
記住我


This randomized controlled trial was registered in the Iranian Registry of Clinical Trials (Trial registration: IRCT, IRCT20090203001640N17. Registered 20 may 2020, https://en.irct.ir/trial/46855). Ethical approval was obtained from the Ethics Committee of Research Institute for Endocrine Sciences of Shahid Beheshti University of Medical Sciences, Tehran, Iran (No. IR.SBMU.ENDOCRINE.REC.1399.001). All participants provided written informed consent forms before recruitment. According to the principles of the Declaration of Helsinki, the study procedures, purpose, and adverse events were explained to each participant (written and orally).
Participants, randomization, and allocation concealmentThis randomized controlled trial was conducted in the framework of Tehran Lipid and Glucose Study (TLGS). The TLGS is a large long-term community-based prospective study being conducted on a representative sample of residents from district No. 13 of Tehran, Iran. The population of this district represents the urban population of Tehran. The details of this study are described elsewhere [29]. Briefly, the first examination was initiated in March 1999. Using multistage stratified cluster random sampling, more than 15,000 individuals, aged ≥ 3 years, were enrolled. Overall, since 1999, the TLGS participants have undergone assessments for sociodemographic factors, lifestyle, medication use, socioeconomic status, anthropometric indices, and medical history of cardiovascular risk factors. The information is documented every three years in face-to-face visits by the local research team to update the previous data. Phases II, III, IV, V, and VI of this study were prospective follow-ups conducted during 2002–2004, 2005–2008, 2008–2011, 2012–2015, and 2016–2018, respectively.
Of 10,927 individuals participating in phase VI of the TLGS study, TCF7L2 rs7903146 genotype was randomly determined in 8399 participants. Of these, 662 participants, aged 30–65 years, had type 2 diabetes with available information on TCF7L2 rs7903146 genotype (CC genotype, n = 240; TT genotype, n = 128, and CT genotype, n = 294). The criteria for diagnosing diabetes included a fasting plasma glucose (FPG) level ≥ 126 mg/dL, two-hour plasma glucose ≥ 200 mg/dL, or using antihyperglycemic medications. Other inclusion criteria were being overweight or obese (BMI: 25–40 kg/m2); no weight changes in the last three months before enrollment; consumption of red meat ≥ 1 serving/d; and willingness to consume legumes in the diet. On the other hand, participants with pregnancy or lactation, cardiac, hepatic, or renal impairment (creatinine ≥ 1.4 mg/dL in men and ≥ 1.3 mg/dL in women), and insulin use were excluded.
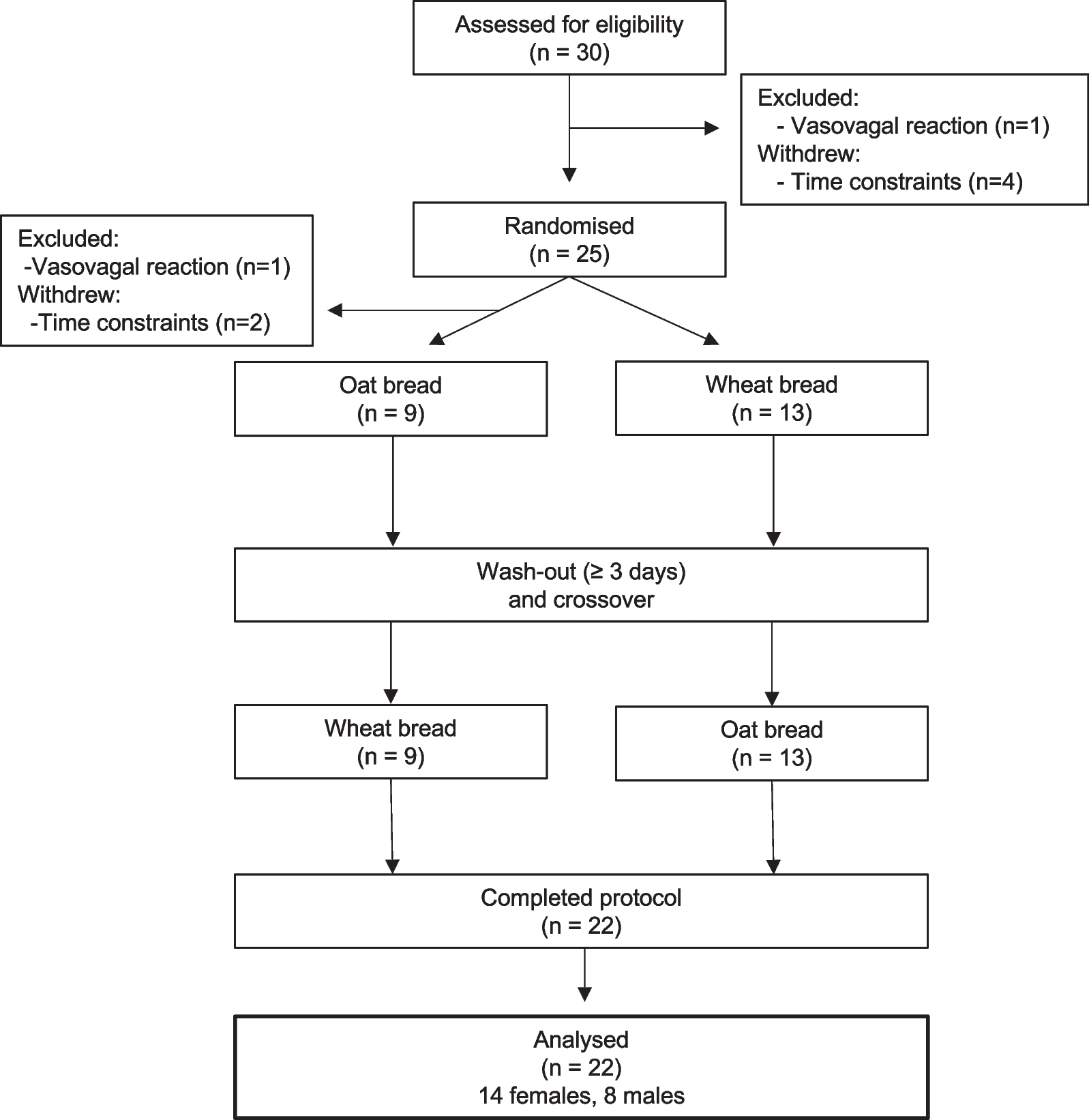
Randomization was carried out to generate the randomization sequence using the randomization website (www.randomization.com). The randomization sequence was separately generated for participants with TCF7L2 rs7903146 risk allele (CT + TT) and non-risk allele (CC). Among participants eligible for this study, we selected 150 participants with genotype CC and 150 participants with genotype TT + CT and assigned them separately and randomly (1:1 ratio) to either the DASH diet group or the legume-based DASH diet group. The recruitment of participants is shown in Fig. 1.
Fig. 1
Flowchart for the participants
The participants were randomly assigned to receive one of the two diets by a member of the TLGS staff. Using sealed and sequentially numbered opaque envelopes, the subject’s allocation to treatment was concealed from all staff members and the principal investigator; they were only opened sequentially by the dietitian in the presence of eligible participants in the first visit.
BlindingIn the nutritional interventions, blinding of the participants was practically impossible. However, the participants were unaware of their assignment to the intervention groups before enrolment. Individuals who assessed the outcomes, including laboratory technicians and staff members, were blind to the participants’ assignment, and dietary interventions were provided by a dietitian.
Dietary interventionsFirst, 307 individuals participated in a two-week run-in period when they consumed their usual diet while eliminating the legume intake. In the run-in period, seven participants were unwilling to continue the study and were excluded. At the end of the run-in period, 300 participants, stratified based on risk and non-risk alleles, were randomly assigned to the DASH diet group or legume-based DASH diet group over 16 weeks.
The participants’ energy requirements were estimated from the resting energy expenditure, based on the Mifflin-St Jeor formula and multiplied by the physical activity coefficient [30]. Because the participants were overweight and obese, 500–700 kcal/d was deducted from their energy requirements. Based on each participant's energy requirement, the dietitian determined the diet, which contained approximately 25–30% fat, 15% protein, and 55–60% carbohydrate. In the DASH diet group, the participants were instructed to follow the DASH diet (2000–3000 kcal based on the participant’s energy requirement), composed of 8–12 servings/day of fruits and vegetables, 7–15 servings of whole grains, 2–3 servings of low-fat dairy products, two servings of red meat, one serving of nuts and seeds, and limited intake of sweets (five servings per week). The legume-based DASH diet was similar to the standard DASH diet, with the exception that one serving of red meat was replaced with one serving of legumes at least five days a week. Also, because legumes are equivalent to one serving of whole grains, one serving of bread was also deducted from the legume-based DASH diet. In both diets, the participants were advised to consume less than or equal to one teaspoon of salt per day (2300 mg/d).
To evaluate the participants’ adherence to the interventions, the dietitian instructed them to record their daily dietary intake using a three-day food record (two weekdays and one weekend day) every weeks. The dietitian called the participants every week to gather their dietary information, compared their information with the instructed diet, and reinforced their diet adherence. The intake of macro- and micronutrients was also calculated using NUTRITIONIST III Version 7.0 (N-Squared Computing, Salem, OR, USA), designed for Iranian foods. All participants were requested to maintain their physical activity and not to change their medications during the 16-week interventions unless prescribed by their physicians.
Primary and secondary outcomesThe primary outcome of this study was the difference in hs-CRP change from baseline to week 16 of follow-up between the groups. The secondary outcome was the difference in IL-6, TNF-α, and MDA changes between the groups. Another secondary outcome was assessment of changes in the inflammatory markers, based on TCF7L2 rs7903146 risk allele (CT + TT) and non-risk allele (CC) separately.
MeasurementsWeight was measured using a digital scale (Seca 707; range: 0–150 kg; Seca GmbH, Germany), with minimal clothing and without shoes; it was recorded to the nearest 100 g. Height was also measured in a standing position, with shoulders in neutral alignment using a stadiometer (Seca 225; Seca GmbH, Germany) without shoes and recorded to the nearest 0.5 cm. The body mass index (BMI) was calculated by dividing weight in kilograms by height in meters squared.
At the beginning of the study and 16-week follow-up (between 7∶00 a.m. and 9∶00 a.m.), venous blood samples were collected from all participants who fasted for 12–14 h overnight. The blood samples were placed in vacutainer tubes, centrifuged within 30–45 min of collection, and stored in a − 80 °C freezer. The serum concentration of hs-CRP was measured using an enzyme-linked immunosorbent assay (ELISA) kit (ZellBio, Germany). To analyze the concentrations of TNF-α and IL-6, ELISA assay was performed using a commercial kit (Diaclone, France). Also, the serum MDA concentration was assessed based on a colorimetric method using a commercial kit (ZellBio GmbH, Ulm, Germany). The intra-assay coefficients of variation (CVs) for the serum hs-CRP, IL-6, TNF-α, and MDA were 2.7%, 8.1%, 6.3%, and 3.3%, respectively.
Genomic DNA was extracted from the buffy coat of samples, using a standard salting out method with proteinase K. The quality of extracted DNA was determined using the NanoDrop 1000 Spectrophotometer. Samples in the range of 1.7 < A260/A280 < 2 were excluded due to low quality and concentration. DNA samples were processed on a HumanOmniExpress-24-v1-0 BeadChip (containing 649,932 SNP loci with an average mean distance of 4 kb) at deCODE Genetics Company (Reykjavik, Iceland), according to the manufacturer’s instructions (Illumina Inc., San Diego, CA, USA). Quality control procedures were also performed using PLINK V. 1.07 and R Statistic V. 3.2 [31].
Assessment of other variablesMedication regimen (e.g., antihypertensive, lipid-lowering, and anti-diabetes drugs and others) and supplement intake were collected. Physical activity was also assessed using the Modifiable Activity Questionnaire (MAQ), and the frequency and amount of time spent per week on physical activity over the last year were recorded.
Statistical analysisThe target sample size was measured to be 150 in each intervention group to detect a difference of 1 mg/dl reduction in hs-CRP [32] between the two diets in the total population by assuming an α error of 0.05, a β error of 0.20, power of 80%, and an attrition rate of 20%.
Through visual inspection of the histograms, scatter plots, and Shapiro–Wilk test, the normal distribution of data was assessed. Normal variables are presented as mean ± SD for demographic variables and mean ± SEM for dietary variables. Skewed variables are also presented as median (interquartile range) and dichotomous variables as count (percentage). Analyses were performed according to the per-protocol and intention-to-treat principles. Multiple imputation by chained equations method was also applied to impute the primary and secondary missing outcomes. In this method, the predictors included all variables presented in Table 1, TCF7L2 rs7903146 variant, and intervention diets.
Table 1 Baseline characteristic of participants according to group of intervention diets and TCF7L2 rs7903146 gene variantDifferences in the changes of outcomes between the two diets in the total population and also with respect to the TCF7L2 rs7903146 risk allele (CT + TT) and non-risk allele (CC) were compared using the analysis of covariance (ANCOVA). Model 1 was adjusted for the baseline values, and model 2 was further adjusted for oral antihyperglycemic Medications. The gene-diet interaction was analyzed by an ANCOVA multivariate interaction model, and P-value < 0.2 indicated the significant effect of gene-diet interaction on the outcomes. The Benjamini–Hochberg correction method for multiple testing yielded critical P-values of < 0.1 for the secondary outcome comparisons. Cohen’s d for effect size (0.20, 0.50, and 0.80 interpreted as small, medium, and large treatment effects, respectively) was also calculated based on mean and SD [33]. All analyses were performed in Stata Version 14.0 (StataCorp LLC, TX, USA).
留言 (0)