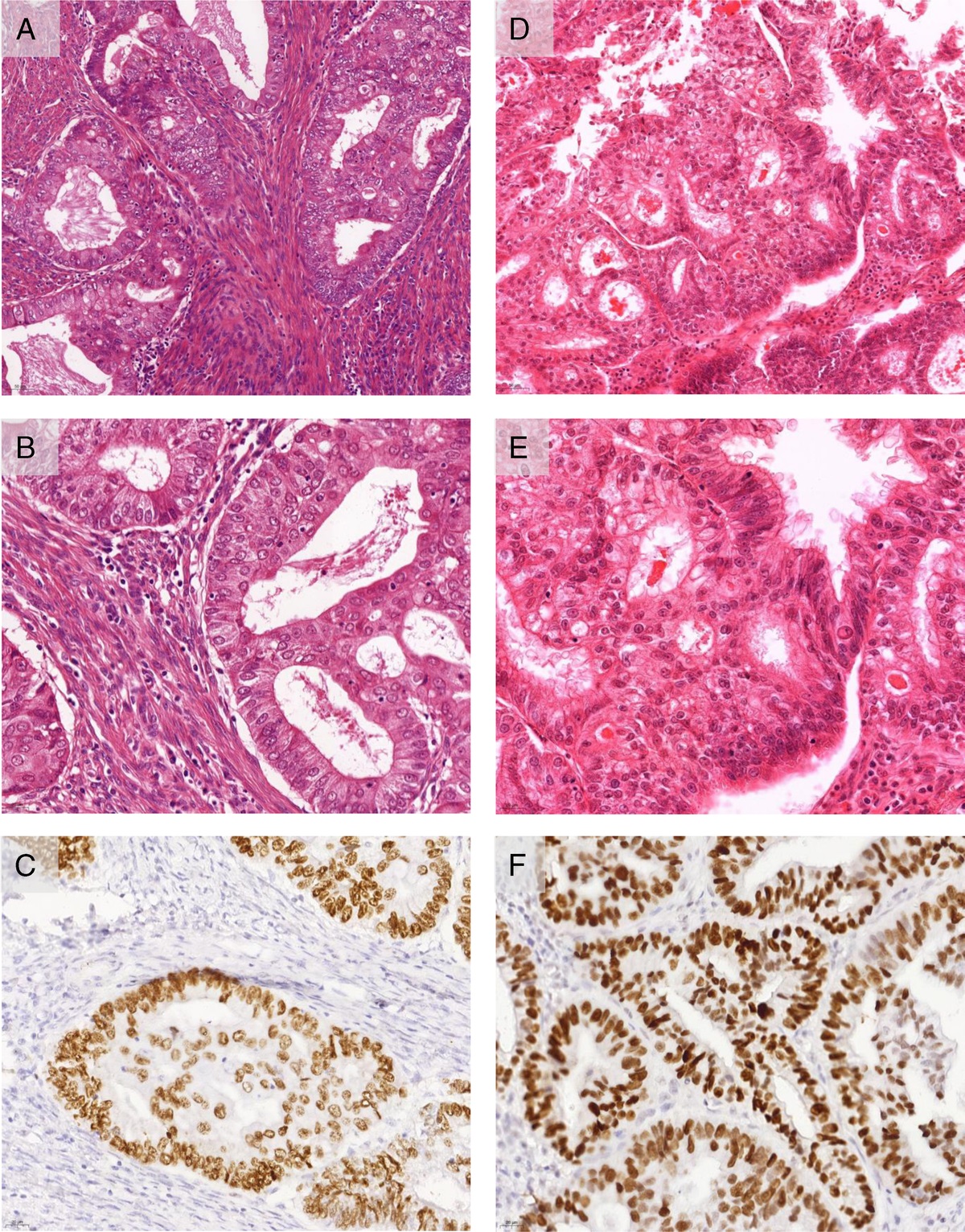
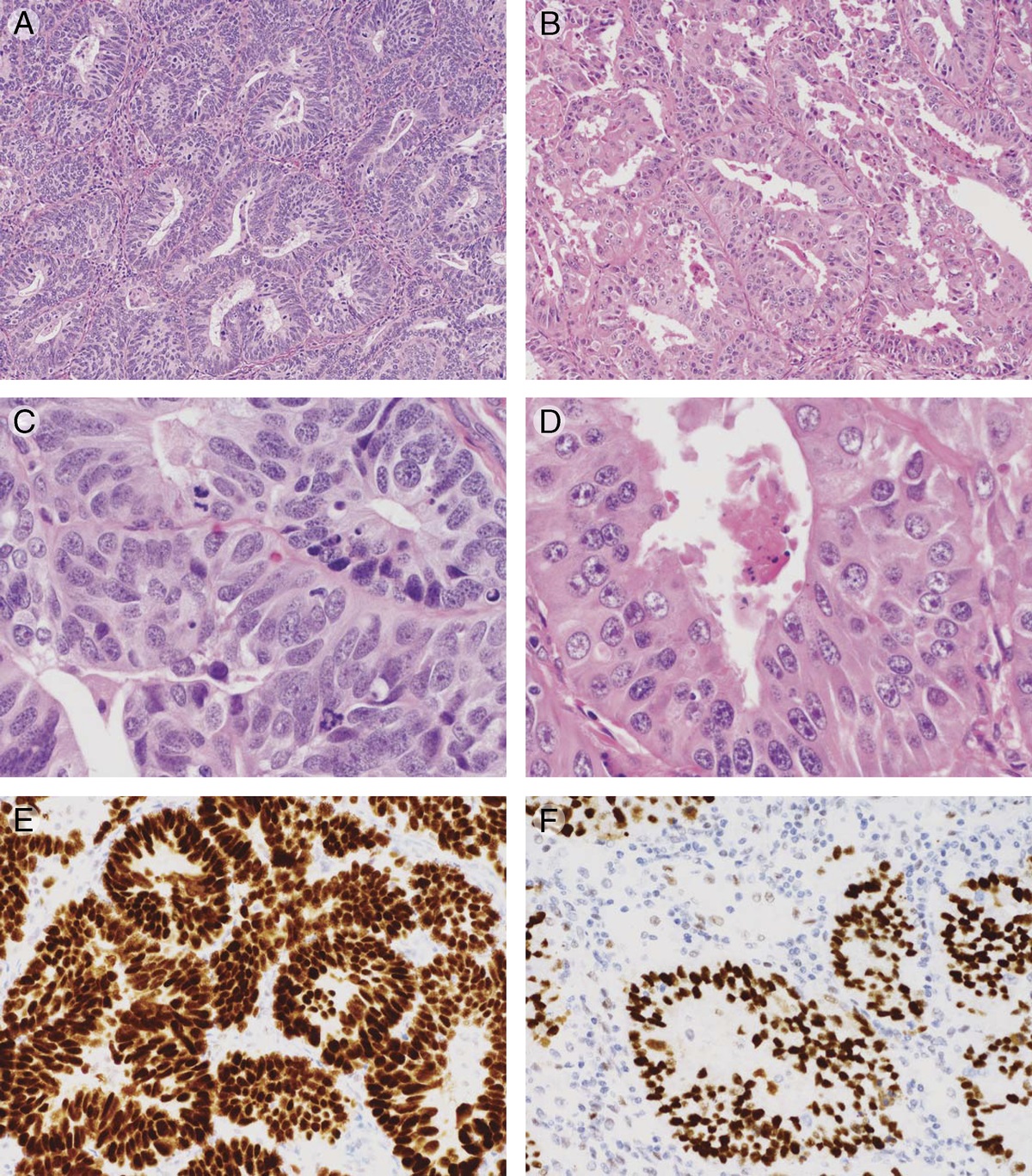
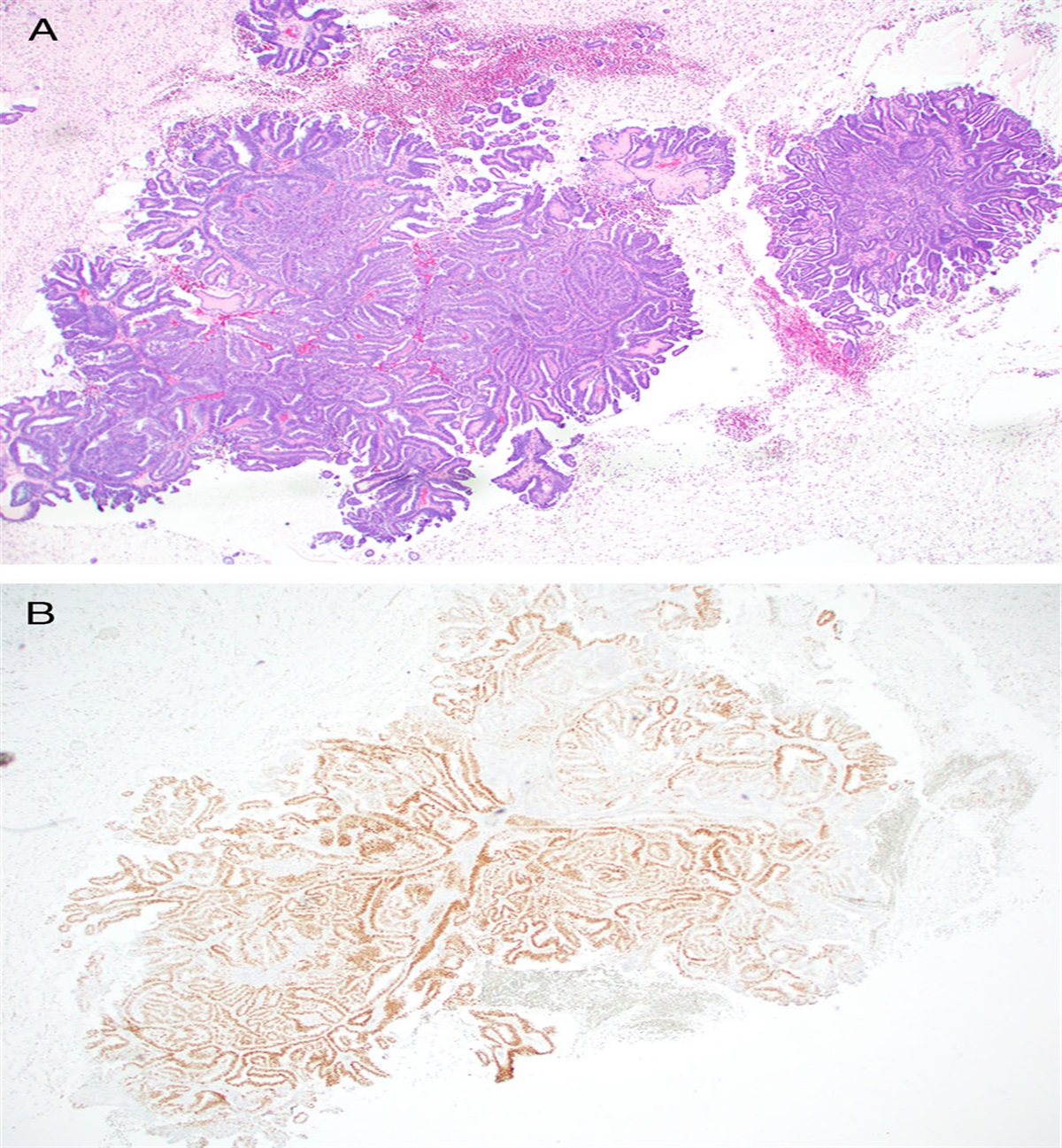
She underwent tumor resection, which revealed tan-pink friable soft tissue with nodularity and a gritty cut surface (Fig. 2A). Hematoxylin-eosin sections of the tumor showed a neuroepithelial tumor with papillary and pseudopapillary architecture with radially arranged perivascular structuring (Fig. 2B). The tumor cells were anchored to centrally positioned blood vessels by their well-defined eosinophilic cytoplasmic processes, resulting in an inverted columnar or cuboidal arrangement of tumor cells (Fig. 2C). Areas of vascular and stromal sclerosis were seen with scattered remnant tumor cell cords (Fig. 2D). Mitotic activity was readily identified, and microvascular proliferation was absent. The differential diagnosis remained broad, including BRAF-mutant epithelioid glioblastoma, ZFTA (C11orf95) fusion-positive ependymoma, central nervous system (CNS) tumor with BCOR internal tandem duplication (ITD), BRAF-mutant pleomorphic xanthoastrocytoma, IDH wild-type glioblastoma, and astroblastoma (AB), MN1-altered. Immunohistochemistry showed that the tumor was positive for OLIG2 and negative for GFAP, had weak perinuclear Golgi expression for synaptophysin, and was strongly and diffusely positive for EMA. There was also nuclear expression of BCOR (Fig. 3). BAF47 and BRG-1 were retained (ie, no INI-1 deletion was present). The Ki-67 was approximately 20%.
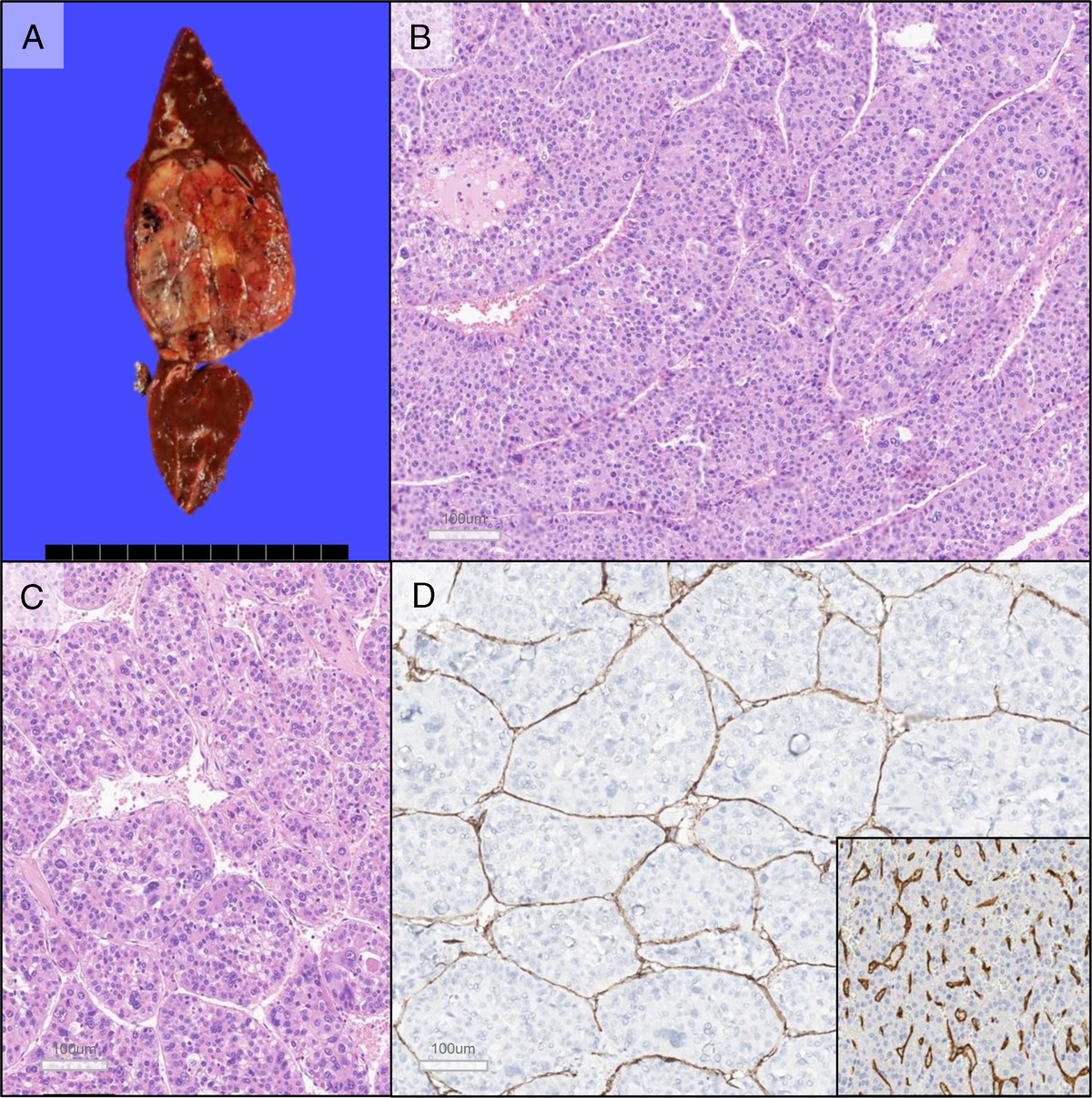
 FIGURE 2:
FIGURE 2: A, Gross examination revealed tan-pink friable soft tissue with nodularity and a gritty cut surface. B, Hematoxylin-eosin sections of the tumor showed a neuroepithelial tumor with papillary and pseudopapillary architecture. C, The tumor cells were anchored to centrally positioned blood vessels by their well-defined eosinophilic cytoplasmic processes. D, Areas of vascular and stromal sclerosis.
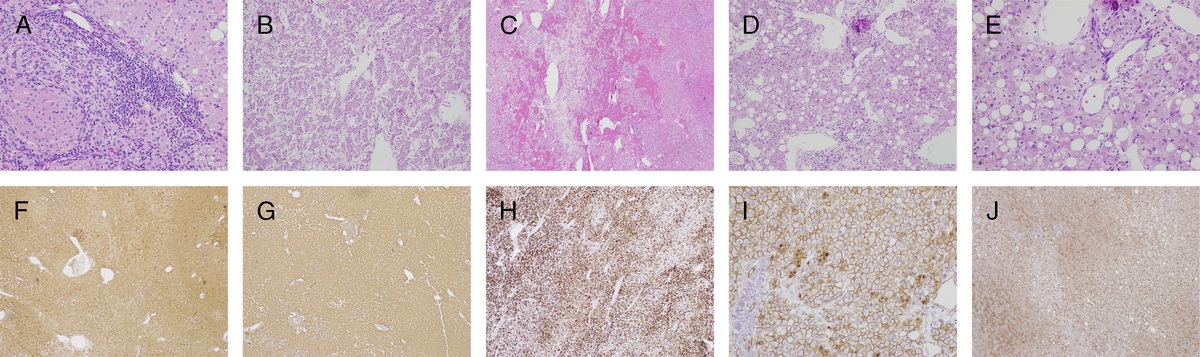
 FIGURE 3:
FIGURE 3: A, Olig2. B, GFAP. C, Synaptophysin. D, EMA. E, BCOR. F, Ki-67.
A preliminary diagnosis of high-grade neuroepithelial tumor was made given the imaging, light microscopy, and immunophenotype, with BCOR ITD as the highest consideration. Next-generation sequencing (NGS) with a fusion panel, including BCOR ITDs, was performed. The tissue was also submitted to Northwestern Memorial Hospital for DNA methylation.
The comprehensive NGS panel failed to reveal any significant molecular abnormalities. No BCOR fusions were present; moreover, BCOR ITDs were absent. The partial loss of Xp and Xq was present (Fig. 4B). DNA methylation pattern classified the tumor as AB, MN1-altered, as shown in the t-SNE (t-distributed stochastic neighbor embedding) plot (Fig. 5). In light of the DNA methylation findings, a second NGS panel (containing multiple MN1 fusion partners) was performed, and the tumor was shown to contain an MN1-BEND2 fusion (Fig. 4A). The tumor was ultimately classified as an AB, MN1-altered.
 FIGURE 4:
FIGURE 4: A, Integrated Genome Viewer (IGV) illustration of the multiple NGS reads aligning to the MN1-BEND2 fusion transcript sequence. According to the sequence detected, the fusion transcript comprised exon 1 of MN1 (chromosome 22q12.1) fused to exon 7 of BEND2 (chromosome Xp22.13) as depicted in schematic on the bottom panel. B, Copy number profile derived from NGS DNA analysis illustrating multiple losses affecting the X chromosome.
 FIGURE 5:
FIGURE 5: t-SNE (t-distributed stochastic neighbor embedding) dimensionality reduction: index case.
DISCUSSIONThe 2021 CNS World Health Organization (WHO) now recommends the use of term AB only when it contains an MN1 alteration.1 However, historically, AB was a diagnosis based solely on light microscopy and immunohistochemistry. Classically, AB is a neuroepithelial tumor with a papillary or pseudopapillary architecture forming pseudorosettes, and with dense sclerosis. When the sclerosis involves the pseudorosette, the term astroblastomatous rosette may be used. While astroblastomatous rosettes can be seen in AB, they are not required for its diagnosis; indeed, astroblastomatous rosettes can be seen in other tumors2 and often invoke a wider differential diagnosis, including pleomorphic xanthoastrocytoma and ZFTA (C11orf95) fusion-positive ependymoma. Previous studies showed that ABs have fairly unique imaging characteristics. These tumors are usually large, peripherally located, and cystic with a bubbly solid component.3 Astroblastomas more commonly occur in females than males.4 Astroblastoma, MN1-altered, also may have variable expression of commonly used immunostains for the workup of neuroepithelial tumors. Immunoreactivity for OLIG2, S-100, and EMA can be variable.5 The current WHO advocates for the utilization of D2-40 (podoplanin) as it has also been expressed in AB, MN1-altered. Other markers used in the immunohistochemical workup of bone and soft tissue tumors (BCOR, SATB2) have also been shown to be positive in AB, MN1-altered.
While it has been recognized that the aforementioned differential diagnoses of tumors with astroblastomatous rosettes have distinct molecular abnormalities, most panels cannot identify every abnormality in the MAPK pathway and contain only a limited number of ZFTA-associated fusion partners. Interestingly enough, there is also another rare neuroepithelial tumor that was considered in the differential diagnosis here, a CNS tumor with BCOR ITD (formerly CNS high-grade neuroepithelial tumor with BCOR ITD). This tumor notoriously has a variable appearance by light microscopy, but a conspicuous feature is the presence of an ependymoma-like perivascular pseudorosette. The largest series of this tumor described in the literature also describes a peculiar sclerosis that may occur in the tumor reminiscent of AB; moreover, Ferris et al6 describe an AB-like neuroepithelial tumor with MN1 alteration that contained strong nuclear BCOR expression. Several round cell sarcomas can also demonstrate the overexpression of BCOR as these sarcomas can be associated with BCOR ITDs and BCOR fusions, commonly BCOR-CCNB3.7 Whereas some reports suggest that the BCOR immunostain displays 100% sensitivity and specificity for tumors with BCOR ITDs,8 this example suggests that that may not be entirely true. There is an underrecognized morphologic and immunophenotypic overlap that can occur in both AB, MN1-altered, and CNS tumor with BCOR ITD.
In this case, comprehensive somatic NGS and fusion panel were utilized to look for both BCOR fusions and BCOR ITDs. MN1 was not present on that panel. Luckily, DNA methylation was also performed simultaneously. If DNA methylation had not been performed, it is likely that an integrated diagnosis would not have been possible. While secondary testing using an in-house panel did identify an MN1-BEND2 fusion, the most common fusion that is present in AB, MN1-altered,5 genomic DNA methylation profiling was a useful upfront screening test.9,10
Lastly, the WHO does not recommend a grade for this tumor.1,11 In the past, these were either considered low or high grade. A narrower subset of histologically diagnosed ABs that contain only an MN1 alteration allows for correlative studies with long-term clinical data, to potentially assign WHO grades in the future.
CONCLUSIONThis case demonstrates the utility of genomic DNA methylation profiling as a key ancillary molecular tool in the workup of brain tumors, either alongside or before NGS. It can not only provide critical information about a tumor's true identity, but also generate invaluable data that will eventually be leveraged in research studies aimed at better understanding tumor biology, prognosis, and potential new therapeutics.
REFERENCES 1. Brat DJ, Solomon DA, Rosenblum MK, et al. Astroblastoma, MN-1 altered. In: WHO Classification of Tumours Editorial Board. Central nervous system tumours (WHO classification of tumours series, 5th ed.; vol. 6). Lyon, France: International Agency for Research on Cancer; 2021. Available at: https://tumourclassification.iarc.who.int/chapters/45. Accessed March 6, 2022. 2. Lehman NL, Usubalieva A, Lin T, et al. Genomic analysis demonstrates that histologically-defined astroblastomas are molecularly heterogeneous and that tumors with MN1 rearrangement exhibit the most favorable prognosis. Acta Neuropathol Commun 2019;7(1):42. 3. Port JD, Brat DJ, Burger PC, et al. Astroblastoma: radiologic-pathologic correlation and distinction from ependymoma. Am J Neuroradiol 2002;23(2):243–247. 4. Brat DJ, Hirose Y, Cohen KJ, et al. Astroblastoma: clinicopathologic features and chromosomal abnormalities defined by comparative genomic hybridization. Brain Pathol 2000;10(3):342–352. 5. Hirose T, Nobusawa S, Sugiyama K, et al. Astroblastoma: a distinct tumor entity characterized by alterations of the X chromosome and MN1 rearrangement. Brain Pathol 2018;28(5):684–694. 6. Ferris SP, Velazquez Vega J, Aboian M, et al. High-grade neuroepithelial tumor with BCOR exon 15 internal tandem duplication—a comprehensive clinical, radiographic, pathologic, and genomic analysis. Brain Pathol 2020;30(1):46–62. 7. Kao YC, Owosho AA, Sung YS, et al. BCOR-CCNB3 fusion positive sarcomas: a clinicopathologic and molecular analysis of 36 cases with comparison to morphologic spectrum and clinical behavior of other round cell sarcomas. Am J Surg Pathol 2018;42(5):604–615. 8. Mardi L, Tauziede-Espariat A, Guillemot D, et al. BCOR immunohistochemistry, but not SATB2 immunohistochemistry, is a sensitive and specific diagnostic biomarker for central nervous system tumours with BCOR internal tandem duplication. Histopathology 2021;79(5):891–894. 9. Capper D, Jones D, Sill M, et al. DNA methylation-based classification of central nervous system tumours. Nature 2018;555(7697):469–474. 10. Sturm D, Orr BA, Toprak UH, et al. New brain tumor entities emerge from molecular classification of CNS-PNETs. Cell 2016;164(5):1060–1072. 11. Tauziède-Espariat A, Pagès M, Roux A, et al. Pediatric methylation class HGNET-MN1: unresolved issues with terminology and grading. Acta Neuropathol Commun 2019;7(1):176.
留言 (0)