
記住我
Participants were recruited through the multicenter RNHS to provide suitable longitudinal information that could serve as the foundation for conducting translational research including clinical trials. Assessments were conducted every 6 to 24 months by clinicians at one of eight sites in the USA from 2006 to 2015 (first iteration) and at 1 of 14 sites from 2015 to 2019 (second iteration). Data from 1380 females with RTT (718 in the first iteration only, 310 in the second iteration only, and 352 in both iterations) were included (Fig. 1). Medication log data from the first iteration were compared with parental report of anxiety-like behavior from the second iteration. Participants from both iterations allowed confirmation of parental report accuracy. Only baseline measures from each iteration were analyzed for this report. All female participants with a diagnosis of RTT (typical and atypical), regardless of MECP2 pathogenic variant status, were considered for inclusion in the analyses presented here. For this analysis, data were excluded from males, participants with a non-RTT diagnosis, and participants missing significant baseline data. The RNHS consortium is part of the Rare Diseases Clinical Research Network (RDCRN), an initiative of the Office of Rare Diseases Research, National Center for Advancing Translational Sciences, National Institutes of Health.
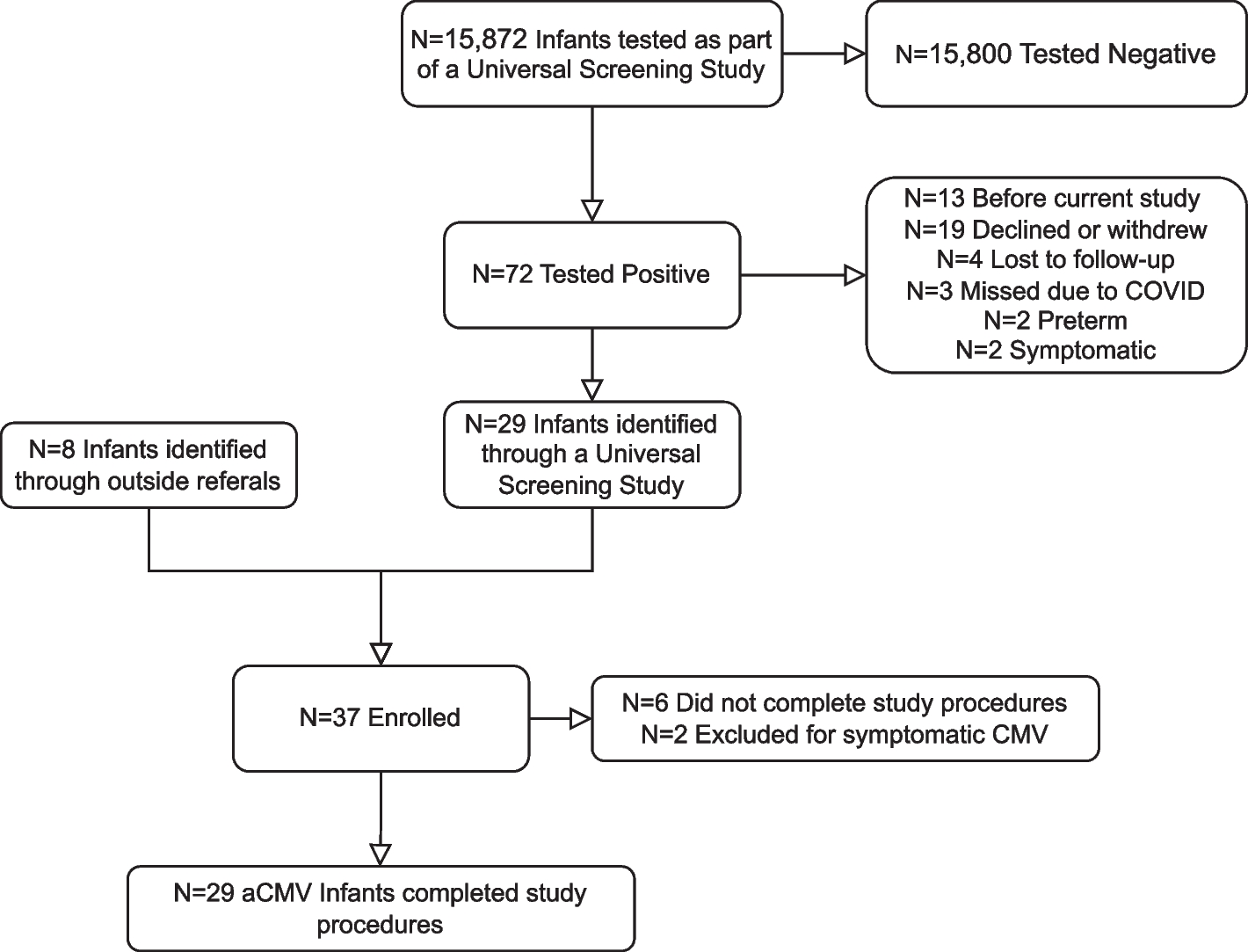
Fig. 1
Rett syndrome natural history study (RNHS) participants selected for analysis (n = 1380). Both = subjects participating in both the first and second iterations; cohort 1 = subjects only participating in the first iteration; cohort 2 = subjects only participating in the second iteration
Human studies approvalParental consent for study conduct and publication of results was obtained prior to entry into the study for all participants. Each participating institution retained institutional review board approval for the implementation of this study protocol and consent form (ClinicalTrials.gov identifiers: NCT00299312 and NCT02738281).
DiagnosisDiagnoses of RTT were based on published diagnostic guidelines, whether classic (typical), variant (atypical), or other related phenotypes by a RNHS site Principal Investigator [22].
MECP2 pathogenic variantsMECP2 variants were reported from clinical laboratory testing. We categorized pathogenic variants as severe (R106W, R168X, R255X, R270X, early truncations, large deletions, and splice site), moderate (T158M and other point mutations), or mild (R133C, R294X, R306C, and C-terminal truncations) based on prior reports of genotype-phenotype correlations [4, 11, 23, 29]. Participants with clinical RTT without a MECP2 variant or with variants in exon 1 were excluded from analyses involving MECP2 severity.
MeasuresClinical severity scale (CSS)The CSS is a clinician-completed questionnaire that uses a Likert-type scale to measure clinical features common in RTT, including age at onset of regression, somatic and head growth status, motor, communication, and RTT behaviors/other neurologic symptoms. Each item is ranked from either 0–4 or 0–5, with higher scores indicating greater clinical severity (range 1–58).
Motor behavioral assessment (MBA)The MBA is a clinician-completed questionnaire for RTT that uses a Likert-type scale to score multiple items based on severity from 0 to 4, with a maximum total score of 148 (first iteration) or 136 (second iteration, with 3 previously low-scoring items removed). The scale includes measures of behavioral/social assessment, orofacial/respiratory assessment, and motor assessment/physical signs. A higher score indicates greater clinical severity.
Anxiolytic and/or SSRI treatmentThe first iteration of the RNHS did not include direct parental assessment of anxiolytics use but the second iteration explicitly asked if the child was prescribed medication for being anxious or nervous. Both iterations of the RNHS collected comprehensive data regarding developmental and medical history, including medication use and indication. Medication logs from both iterations were reviewed for the indication of “anxiety” entered as either free text or as a SNOMED code, regardless of the type of medication associated with that entry. Medication logs were also reviewed for reported use of any SSRI, regardless of the indication associated with that entry.
Anxious behaviorThe first iteration of the RNHS did not include specific questions about anxious behavior but the second iteration explicitly asked how frequently the child was anxious or nervous (with results on a scale of 0–4), whether the child was medicated for being anxious or nervous and, if yes, was the behavior well or poorly controlled. Parents were also asked to choose from a list of common features of RTT and select the top 3 features that have had the greatest impact on their child’s quality of life in the past 6 months.
Analytical strategyData from the second iteration of the RNHS constituted the primary source for the analyses, which included frequency of anxious/nervous and other abnormal behaviors, frequency and effectiveness of treatment for anxiety, drug type used to treat anxiety in RTT, and clinical characteristics of participants. Data from the first iteration of the RNHS were used as a potential source of convergent evidence for profiles of individuals with RTT treated pharmacologically for anxiety. Comparisons of direct report and medication logs for overlapping and non-overlapping subgroups of the second iteration were employed to assess comparability of first and second iteration datasets and accuracy of parental report of anxiety-like behavior.
Statistical analysesDescriptive statistics were used for characterizing most parameters, with continuous variables described in terms of means, standard deviations (SD), and ranges and categorical variables mainly as frequencies. Groups’ age and clinical severity, based on CSS or MBA total scores, were compared using the Mann-Whitney U or Kruskal-Wallis tests. Parent-reported frequency of anxious behavior in different groups was compared by Chi-square test or Fisher’s exact test. Frequency of other parameters and categorical variables, such as race, ethnicity, RTT diagnosis, MECP2 severity, parental report of anxiolytic use, medication log report of anxiolytic use, and medication log report of SSRI use, were also analyzed by these tests. Two-sided P values less than 0.05 were considered significant; Bonferroni adjustments for multiple comparisons were used for analyses where appropriate. The analyses were performed using SPSS version 24.
Characteristics of the study populationFigure 1 displays the number of participants across the years of the first (2006–2015) and second (2015–2019) iterations of the RNHS, including the number of individuals unique to each study and those participating in both iterations. Table 1 displays the clinical features of the participants. Race and ethnicity differ between the study iterations, though most participants (> 85%) are White and non-Hispanic. Participants in the second iteration of the RNHS were older than the first iteration and displayed higher clinical severity scores, as expected from earlier studies. Older age was expected in the second iteration given the overlap of participants. Unexpectedly, when overlapping participants were removed from analysis, on average, participants in the second iteration were older than participants in the first iteration but had similar clinical severity. The type of RTT diagnosis (typical or atypical) and MECP2 variant severity did not differ between the first and second iteration.
Table 1 Baseline clinical characteristics of participants from the Rett syndrome natural history study (RNHS) analyzed in this study
留言 (0)