In this report, we describe a rare fatal case of disseminated nocardiosis due to N. Otitidiscaviarum resistant to TMP–SMX in a lady with advanced cancer.
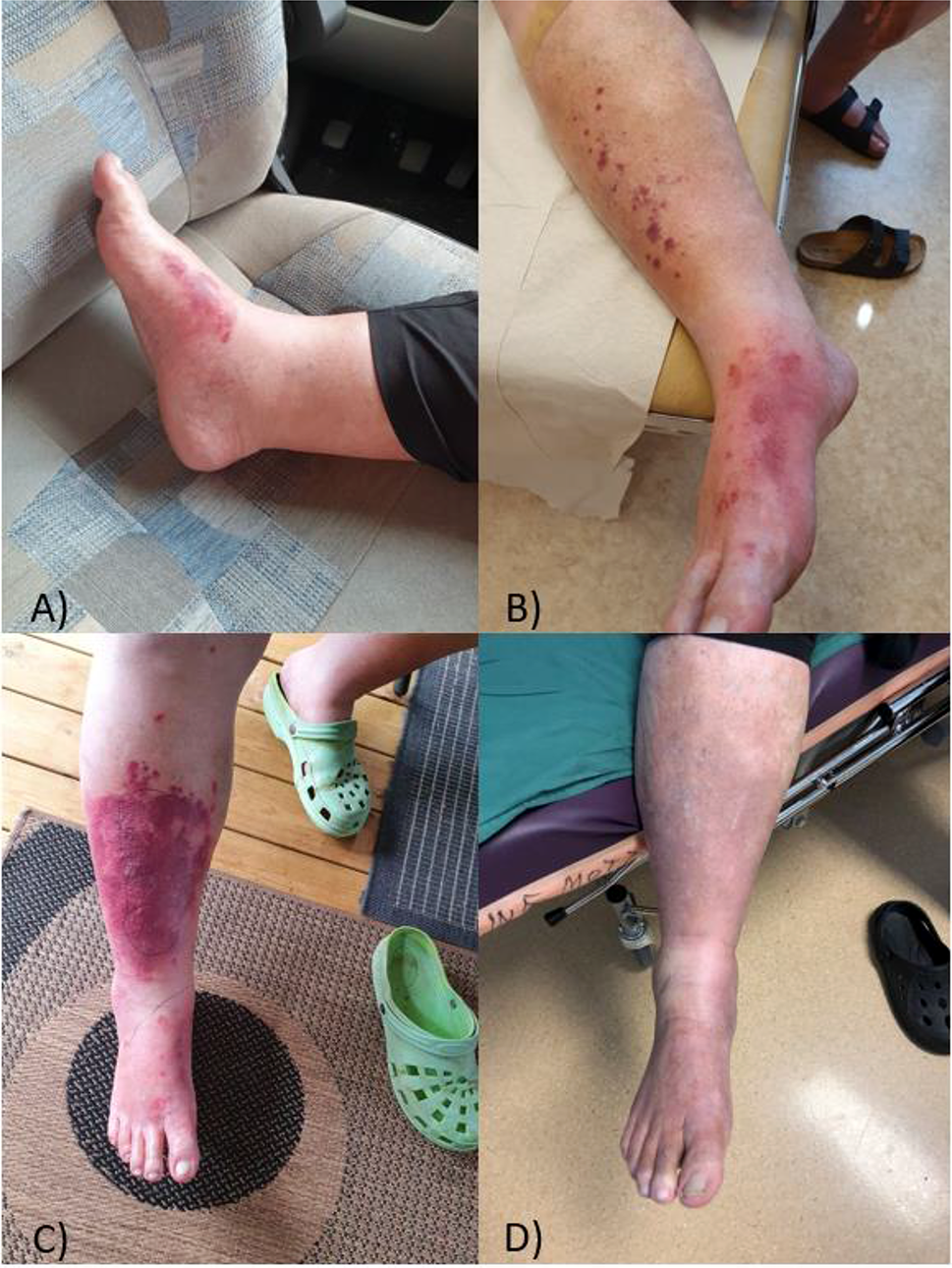
The most common clinical presentation of nocardial disease is pulmonary due to inhalation of mycelial fragments or via contact with the bacteria by a cut or abraded skin which may lead to extrapulmonary dissemination [1]. In our case, the patient’s risk factor was gardening.
N. otitidiscaviarum, formerly called N. caviae, was first reported in humans in the mid-1960s [2]. It was previously reported in 1924 after the organism was isolated from a guinea pigs middle ear [3]. Infections with Nocardia are being increasingly recognized, however, infections due to N. otitidiscaviarum are reported in only 0.3–2.9% of all Nocardia. infections and remains infrequently reported [4]. In one review only 10 cases of 347 patients infected with Nocardia. in the United States were identified as N. otitidiscaviarum [5]. In a Japanese report of more than 303 pathogenic Nocardia isolated from infected patients between 1992 and 2001, only 14 cases were due to N. otitidiscaviarum [6]. More recently, Chen Liu et al. described a fatal case of severe pneumonia due to N. otitidiscaviarum in an immunocompetent cotton farmer [7], while Ranjit Sah et al. reported successful treatment of a patient under steroid therapy with disseminated N. otitidiscaviarum [8]. Moreover, it was reported to cause disease in both immunocompetent and immunocompromised hosts in the forms of pulmonary, cutaneous, central nervous system and lymphocutaneous infections [4].
In nature, N otitidiscaviarum is found in soil, decomposing vegetation, and other organic matter, as well as in fresh and saltwater [9]. A survey of 504 soil samples in India revealed that N. otitidiscaviarum had a much lower prevalence compared to other Nocardia which may indicate the reason for its low incidence in clinical practice [10]. In addition, it was noted to be less pathogenic in humans when compared to other Nocardia.
Being described as an opportunistic pathogen, individuals with weakened immune system, such as patients suffering from diabetes mellitus, chronic obstructive pulmonary disease, mixed connective tissue disorder, ulcerative colitis, cirrhosis, human immunodeficiency virus (HIV) infection, malignancies, those receiving long-term or large doses of corticosteroid therapy, and stem cell or solid organ transplant recipients are at higher risk for infections due to N. otitidiscaviarum [11], similarly, our case had stage 4 invasive ductal carcinoma of the breast and was on chemotherapy for eight weeks with the last dose given three weeks before her presentation.
In a review of the database for N. otitidiscaviarum, 25 cases had been reported between 1997 and 2018 [7, 12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30]. More than half of those cases were reported in immunocompromised patients. Prolonged use of corticosteroids was a major risk factor in the majority [12, 13, 16, 20, 21, 23, 30, 31]. In other cases, organ transplant recipients [32], endocrine disorders [26], HIV and rheumatic heart disease were identified as risk factors [18, 20, 25]. On the other spectrum, eight cases were reported in immunocompetent patients. Four of those were engaged in gardening or farming and were exposed to dust inhalation similarly to our patient [7, 15, 19, 22]. Only one case reported no underlying immunocompromised state nor any occupational risk factors like farming [13].
It may be challenging to diagnose such patients who present with many possible differential diagnoses. Conventional evaluation of specimens including wound drainage, skin and brain lesions biopsies, CSF analysis and cultures along with imaging studies, all remain the principal diagnostic methods. In the present report, the species was determined using MALDI-TOF MS. Although the gold standard for Nocardia species identification is molecular biology with amplification and sequencing of one or two gene(s) among rrs (i.e. the gene coding for 16 S rRNA), hsp65, secA1 and sodA, MALDI-TOF MS is increasingly being used for identifying Nocardia species. MALDI-TOF MS adequately identifies frequent species in 95–100% of cases, however for cases of a low identification score molecular biology-based identification remains important [33]. The isolate in the current study had a 99.9% confidence value, hence no molecular sequencing was performed.
Most N. otitidiscaviarum isolates are reported to be resistant to beta-lactams while usually being susceptible to Amikacin, Fluoroquinolones [12, 34], and trimethoprim–sulfamethoxazole, hence, Sulfonamides remain the standard agents for treatment [12]. Meanwhile, some studies reported N. otitidiscaviarum susceptibility to Linezolid in-vitro; however, data from in-vivo studies are still lacking and the risk of haematological toxicity with prolonged Linezolid therapy is high, hindering its clinical use [35, 36]. A study that assessed 552 clinical isolates of Nocardia from six major laboratories in the USA, found sulfonamide resistance to be only 2%, which is lower than previously shown [37, 38]. The authors hypothesized that these discrepancies may be associated with difficulty in the laboratory interpretation of in vitro MICs for TMP-SMX and SMX and the lack of quality controls for Nocardia for these agents [39]. The isolate in the current study showed MIC of ≥ 8/152 for TMP/SMX respectively, which indicates it to be a realistic phenomenon. However, Imipenem resistance has been more commonly described [34]. Typical in-vitro antimicrobial susceptibility patterns of various Nocardia species indicates that N. otitidiscaviarum is usually susceptible to TMP–SMX (Table 3).
Table 3 Typical in-vitro antimicrobial susceptibility patterns of various Nocardia species (Adapted from Manual of clinical microbiology [40])
Table 4 Case studies of N. otitidiscaviarum resistant to TMP-SMX
Similarly, in our case combined drug therapy with Imipenem and TMP-SMX were used for a total of 22 days until the susceptibility result showed resistance to both agents and treatment with Linezolid, Ceftriaxone, moxifloxacin, doxycycline was used in addition to Amikacin that was added earlier due to the appearance of new skin lesions. The delay in obtaining susceptibility results from the outside lab clearly had a negative impact on patient outcome, such cases would advocate for wider availability of such testing and higher turnaround time.
Mortality due to disseminated Nocardiosis is high, therefore early diagnosis and initiation of therapy are of vital importance in Nocardial infections. In our case, the patient was started on empirical treatment for Nocardiosis that was later adjusted according to the susceptibility results, however, the delay in administering proper antimicrobials and her pre-existing advanced malignancy may have attributed to her mortality.
In conclusion, N. otitidiscaviarum infection though rare may have considerable mortality; early diagnosis and susceptibility testing are crucial in avoiding similar devastating outcomes. In addition, surveillance for emerging TMP-SMX resistance should be closely monitored.

留言 (0)