
記住我
Overactive bladder syndrome (OAB) is a common clinical diagnosis that affects 7–27% of men and 9–43% of women worldwide.1–8 One of the most burdensome symptoms of OAB, urgency urinary incontinence (UUI), exerts a significant negative impact on quality of life for millions of Americans.9 Despite availability of first-line behavioral modifications and second-line medications, many patients are still undertreated. Third-line treatment options are underpenetrated as well because patients rarely progress to these therapies or have poor retention rates.10
The eCoin® (Valencia Technologies Corp., Valencia, CA) is an investigational, fully implanted, neuromodulation device indicated for the treatment of OAB with refractory UUI. It is intended to treat UUI by electrically stimulating the tibial nerve, which is presumed to improve or restore normal control of an imbalanced voiding reflex by retrograde stimulation of the lumbosacral nerves (L4-S3).11,12
The eCoin device is implanted during a short, minimally invasive office or outpatient procedure under local anesthesia. After device activation, subsequent stimulation is automatic and, therefore, does not require multiple office visits or externally applied apparatus. The eCoin is a leadless, coin-sized, and shaped device powered by an internal battery. To maintain the advantages of this design, the device must be replaced upon battery depletion. Potential improvement of the battery longevity would require a bulkier device. A rechargeable power source would require patient intervention, for which adherence might be an issue. Hence, replacement of the eCoin is critical to maintain continuous therapy, and the procedure must be simple and effective such that it can be repeated with each battery depletion. If this reimplantation can be completed safely and with sustained efficacy, eCoin therapy potentially provides a long-term treatment option, in competition with third-line therapies, such as sacral neuromodulation (SNM).
This follow-on study evaluates the feasibility, safety, and efficacy of the reimplantation of eCoin for the treatment of patients with refractory UUI. Replacement of the pulse generator for SNM is a common procedure when the battery is depleted but it has not been reported in the tibial region. Participants included in this study were previous participants of the eCoin feasibility study.13 In the feasibility study, participants were implanted with the first-generation eCoin device, which had an average battery life of approximately 1 year. This follow-on study provided participants the opportunity to be reimplanted with a newer-generation eCoin, which contains a larger battery for greater lifespan.
METHODS Study OverviewThis prospective, single-arm study was conducted at 7 sites in the United States and New Zealand (clinicaltrials.gov: NCT03655054). As a follow-on to the feasibility study (clinicaltrials.gov: NCT03029624), participants had the eCoin-OAB device for at least 1 year before reimplantation. The feasibility study comprised 46 participants, all of which were offered the opportunity to enroll in this follow-on study, regardless of their response to the therapy. Of these 46 individuals, 23 voluntarily enrolled in this follow-on study. The participants of this study were reimplanted with the eCoin OAB-02A, a second-generation device, which differed slightly from the previous device by being 0.8 mm thicker. The eCoin OAB-02A has a larger battery for increased battery life, along with a revised automatic stimulation schedule with more frequent stimulation. The speculated average operating battery life of the eCoin OAB-02A is 2.8 years (compared with 1 year for the first generation in the feasibility study), with a range from 1 to 7 years determined by the inverse relationship between stimulation amplitude and battery life. Participants attended visits for screening, reimplantation, healing check, device activation, and programming. Safety and efficacy assessments were completed at 12 weeks and 24 weeks postactivation, with the primary efficacy analysis at 12 weeks.
This study was conducted in compliance with FDA and International Conference on Harmonization regulations for Good Clinical Practice. Quorum Review approved the protocol and informed consent forms, and regulatory bodies in the United States and New Zealand approved conduct of the study. All participants provided written informed consent.
Study DeviceThe implanted neuromodulation device is a leadless, primary battery-powered, nickel-sized device hermetically enclosed in a titanium case. A conically shaped field of stimulation radiates from a center cathode to an anode outer rim of the 23.3-mm diameter and 3.2-mm-thick device. Materials in direct contact with tissue are the platinum electrodes and the silicone elastomer jacket that covers the titanium housing. The study device differs slightly from the previous generation device that was implanted in the feasibility study. The new device has a slight increase in size of 0.3 mm in diameter and 0.8 mm in thickness. This small enlargement was implemented to incorporate a larger internal battery to improve the longevity of the device.
Patient Screening and Baseline AssessmentsParticipants that were included in the eCoin Feasibility Study for Urgency Urinary Incontinence13 were eligible to participate in this follow-on study. Screening for this follow-on study began after the 1-year follow-up visit from the feasibility study. Regardless of treatment response from the feasibility study, all 46 participants were eligible to enroll in this follow-on study. The baseline assessment completed before initial device implantation in the feasibility study served as the baseline for the 23 participants of this follow-on study. Participants in this study retained their subject ID numbers from the previous feasibility study.
Device Implantation, Activation, and ProgrammingNo later than 120 days after screening, the newer generation eCoin OAB-02A device was reimplanted in each participant by 1 of the 7 participating urologist or urogynecologist investigators. Each of the 23 reimplantation procedures were done in office. The reimplantation procedure for this follow-on trial was similar to the feasibility study implantation procedure. Physicians explanted the older eCoin located in the participants lower leg, and reimplanted a new eCoin device in a single procedure. Physicians palpated and marked the circular boundary of the feasibility study eCoin device, and then marked a 2.5-cm vertical line where the original incision was made. After generously injecting anesthetic to the incision and eCoin site, physicians incised along this marking down to the fascia. The subcutaneous layers were then separated to allow access to the fibrous capsule formed around the device. Investigators made a horizontal incision along the fibrous capsule to access and extract the previously implanted eCoin using forceps. Once the older eCoin was extracted, the new device was inserted and placed in the same fibrous capsule that the previous device was situated. The marginal increase in size of less than 1 mm for the replaced eCoin was negligible when inserted into the fibrous capsule, thus there were no complications with insertion. The incision was then closed in multiple layers using absorbable sutures and dressed.
Participants were provided with wound-care instructions directing them to wear a provided compression sock, and to limit exercise to light activities. The wound was kept dry for at least 72 hours. Participants were instructed to resume daily walking activities.
Participants were not required to wash off or stay off of pharmacological medications for overactive bladder during this study. If participants took pharmacological medications for OAB, this information was recorded.
An incision-site healing check visit was completed 2 weeks postreimplantation. Four weeks postimplantation, a trained field clinical engineer (FCE) conducted the activation visit. During this visit, the FCE activated and set the eCoin stimulation to an amplitude (0.5 to 15 mA) at or below sensory level, which was not uncomfortable for the participant. Participants provided feedback to the FCE about the sensation, most indicating feeling it in the foot, heel, and toes, suggesting stimulation of the tibial nerve. Once activated, electrical stimulation to the tibial nerve is automatically provided in 30-minute stimulation sessions every 3 days for 18 weeks and every 4 days thereafter. The stimulation amplitude could be adjusted by the FCE at follow-up visits.
Follow-UpFollow-up visits occurred at 12 weeks and 24 weeks after activation. During these visits, assessments included review of the 3-day voiding diary, adverse events (AEs), concomitant medication, the Incontinence Quality of Life Questionnaire (I-QOL), and Patient Global Impression of Improvement (PGI-I) survey (a 7-point Likert scale from 1 (very much worse) to 7 (very much better)).14
Statistical Analysis and OutcomesData were analyzed with R, version 3.2 (https://www.r-project.org/). Outcomes for this study contain descriptive statistics, using frequencies and proportions for categorical variables, mean ± standard deviation for continuous data following the normal distribution, and median and range for nonnormal continuous data. The P values for absolute and percent change from baseline comparisons were computed using the nonparametric Wilcoxon signed rank test because most of the outcomes did not follow a normal distribution.
The primary effectiveness outcome was measured by the number of participants achieving at least 50% reduction from baseline in the number of UUI episodes per 24 hours on a 3-day voiding diary after 12 weeks of therapy. The secondary effectiveness outcome was measured by the number of participants achieving at least a 50% reduction from baseline in the number of UUI episodes per 24 hours on a 3-day voiding diary after 24 weeks of therapy. A 95% Clopper Pearson confidence interval was to be summarized for the primary and secondary effectiveness endpoints. The primary and secondary safety endpoints were device related events 16 weeks and 28 weeks after reimplantation respectively. Adverse events were graded by the study centers as mild, moderate, or severe; serious or not serious; classified as related or unrelated; and classified as causing or not causing study termination. The data safety monitoring board reviewed all AEs, including making a confirmation of relatedness.
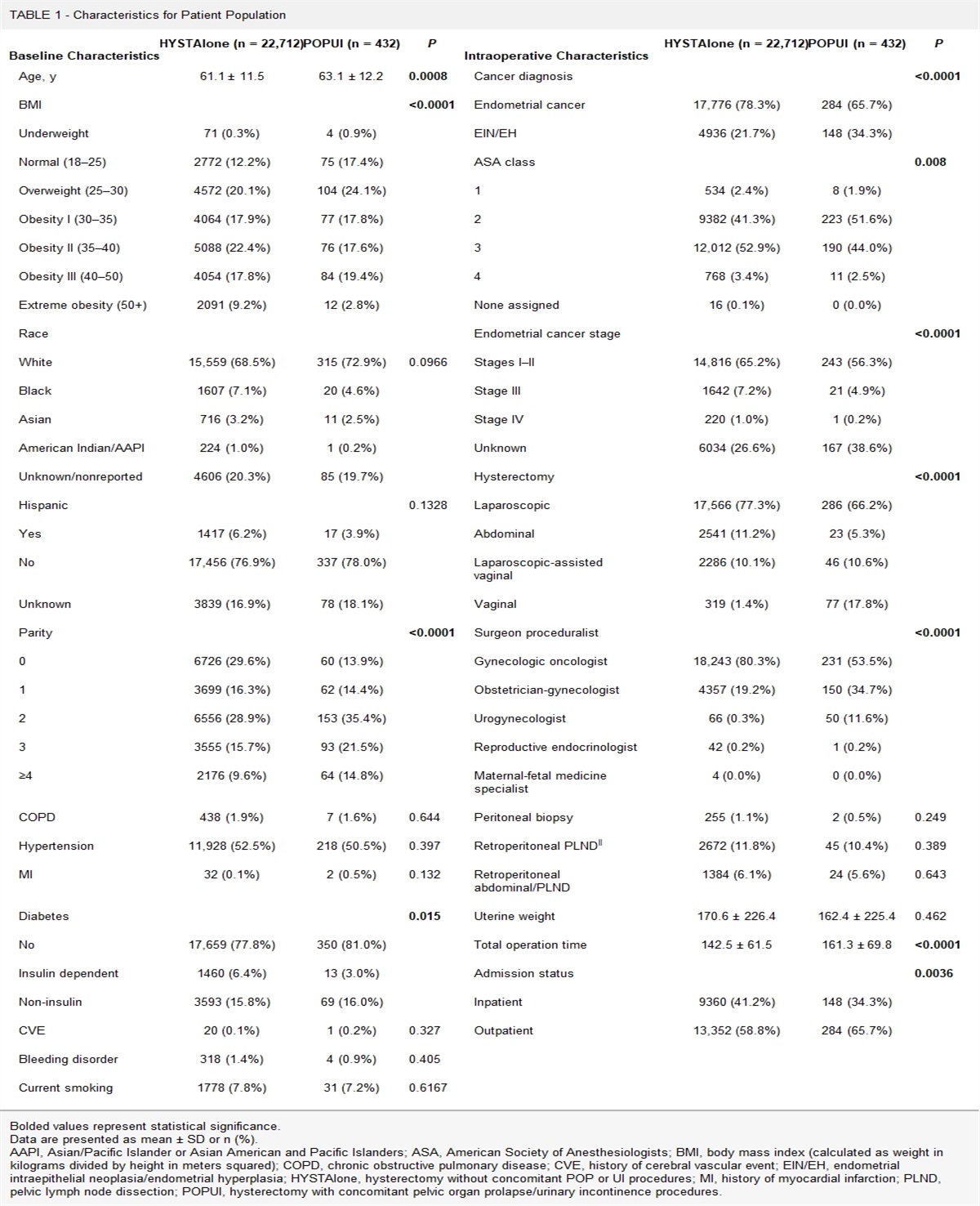
RESULTS Participant CharacteristicsBetween March and September 2019, 23 participants at 7 sites met eligibility criteria, consented to enroll, and were reimplanted with the device. Participant mean age was 63.6 ± 11.0 years, and 22 (96%) were women. There were no participants that discontinued during the study before primary or secondary endpoints. Baseline data obtained from the feasibility study for these 23 participants were used as the baseline data for this study (Table 1). Data were incomplete for 1 participant at 24 weeks: the participant was nonadherent in completing a voiding diary at this visit. Although not required to wash off or refrain from OAB medication for this follow-on study, none of the participants in this study began, continued, or restarted taking OAB medication.
 TABLE 1:
TABLE 1: Baseline Demographics of 23 Trial Participants
Efficacy OutcomesAt baseline, the 23 study participants experienced a median of 3.3 episodes of UUI per day (range, 1–14.0). After reimplantation and activation of the new study device, the median number of UUI episodes decreased to 1.3 at 12 weeks (P < 0.001), and 0.7 at 24 weeks (P < 0.001) (Table 2).
 TABLE 2:
TABLE 2: Efficacy Outcomes of 23 Trial Participants Obtained From Voiding Diary Data
At the final follow-up visit of the feasibility study, data were available for 22 of the 23 participants who enrolled in this reimplantation study. Of these 22 participants, 73% (16 of 22) were considered responders at this 12-month follow-up endpoint of the feasibility study.
The responder rate achieved in the feasibility was reached again in this study. After reimplantation and activation of the new study device, 74% of participants (17 of 23) were responders to the therapy at the 12-week primary endpoint (Fig. 1). Of these responders, a total of 71% (12 of 17) had at least a ≥ 75% reduction in UUI symptoms compared to baseline, with 4 participants completely dry (Table 2). The responder rate was maintained at 82% of participants (18 of 22) after 24 weeks of treatment (Fig. 1). The percentage of responders that were completely dry after 24 weeks increased to 44% (8 of 18). These results suggest that significant improvement in UUI symptoms are achievable and sustainable with continued exposure to therapy via a replacement device.
 FIGURE 1:
FIGURE 1: Average improvement in urgency urinary incontinence (UUI) in all participants with implants at 12 weeks of therapy (n = 23) and at 24 weeks of therapy (n = 22), showing sustained continuous improvement in therapy over duration of study.
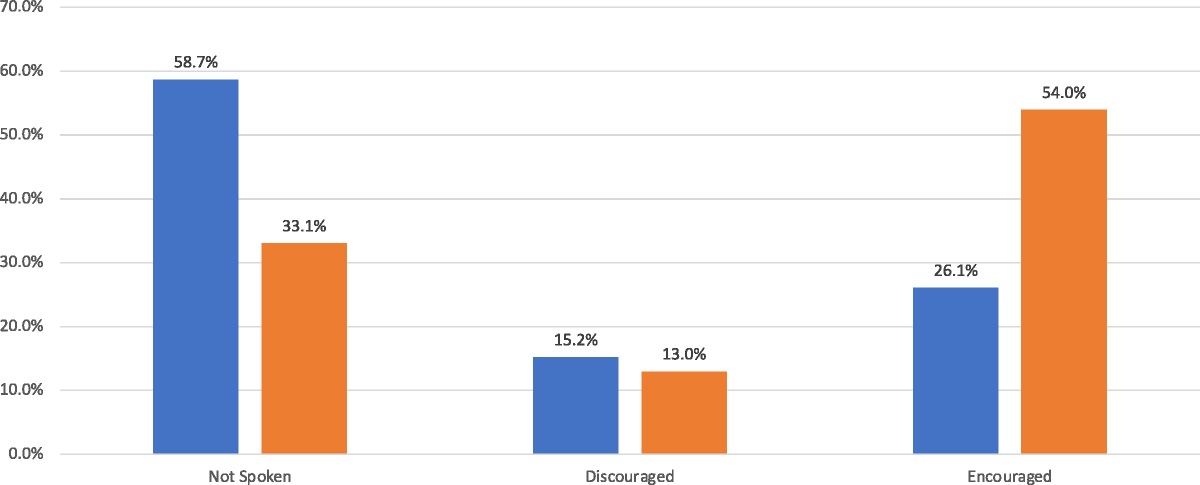
Patient-Reported OutcomesThe I-QOL and PGI-I questionnaires were completed at each follow-up visit. The mean I-QOL scores for the 23 participants assessed at baseline from the original feasibility study serve as the baseline for comparisons in this study. The mean I-QOL score at baseline was 50.1 ± 19.2. At 12 weeks, participants reported a substantial improvement in their quality of life, demonstrated by a significant increase in I-QOL scores and favorable PGI-I results. Participants’ I-QOL scores improved by an average of 25.1 (16.7, 33.5) from baseline (P < 0.001). This is more than 4 times the minimal clinically important difference for the I-QOL of 6.3 for within-treatment groups.15 The mean PGI-I score was 5.3 ± 1.4 at 12 weeks. A total of 18 of 23 (78%) participants responded with scores of 5 or greater (“better,” “much better,” or “very much better”), consistent with the size of the responder population. Of those 4 of 23 (17.4%) participants reported feeling “very much better” (the highest possible score), which is consistent with the proportion of dry patients. Three of 23 (13%) of participants rated themselves as “same” and only 2 of 23 (8.7%) of participants rated themselves as “worse,” “much worse,” or “very much worse” (Table 3).
 TABLE 3:
TABLE 3: Patient-Reported Quality of Life Outcomes for All 23 Trial Participants Obtained From I-QOL and PGI-I Questionnaires
At 24 weeks, patient reported outcomes improved further, demonstrated by an average I-QOL score increase of 28.1 (20.8, 35.5) (P < 0.001), and even greater PGI-I results. A total of 18 of 23 (78%) participants responded with scores ≥5 (better, much better, or very much better), consistent with the size of the responder population. Of those, 10 of 23 (43.4%) participants reported feeling “very much better” (the highest possible score), which is consistent with the proportion of dry patients. Three of 23 (13%) participants rated themselves as “same” and only 2 of 23 participants (8.7%) rated themselves as “worse,” with no participants rating themselves as “much worse” or “very much worse” (Table 3).
SafetyMean time to reimplantation, from incision to final suture, was 24.4 ± 9.3 min (N = 23). There were 8 device-related AEs reported from a total of 21.7% of the participants (5 of 23) all of which were typical wound healing events. These AEs included discomfort at the incision site (3), swelling at the incision site (2), incision site redness (1), localized dermatitis (1), and bruising of the left posterior calf (1), most of which resolved without any treatment. There were no related serious AEs (Table 4).
 TABLE 4:
TABLE 4: Summary of Adverse Events Safety Data for All 23 Trial Participants
DISCUSSIONThe data presented suggest that reimplantation of the eCoin device is both a safe and effective therapy in the treatment of OAB. Participants previously implanted with the eCoin as part of the feasibility study were shown to have significant sustained improvement in their UUI symptoms after device reimplantation. The responder rate that these participants experienced in the feasibility study (73%) was maintained at 12 weeks (74%) and maintained at 24 weeks (82%). Patients with complete resolution of incontinence were maintained as well, with 41% dry at the last follow-up in the feasibility, and 36% dry at 24 weeks postactivation of the replacement device. Patient-reported outcomes were consistent with objective findings as demonstrated by 78% of participants indicating they felt at least better after 12 weeks of treatment, and 78% of participants feeling at least better after 24 weeks of treatment.
Reimplantation of the eCoin device occurred without complication, with short procedure time events (24.4 ± 9.3 min) by physicians relatively naïve to the replacement procedure. This procedure time was slightly longer than the average implantation time in the previous feasibility study, which is attributed to the steps of incising through scar tissue and careful incision of the fibrous capsule to maintain its integrity. Although device related AEs were observed in 5 (21.7%) participants, there were no severe AEs, and all were resolved without complication. The strong safety results of the reimplantation procedure, combined with the impressive efficacy results of treatment, suggest that eCoin is a favorable, sustainable treatment for OAB with UUI.
At the 24-week assessment visit, an average of more than 120 weeks had elapsed because participants were first implanted with eCoin. The consistent efficacy of treatment displayed in this follow-on trial confirms that if a patient responds, the therapeutic effects of eCoin are sustained over time. With more than three quarters of participants stating their symptoms are at least better with eCoin, the potential for lifelong therapy is achievable. Upon depletion of the eCoin battery, patients can have their device replaced in less than half an hour without use of general anesthesia.
Third-line options fail to strike a balance between logistical durability and invasiveness. Adherence to percutaneous tibial nerve stimulation (PTNS) therapy is difficult; retrospective studies show real-life median follow-up of 4 months and high discontinuation rates due to logistical difficulties and physician strain.16 Sacral neuromodulation may be seen as the more durable option, ; however, it is associated with a substantial rate of reoperation for revision or removal of the device in 24–38% of patients.17–19 A physician’s office or clinic visit for a 24-minute eCoin device replacement procedure on average every 3 years significantly lessens the treatment burden on patients, and makes maintenance therapy hassle-free without the need for the patient to recharge the battery or change the stimulation program.
There are some limitations to this follow-on study. The relatively small cohort of 23 patients limits the power to detect subtle differences. Further randomized comparative effectiveness studies are needed to establish the long-term safety and efficacy of the device. The proposed average battery life for the eCoin OAB-02A implanted in this study is 2.8 years. It remains to be seen the actual average battery longevity of the device because it varies with programmed stimulation amplitude, and participants are still receiving ongoing therapy. Furthermore, this study demonstrated the first replacement of the eCoin device. It remains to be seen if there is any significant impact to the lower extremity tissue from additional device replacement procedures. Modifications to improve the battery longevity for the eCoin device may be studied in the future, including changing some parameters of the stimulation, for example reducing the stimulation impulses from 20 to 10 Hz, which will double the battery life.
The favorable results presented here support the safety and efficacy of reimplantation of this fully implanted, primary battery-powered, eCoin device for the treatment of OAB with symptoms of UUI. The device is easy to reimplant during an office-based procedure and offers patients the potential for sustained significant reductions in—or even complete resolution of—UUI associated with OAB without the use of an external power source. With eCoin, patients who have OAB with UUI have the potential for a convenient, life-long treatment option.
ACKNOWLEDGMENTSThis study was supported by the Valencia Technologies Corp.
REFERENCES 1. Choo MS, Ku JH, Lee JB, et al. Cross-cultural differences for adapting overactive bladder symptoms: results of an epidemiologic survey in Korea. World J Urol 2007;25:505–511. doi:10.1007/s00345-007-0183-6. 2. Corcos J, Schick E. Prevalence of overactive bladder and incontinence in Canada. Can J Urol 2004;11:2278–2284. 3. Coyne KS, Sexton CC, Vats V, et al. National community prevalence of overactive bladder in the United States stratified by sex and age. Urology 2011;77:1081–1087. doi:10.1016/j.urology.2010.08.039. 4. Herschorn S, Gajewski J, Schulz J, et al. A population-based study of urinary symptoms and incontinence: the Canadian Urinary Bladder Survey. BJU Int 2008;101:52–58. doi:10.1111/j.1464-410X.2007.07198.x. 5. Irwin DE, Milsom I, Hunskaar S, et al. Population-based survey of urinary incontinence, overactive bladder, and other lower urinary tract symptoms in five countries: results of the EPIC study. Eur Urol 2006;50:1306–1314. doi:10.1016/j.eururo.2006.09.019. 6. Milsom I, Abrams P, Cardozo L, et al. How widespread are the symptoms of an overactive bladder and how are they managed? A population-based prevalence study. BJU Int 2001;87:760–766. doi:10.1046/j.1464-410x.2001.02228.x. 7. Stewart WF, Van Rooyen JB, Cundiff GW, et al. Prevalence and burden of overactive bladder in the United States. World J Urol 2003;20:327–336. doi:10.1007/s00345-002-0301-4. 8. Tikkinen KA, Auvinen A, Tiitinen A, et al. Reproductive factors associated with nocturia and urinary urgency in women: a population-based study in Finland. Am J Obstet Gynecol 2008;199:153.e1–153.e12. doi:10.1016/j.ajog.2008.03.054. 9. Reynolds WS, Fowke J, Dmochowski R. The burden of overactive bladder on US public health. Curr Bladder Dysfunct Rep 2016;11:8–13. doi:10.1007/s11884-016-0344-9. 10. Du C, Berg WT, Siegal AR, et al. A retrospective longitudinal evaluation of new overactive bladder patients in an FPMRS urologist practice: are patients following up and utilizing third-line therapies?Neurourol Urodyn 2021;40:391–396. doi:10.1002/nau.24573. 11. McPherson A. The effects of somatic stimuli on the bladder in the cat. J Physiol 1966;185:185–196. doi:10.1113/jphysiol.1966.sp007980. 12. Vandoninck V, Van Balken MR, Finazzi Agró E, et al. Posterior tibial nerve stimulation in the treatment of urge incontinence. Neurourol Urodyn 2003;22:17–23. doi:10.1002/nau.10036. 13. MacDiarmid S, Staskin DR, Lucente V, et al. Feasibility of a fully implanted, nickel sized and shaped tibial nerve stimulator for the treatment of overactive bladder syndrome with urgency urinary incontinence. J Urol 2019;201:967–972. doi:10.1016/j.juro.2018.10.017. 14. Patrick DL, Martin ML, Bushnell DM, et al. Quality of life of women with urinary incontinence: further development of the incontinence quality of life instrument (I-QOL). Urology 1999;53:71–76. doi:10.1016/s0090-4295(98)00454-3. 15. Yalcin I, Patrick DL, Summers K, et al. Minimal clinically important differences in incontinence quality-of-life scores in stress urinary incontinence. Urology 2006;67:1304–1308. doi:10.1016/j.urology.2005.12.006. 16. Te Dorsthorst MJ, Heesakkers JPFA, van Balken MR. Long-term real-life adherence of percutaneous tibial nerve stimulation in over 400 patients. Neurourol Urodyn 2020;39:702–706. doi:10.1002/nau.24254. 17. Peters KM, Killinger KA, Gilleran JP, et al. Predictors of reoperation after sacral neuromodulation: a single institution evaluation of over 400 patients. Neurourol Urodyn 2017;36:354–359. doi:10.1002/nau.22929. 18. Shih C, Miller JL, Fialkow M, et al. Reoperation after sacral neuromodulation therapy: a single-institution experience. Female Pelvic Med Reconstr Surg 2013;19:175–178. doi:10.1097/SPV.0b013e31828ab3c9. 19. Yazdany T, Bhatia N, Nguyen J. Determining outcomes, adverse events, and predictors of success after sacral neuromodulation for lower urinary disorders in women. Int Urogynecol J 2011;22:1549–1554. doi:10.1007/s00192-011-1512-2.
留言 (0)