
記住我


Adeel Khan, MD and Justin Karstadt
Affiliations: University of Toronto and McMaster University.
Objective: We describe a new technique of platelet-rich plasmas (PRP) infiltration for the treatment of severe foot osteoarthritis. PRP intra-articular infiltration is a promising treatment for osteoarthritis, but it still has some limitations in high-degree osteoarthritis.
Study Design: Single Patient Case Report.
Subject: Thirty-seven-year-old man with a history of chronic left foot pain with failure of pain management and wanted to avoid surgical fusion.
Intervention: Fluoroscopically-guided intraosseous (Arrow OnControl Powered Bone Access System) PRP injection was advanced into the bone approximately 1 cm deep, using the marked lines of the needle as reference (Fig. 2 & 3). The power driver was removed from the hub and a syringe containing 3 mL of activated LR-PRP was attached to the trocar and totally injected into the 5th MT.
Outcome Measures: The outcome measurements were foot function and visual analog scale pain ratings for 3 different situations: foot pain during sport activity, foot pain 1 hour after sport activity and foot pain after standing on feet for 30 minutes. The outcome measurements were assessed at baseline, 1, and 6 weeks.
Results: The patient's NRS pain scale value one week after the intraosseous injection was 1/10; 6 weeks after the intraosseous injection the NRS value was 0/10. The swelling, increased warmth, and redness seen in the pre-treatment physical examination were absent 6 weeks post intraosseous injection. All prior symptoms and examination findings were alleviated post-treatment, aside from the deformity due to the previous fracture. Full mobility was restored and there was 100% pain resolution allowing the patient to continue their work as a contractor and resume their ADLs with no limitations.
Conclusions: To the best of our knowledge, we present the first case report of the combined use of intraosseous and intra-articular LR-PRP to treat severe BME and incomplete stress fracture of the proximal 5th MT with advanced OA. This minimally invasive biological approach resulted in complete resolution of pain and functional symptomology at 6 weeks post initial injection. Additional case reports and clinical studies using this treatment approach would be necessary to support our preliminary clinical results.
Baseline Vestibulo-Ocular Motor Screen Assessment in Youth Ice Hockey Players: Factors Influencing Performance?Paul H. Eliason, PhD,*,†,‡,§,¶ Olivia Galea, PT, PhD,*,†,‡,§,¶ Carolyn A. Emery, PT, PhD*,†,‡,§,¶,‖,**, and Kathryn J. Schneider, PT, PhD*,†,‡,§,¶,††,‡‡
Affiliations: *Sport Injury Prevention Research Centre, Faculty of Kinesiology, University of Calgary, Calgary, AB, Canada; †Alberta Children's Hospital Research Institute, University of Calgary, Calgary, AB, Canada; ‡O'Brien Institute for Public Health, University of Calgary, Calgary, AB, Canada; §Hotchkiss Brain Institute, University of Calgary, Calgary, AB, Canada; ¶Integrated Concussion Research Program, University of Calgary, Calgary, AB, Canada; ‖Community Health Sciences, Cumming School of Medicine, University of Calgary, Calgary, AB, Canada; **Pediatrics, Cumming School of Medicine, University of Calgary, Calgary, AB, Canada; ††Evidence Sport and Spinal Therapy, Calgary, AB, Canada; and ‡‡Sport Medicine Centre, Faculty of Kinesiology, University of Calgary.
Objective: To investigate the effect of sex and previous concussion history on baseline measures of the Vestibulo-Ocular Motor Screen (VOMS) in youth ice hockey players.
Study Design: Cross-sectional.
Subjects: A total of 915 youth ice hockey players (136 female, 770 male, 9 preferred not to respond or unknown; ages 10-18) completed baseline VOMS testing and were recruited from teams in Calgary, Alberta over 2 seasons of play (2016/17 and 2017/18); 101 participants participated in both seasons.
Observation Technique: Players completed an annual preseason baseline questionnaire including demographics and medical history (eg, number of previous concussions, diagnosed migraine disorder).
Outcome Measures: Increased symptoms [≥ 2 on the Numeric Pain Rating Scale (/10)] from baseline for headache, dizziness, nausea, fogginess after the following VOMS components: 1) smooth pursuit, 2) horizontal and vertical saccades, 3) near-point convergence (NPC), 4) horizontal and vertical vestibulo-ocular reflex, and 5) visual motion sensitivity, or abnormal objective measurement of NPC (≥ 6 cm). Mixed-effects logistic regression (adjusted for age and diagnosed migraine disorder) with a random effect at a team level was used to explore the association between sex and number of previous concussions (0, 1, 2+) and VOMS symptom increase or abnormal NPC.
Results: A total of 193 participants (21.09%) indicated increased symptoms or had abnormal NPC during testing. Based on complete-case analysis (n = 856 participants; 129 females, 727 males] with 182 participants having increased symptoms or abnormal NPC, players with 2 + previous concussions had significantly higher odds of having increased symptoms or abnormal NPC than those without a previous history (OR = 2.45; 95%CI: 1.52-3.95). Players with a history of one previous concussion were not associated with increased symptoms or abnormal NPC (OR = 1.19; 95%CI: 0.78-1.81), nor was sex (ORM/F = 1.11; 95%CI: 0.65-1.91), migraine diagnosis (OR = 1.63; 95%CI: 0.81-3.29), or age (OR = 0.99; 95%CI: 0.89-1.11).
Conclusions: Players with a history of 2 or more previous concussions had significantly higher odds of having increased symptoms or abnormal NPC during VOMS testing than those without a history. These results highlight the importance of considering concussion history when interpreting VOMS scores. Future prospective studies, including clinician observed test performance, at preseason, following concussion, and at the time of return to sport will assist in further understanding the effect of concussion on VOMS symptom provocation and clinician observed performance.
Acknowledgements: The Sport Injury Prevention Research Centre is one of the International Research Centres for Prevention of Injury and Protection of Athlete Health supported by the International Olympic Committee. We acknowledge the funding from Canadian Institutes of Health Research, Alberta Innovates Health Solutions, Hotchkiss Brain Institute, and Alberta Children's Hospital Foundation (Integrated Concussion Research Program). Carolyn Emery holds a Canada Research Chair in Concussion. We would like to acknowledge Hockey Canada, Hockey British Columbia, Hockey Edmonton, Airdrie Minor Hockey Association, Hockey Calgary, and all team safety designates, coaches, players, and parents involved for their time and support in completing this research project.
Benefits Outweigh the Risks: A Consensus Statement on the Risks of Physical Activity for People Living With Long-Term ConditionsHamish Reid,*,† Ashley J. Ridout,‡ Simone A. Tomaz,§, Paul Kelly,¶ and Natasha Jones*,‡
Affiliations: *Moving Medicine, Faculty of Sport and Exercise Medicine, Edinburgh, United Kingdom; †Advanced Wellbeing Research Centre, Sheffield Hallam University, Sheffield, United Kingdom; ‡Sport & Exercise Medicine, Oxford University Hospitals NHS Foundation Trust, Nuffield Orthopaedic Centre, Oxford, United Kingdom; §Stirling Physical Activity Research Knowledge and Learning Exchange (SPARKLE), University of Stirling, Stirling, United Kingdom; and ¶Physical Activity for Health Research Centre, University of Edinburgh Institute for Sport Physical Education and Health Sciences, Edinburgh, United Kingdom.
Objective: The benefits of physical activity (PA) for people with long term conditions (LTCs) are well established. However, risks of PA are less well documented and the fear of exacerbating symptoms or experiencing an adverse event are barriers to those with LTCs. Our aim was to agree clear statements for use by healthcare professionals (HCPs) about the medical risks of PA for people with LTCs through expert consensus.
Study Design: A multistage consensus process guided by the Appraisal of Guidelines for Research and Evaluation (AGREE II) tool.
Subjects: The process included authorship (n = 5), stakeholder (n = 4), patient & public involvement (n = 401), practitioner (n = 57), steering (n = 13) and Delphi (n = 29) groups.
Intervention: Supporting evidence and draft statements were tested and refined using a three-stage modified online Delphi study incorporating a broad multidisciplinary expert panel.
Outcome Measures: The Delphi study agreement scale ranged from 1 to 6 (strongly disagree-strongly agree). Satisfactory agreement for Phase 1 required average score >80% (all responses >3). Phase 2 was further stratified with >80% high and 60% to 80% satisfactory agreement.
Results: All statements achieved consensus with final agreement 88.5%–96.5%. Five “impact statements” conclude (1) for people living with LTCs, the benefits of physical activity far outweigh the risks, (2) despite the risks being very low, perceived risk is high, (3) person-centred conversations are essential for addressing perceived risk, (4) everybody has their own starting point and (5) people should stop and seek medical attention if they experience a dramatic increase in symptoms. Eight symptom/syndrome-based statements discuss specific risks for musculoskeletal pain, fatigue, shortness of breath, cardiac chest pain, palpitations, dysglycaemia, cognitive impairment and falls & frailty.
Conclusions: Clear, consistent messaging on risk will improve the confidence of people living with LTCs to be physically active and help reduce cross-sector barriers to engagement. Addressing individual fears of adverse events will help HCPs effect meaningful behavioural change. Evidence does not support routine preparticipation medical clearance for people with stable LTCs if they build up gradually from their current level. The need for medical guidance (rather than clearance) should be determined by individuals with specific concerns or active symptoms.
Higher Rates of Head Contacts and Injuries in Female Ringette Compared to Ice Hockey: An Opportunity for PreventionEmily E. Heming, BSc,* Alexandra J. Sobry, BSc,* Alexis L. Cairo, BSc,* Rylen A. Williamson, BSc,* Ash T. Kolstad, MSc,* Stephen W. West, PhD,*,† and Carolyn A. Emery, PT, PhD*,†,‡,§,¶,‖,**
Affiliations: *Sport Injury Prevention Research Centre, Faculty of Kinesiology, University of Calgary, Calgary, AB, Canada; †O'Brien Institute for Public Health, University of Calgary, Calgary, AB, Canada; ‡Alberta Children's Hospital Research Institute, University of Calgary, Calgary, AB, Canada; §Hotchkiss Brain Institute, University of Calgary, Calgary, AB, Canada; ¶McCaig Institute for Bone and Joint Health, University of Calgary, Calgary, AB, Canada; ‖Community Health Sciences, Cumming School of Medicine, University of Calgary, Calgary, AB, Canada; **Department of Pediatrics, Cumming School of Medicine, University of Calgary, Calgary, AB, Canada.
Objective: Female ringette and ice hockey are high participation female team ice sports in Canada. Both have high injury rates, despite disallowing body checking. This study aimed to compare physical contacts (PC) incidence rates (IR), including head contacts (HC), and suspected injuries in female varsity ringette and hockey using video-analysis.
Study Design: Cross-sectional.
Subjects: Canadian female university ringette and hockey playoff/tournament games in the 2018 to 2019/2019 to 2020 seasons.
Observation Technique: Game video-recordings were analyzed using Dartfish video-analysis software. Validated criteria were used to assess PC intensity (levels 1-3 = lower intensity player-to-player contact, levels 4-5 = higher intensity body checking), PC type (eg, trunk or limb contact), HC type (HC1 = direct player-to-player, HC2 = indirect environmental), suspected injury (concussion, musculoskeletal), and penalty enforcement.
Outcome Measures: Univariate Poisson regression analyses (adjusted for cluster by team, offset by game-minutes) were used to estimate PC, HC, and suspected injury IRs and incidence rate ratios (IRRs) comparing sports. Proportions of high intensity body checks and HC1s that were penalized were reported.
Results: Analyses of 36 team-games (n = 18 ringette, n = 18 ice hockey) revealed that ringette had a 19% lower rate (IRR = 0.81, 95%CI:0.73-0.90) of PCs (IR = 310.38 contacts/100 team-minutes, 95% CI: 285.40-337.54) than hockey (IR = 382.48 contacts/100 team-minutes, 95% CI: 356.80-410.00). However, ringette had a 68% higher rate (IRR = 1.68, 95% CI: 1.22-2.31) of HCs (IR = 17.92 contacts/100 team-minutes, 95% CI: 14.71-21.83) compared to ice hockey (IR = 10.67 contacts/100 team-minutes, 95% CI: 8.28-13.75). Further, ringette had a 3-fold higher rate (IRR = 3.11, 95% CI: 1.13-8.60) of suspected injury (IR = 1.46 injuries/100 team-minutes, 95% CI: 0.72-2.93) compared to hockey (IR = 0.47 injuries/100 team-minutes, 95% CI: 0.22-1.00). Ringette also had a higher rate (IRR = 4.67, 95% CI: 0.92-23.61) of suspected concussion (IR = 0.87 concussions/100 team-minutes, 95% CI: 0.34-2.24) compared to hockey (IR = 0.19 concussions/100 team-minutes, 95% CI: 0.05-0.72), however not statistically significant. The proportion of body checks penalized (ringette = 22%, hockey = 15%) and HC1s penalized (ringette = 14%, hockey = 5%) were low in both sports.
Conclusions: While video-analysis revealed a lower rate of overall PCs in ringette than female hockey, ringette had a 68% higher rate of HCs and 3-fold higher rate of suspected injuries than hockey. Further, despite rules disallowing body checking and HCs in both sports, the proportions of each penalized were low for both sports. These findings will inform future research targeting injury prevention strategies in female ringette and ice hockey.
National Experiences Among Sport and Exercise Medicine Residents Trained During the COVID-19 PandemicA. Devon, MD,* G. Briscoe, MD, MBA, CCFP, Dip. Sport Med,* A. Wakabayashi, MSc,* and K. Carter, MD, CCFP, EM*
Affiliation: *Schulich School of Medicine and Dentistry, Western University, London, ON, Canada.
Objective: Currently, the sport medicine community does not have a full understanding of the impact of the COVID-19 pandemic on the training of sport and exercise medicine (SEM) residents across Canada. The College of Family Physicians of Canada (CFPC) has published 31 core competencies essential for the practice of sport medicine. These competencies are classified into 5 domains: musculoskeletal assessment, exercise medicine, urgent/emergent conditions, anti-doping and mental health. We aimed to assess graduating SEM residents' preparedness for independent practice across these competencies to better understand the impact of COVID-19 on their training.
Study Design: Cross-sectional survey.
Subjects: Tweleve of the 19 2020 to 2021 Canadian SEM residents completed the survey.
Observation Technique: Data was collected in survey form by way of 5-point scale Likert-format and short answer questions.
Outcome Measures: Our primary outcome was self-assessment of readiness for transition to practice in SEM with survey questions based on the 31 CFPC core competencies of SEM. Our secondary outcomes included hours of event coverage, education and use of virtual care during training, and identification of novel learning opportunities that developed due to the pandemic.
Results: They reported a mean of 46.13 hours worked per week with virtual care accounting for 9% of their average week. Residents reported a mean of 63.17 (range 0-240) hours of total sporting event coverage. We stratified the 12 participants into 2 groups for comparison: those with >50 hours of event coverage (n = 4) and those with <50 hours of event coverage (n = 8). The group with >50 hours of event coverage had higher mean Likert scores in all 5 domains: musculoskeletal assessment (4.63 vs 4.33), exercise medicine (3.90 vs 3.88), urgent/emergent conditions (4.06 vs 3.62), anti-doping (3.92 vs 3.42) and mental health (4.09 vs 3.96).
Conclusions: Residents with decreased event coverage had decreased confidence, specifically in the domains of urgent/emergent conditions and anti-doping. Additionally, Residents identified novel learning experiences that may be helpful to mitigate the negative impact of the pandemic including programs facilitating travel for on-field experience, acute injuries clinics, on-field simulation, virtual care teaching and continuing opportunities for involvement with varsity team coverage even after graduation.
Direct Impact Bone Injuries of the Midfoot and Ankle in Professional Ice Hockey Players: Epidemiologic Findings and Return to PlayJordan Deneau, MHK, MD(c),* Mark Cairns, MSc, MD,† John Theodoropoulos, MSc, MD†,‡,§
Affiliations: *University of Toronto Temerty Faculty of Medicine, Toronto, ON, Canada; †University of Toronto Orthopaedic Sports Medicine, Toronto, ON, Canada; ‡Women's College Hospital, Toronto, ON, Canada; §Mt. Sinai Hospital, Toronto, ON, Canada.
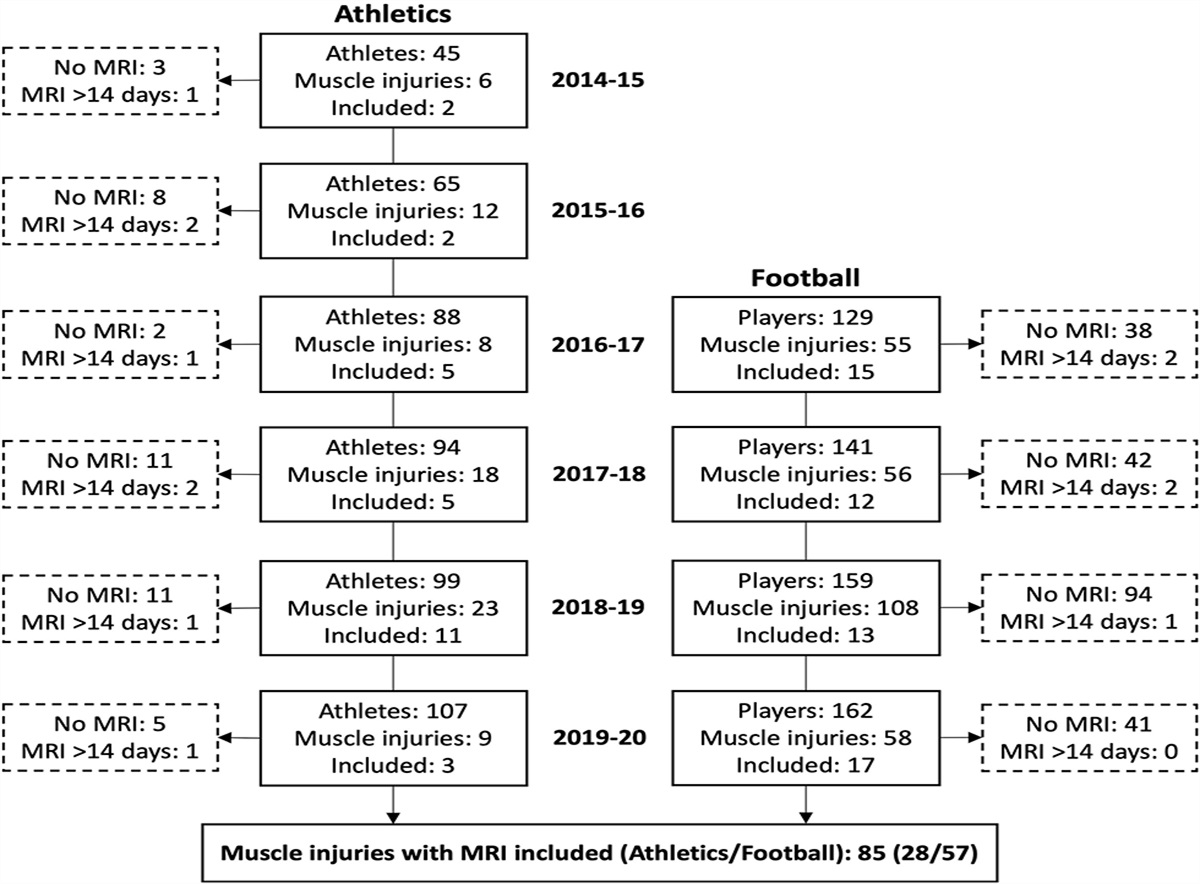
Objective: To evaluate the epidemiologic, clinical, and imaging findings in professional ice hockey players who sustained bone injuries of the midfoot and ankle after direct impact from a moving puck.
Study Design: Retrospective case series.
Subjects: Fifteen acute injuries among 14 current or retired NHL professional ice hockey players (mean age at injury, 26.6 years) who had sustained and were assessed for a clinically suspected foot or ankle injury after a direct impact incident from a moving puck in a game between the 2008 to 2009 and 2020 to 2021 seasons.
Intervention/Observation Technique: Relevant clinical charts and imaging data were retrospectively reviewed.
Outcome Measures: Fracture diagnosis and characterization, player position associated with fracture, initial advanced imaging choice and findings, as well as mean games missed.
Results: Nine of the 15 injuries assessed were identified to have a fracture (60%). Of the 9 fractures identified, 6 were medial (67%) and 3 were lateral (33%). Navicular fractures predominated (n = 5), constituting 80% of medial fractures and 56% of all fractures. Remaining fracture types included lateral malleolus (n = 2) medial malleolus (n = 1), and fifth metatarsal (n = 1). Four of 6 defensemen (67%) and 5 of 9 forwards (56%) were found to have fractures, although there was no statistically significant difference between positions, (P > 0.05, Fisher exact test). After initial x-rays were obtained, CT was the next advanced imaging modality chosen for all players (100%). Initial CT was positive for 8 of the 9 fractures identified (89%). The remaining fracture was identified on subsequent MRI after initial negative CT. The mean number of games missed by players with a fracture was 17.7, compared to 0.5 games among those without fracture (P < 0.05, t test).
Conclusions: Fractures of the midfoot and ankle, particularly of the navicular, were common among clinically suspected cases after a direct impact incident and were associated with a prolonged return to play. CT was frequently chosen as the first advanced imaging modality and successfully identified most fractures.
The Effects of Attentional Focus and Dual-Tasking on Conventional Deadlift Performance in Experienced LiftersAlan Chan, MSc,* Travis Davidson, MD, PhD,† Gordon Robertson, PhD,* and Yves Lajoie, PhD*
Affiliations: *School of Human Kinetics, University of Ottawa, Ottawa, ON; and †Division of Physical Medicine and Rehabilitation, University of Ottawa, Ottawa, ON.
Objective: The purpose of the present study was to examine the effects of attentional focus [internal focus (IF) versus external focus (EF) versus cognitive control task [COG]) on the biomechanics of performing heavily loaded barbell movements.
Study Design: Cross-sectional, multiple session, experimental study design.
Subjects: Fifteen resistance-trained males (age = 23.3 ± 3.4 years) capable of conventional deadlift of at least twice bodyweight (Estimated 1RM 215.1 ± 27.2 kg).
Intervention/observation techniques: Participants participated in 3 separate experimental sessions. The first visit consisted of a five-repetition maximum (5RM) test on the conventional deadlift. During the subsequent sessions, the participants performed a total of 12 single conventional deadlift repetitions while adopting an IF, an EF, or COG. Three-dimensional motion capture and force platforms were used to collect kinematic and kinetic data.
Outcome Measures: Motion capture evaluated kinetic measures about the hip and barbell kinematics and the force platforms extracted variables concerning centres of pressure.
Results: No significant differences were found between the IF, the EF and the COG for lift duration, peak barbell velocity, peak vertical ground reaction force, area of 95% confidence ellipse, peak hip moments and peak hip powers. Adopting an EF significantly reduced variability of the barbell trajectory and centre of pressure (COP) in the anterior-posterior direction. Mean velocity of COP was also significantly lower for the EF.
Conclusions: Although there were no difference in our performance parameters, our findings suggest that adopting an EF may lead to greater postural stability when performing a near maximal physical effort which could suggest a decreased risk of injury from the movement.
Surgical Outcomes for Long Head of the Biceps Surgery: An Updated Chart ReviewPaul (Pavlo) Zerebecky, BSc, MBA,* Wyatt Tyndall, BSc,* Robert Downey, BSc,* Michelle McCarron, PhD,† and Aden Mah, BSc, MD,‡ Jeremy Reed, MD§
Affiliations: *University of Saskatchewan - College of Medicine - Office of the Vice-Dean Research, Saskatoon, SK, Canada; †Saskatchewan Health Authority, Regina, SK, Canada; ‡Reed & Dash Sports Medicine Clinic, Regina, SK, Canada; and §University of Saskatchewan - College of Medicine - Office of the Vice-Dean Research, Saskatoon, SK, Canada.
Objective(s): To better understand which technique provides the best surgical outcomes based on improved function and minimizing re-operation. To better inform surgeons in decision making and surgical management of pathology of the Long Head of the Biceps Tendon (LHBT).
Study Design: Retrospective Chart Review followed by Prospective Telephone Interviews.
Subjects: Three hundred twenty-five subjects (167 tenotomy and 158 tenodesis) who underwent one of 4 tenotomy- or one of 3 tenodesis-based surgical techniques for management of LHBT pathology.
Intervention: Tenotomy-based surgical techniques: 1) Arthroscopic tenotomy; 2) Arthroscopic shortening and tenotomy; 3) Arthroscopic tenotomy with mini open shortening; 4) Arthroscopic tenotomy with mini open shortening and debridement of bicipital groove. Tenodesis-based surgical techniques: 5) Arthroscopic tenotomy with mini open tenodesis, drawn in; 6) Arthroscopic tenotomy with mini open tenodesis, pushed in; 7) Arthroscopic tenotomy with mini open tenodesis, pushed in with bicep groove debridement.
Outcome Measures: The primary outcome measure was the requirement for further intervention following the LHBT surgery (cortisone injection or another surgery) assessed by chart review. The secondary outcome measures were the patient's personal satisfaction with the procedure (Single Assessment Numeric Evaluation (SANE) score) and the patient's subjective restriction in function following the surgery (assessed using a single ranking question with 5 possible answers).
Results: Patients who underwent tenotomy with tenodesis (12%) were significantly more likely to require subsequent intervention than were patients who underwent tenotomy alone (4.2%), χ21 = 6.687, P = 0.010. Patients who indicated that they were able to do everything as they could before their problems started, nearly two-thirds (62.1%) had undergone tenotomy as opposed to tenodesis (χ24 = 9.970, P = 0.041). Both tenotomy and tenodesis patients overwhelmingly reported being glad (90.4% vs 93%, respectively) that the surgery was performed and that they would have the surgery again (88.6% vs 90.4%, respectively). Median SANE scores were high in both tenotomy (Median = 85, IQR = 73.75-95) and tenodesis (Median = 85, IQR = 75-90) patients.
Conclusions: It appears that biceps tenotomy alone is superior to tenotomy with tenodesis in decreasing the rate of re-operation and improving functional outcomes, although, both tenotomy and tenodesis procedures appear to produce high patient satisfaction.
Acknowledgments: University of Saskatchewan - College of Medicine - Office of the Vice-Dean Research.
Assessing Family Resident Confidence and Competency in Ordering Appropriate Diagnostic Imaging for Knee Pain in Primary CareSheniz J. Eryuzlu, MD, and David W. Lawrence, MPH, MD
Affiliations: University of Toronto, Toronto, ON, Canada.
Objective: To assess the confidence and competency among family medicine residents in ordering appropriate ultrasound (US) and MRI imaging for knee pain in primary care.
Study Design: Quality improvement study.
Subjects: Thirty-seven University of Toronto Family & Community Medicine Residents (PGY1 and PGY2).
Intervention: A pre-post case-based survey to assess the efficacy of a didactic lecture focusing on appropriate imaging (particularly ultrasound vs MRI) utilization for knee-specific conditions. The case-based survey was validated first by 11 academic staff sports medicine physicians, all of whom reached consensus on the “correct” selection of image modality for each case.
Outcome Measures: Primary outcomes were pre-teaching and post-teaching scores, and self-rated confidence in ordering knee imaging.
Results: There were 22 PGY1 respondents and 15 PGY2 respondents pre-teaching, and only one PGY1 lost to follow-up post-teaching. The average number of days that each resident had completed in residency MSK rotations was approximately 4.5 days. Across all residents, the average pre-teaching correct score was 54%, compared to 88% after teaching. The cases on ACL injuries had the lowest average pre-teaching correct scores (38%). All 3 groups showed a statistically significant increase in their scores post-teaching (P < 0.0001 for PGY1, PGY2, and total cohort). The predominant change in correct answers in all 3 groups was attributed to a decrease in ordering unnecessary US and MRI following the teaching. Prior to the education session, the average self-rated confidence in appropriately ordering knee imaging was between “poor” and “fair”, with a statistically significant increase in confidence post-teaching to between “fair” and “good” (P < 0.0001). There was a statistically significant correlation between number of weeks in MSK rotations and self-rated MSK knowledge (P = 0.02), but no statistically significant correlation between weeks in MSK rotations and pre-teaching confidence in ordering knee imaging or pre-teaching score.
Conclusion: This study highlights the efficacy and need for increased exposure to MSK teaching within family & community medicine curriculum.
Age and Pacing Strategies Differences Between Younger and Older Canadian Competitive Cross-Country SkiersPatricia K. Doyle-Baker, DrPH/PhD, MSc, CEP,*,† Anneke Winegarden, MSc,* Tak Fung, PhD,‡ Louis Passfield, PhD,*,§
Affiliations: *Human Performance Lab, Faculty of Kinesiology, University of Calgary, Calgary, AB, Canada; †Alberta Children's Hospital Research Institute, University of Calgary, Calgary, AB, Canada; ‡Research Computing Services, Information Technologies, University of Calgary, AB, Canada; and §Endurance Research Group, School of Sport and Exercise Sciences, University of Kent, Chatham Maritime, Kent, United Kingdom.
Objective: The study explored the influence of sex, age and pacing strategies on 3 km track time trial (TT) performance following a lap-based high-intensity interval training (HITT) protocal in cross-country (XC) skiers at a national level of competition or greater.
Study Design: Quasi experimental design -field based study at track venues (Ottawa, ON; Montreal, QC; Revelstoke, BC; Calgary, AB).
Subjects: Thirty-nine (N = 63) athletes from 9 different teams met the inclusion criteria (76% F).
Intervention/Observation Technique: Nordiq Canada (2018) uses the 3 km TT on a 400 m track to monitor improvement over a season. Change in performance is based on TT differences with a performance decrement considered a negative change and a performance improvement a positive change. The 3 km TT consists of 7.5 laps, with the first 600 m considered as lap 1 as the first 200 m lap time is not recorded. Lap times are collected using Webscorer © and converted to average speed per lap (m/s), with an average lap time for the entire TT calculated. Pacing strategy is calculated by sum of the differences of each individual lap from the average lap speed.
Outcome measures: The influence of age and pacing was analyzed by group (under (u)18 or older than 18(+) years). A two-tailed, unpaired t test determined differences in mean performance change between groups. A significance value of P ≤ 0.05 was set.
Results: Improvement in pacing strategy in u18 (16-17 years) was observed post the HIIT (P = 0.02), but did not result in improved performance (P = 0.09). Most 18+ (18-28 years) did not improve their pacing strategy (P = 0.23), but those who did, improved their performance (P = 0.048). The difference in performance change between groups was not significant (P = 0.06). Mean performance change in u18 and 18+ was 1.78 ± 2.59% and 0.24 ± 2.38%, respectively.
Conclusions: This study found that younger athletes were more variable in their pacing strategy in comparison to older XC skiers, indicating an improvement in pacing with age. These results highlight the importance of standardizing pre-testing workouts in younger, less experienced athletes. Lack of standardization may lead to unexplained variation in testing results and an inability to make effective conclusions from testing.
Acknowledgments: The authors thank the XC ski coaches and athletes for their participation.
Should Physicians Prescribe Physical Activity to Adults with Adverse Childhood Experiences to Improve Physical and Mental Health?Brook Hadwen, BMSc,* Eva Pila, PhD,† and Jane Thornton, MD, PhD‡,§
Affiliations: *Department of Epidemiology and Biostatistics, Western University, London, ON, Canada; †School of Kinesiology, Western University, London, ON, Canada; ‡Western Centre for Public Health & Family Medicine, Schulich School of Medicine & Dentistry, Western University, London, ON, Canada; and §Fowler Kennedy Sport Medicine Clinic, Western University, London, ON, Canada.
Corresponding Author: Brook Hadwen, Western Corresponding Author: Brook Hadwen, Western Centre for Public Health and Family Medicine, 3rd Floor, 1465 Richmond St, London, ON N6G 2M1 ([email protected]).
Objective: Exercise medicine physicians prescribe physical activity to their patients to improve physical and mental health. Certain patient populations with poor physical and mental health, such as adults with adverse childhood experiences (ACEs), may face barriers preventing engagement in physical activity. Compared to the general population, adults with ACEs have an increased risk for poor physical health and chronic conditions such as cardiovascular disease, pulmonary disease, inflammatory conditions, cancer, and Type 2 diabetes. They also experience a higher burden of depression, anxiety, and other mental health conditions. It is unknown whether physical activity prescription leads to improvements in physical and mental health, and prevention of incident disease, in adults with ACEs. This scoping review aimed to explore whether engaging in physical activity is associated with better physical and mental health among adults with ACEs, and to identify areas that require further research, including further considerations for physical activity counselling.
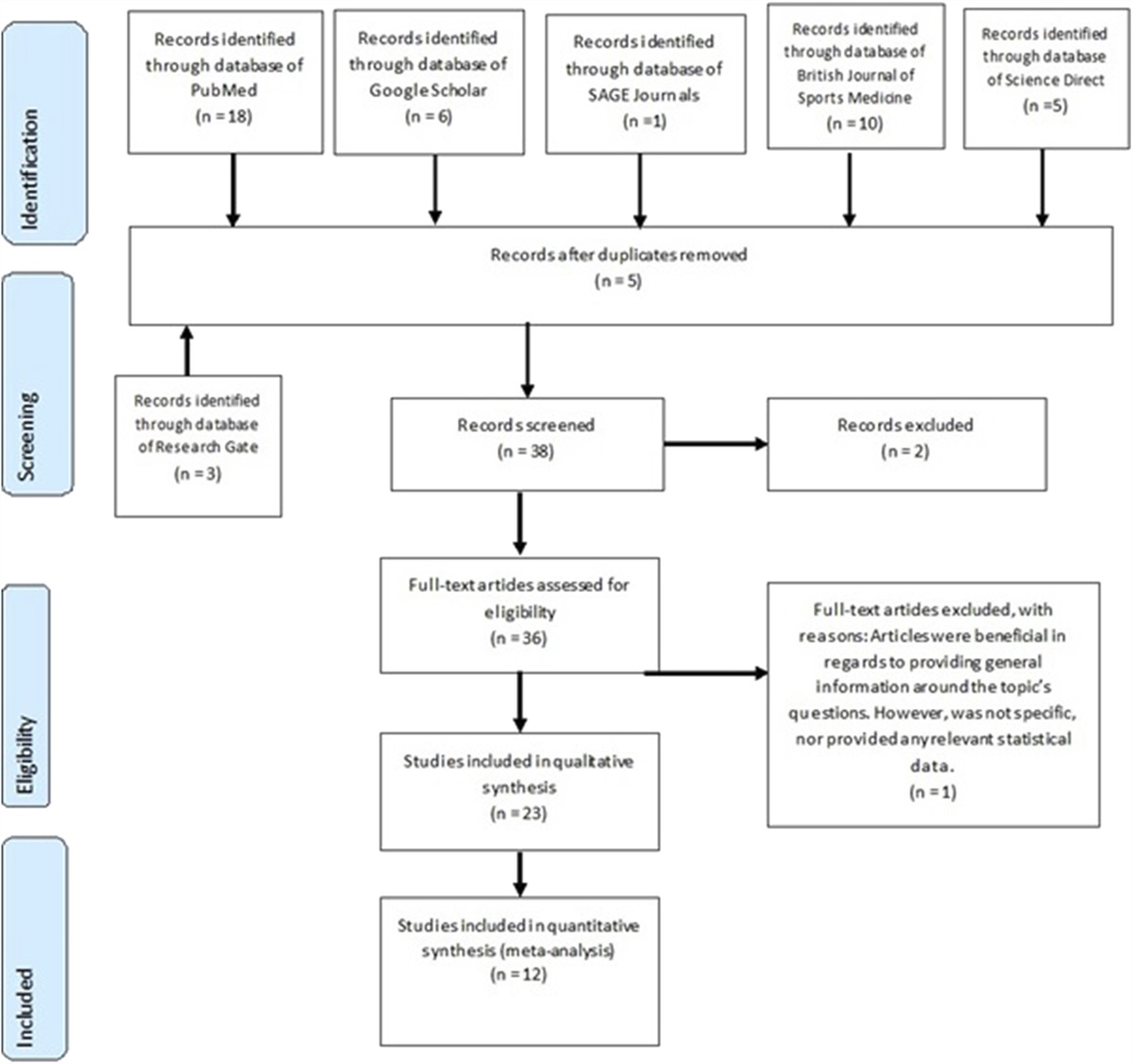
Data Sources: We searched Medline, Scopus, SPORTDiscus, and PsycInfo for relevant articles. Studies were considered eligible if they were articles, dissertations, or abstracts that aimed to explore the relationship between physical activity and physical/mental health in adults with ACEs, and were written in English.
Main Results: Sixteen studies were included. Nine explored physical health as an outcome and 10 explored mental health. Physical activity was associated with better overall self-reported physical health, lower levels of inflammation in middle aged adults, lower resting heart rate in young adults, and improved body composition. Moderate and vigorous physical activity was also associated with lower depressive symptoms. Successful approaches to increase physical activity levels included consistent, one-on-one support.
Conclusions: Physical activity may confer protective effects against poor physical and mental health in adults with ACEs. Sport and exercise medicine physicians should be aware that a high proportion of their patients may suffer from ACEs. Working together in a supportive, consistent manner with these patients can overcome barriers and increase engagement in physical activity. Further research is required to determine optimal frequency and intensity (“dosing”) of physical activity in adults with ACEs, as well as the most effective interventions to improve physical activity engagement.
Acute Responses to High-Intensity Interval Training in 4 Males With Permanent Atrial FibrillationSol Vidal-Almela, MSc,*,† Tasuku Terada, PhD,* Andrew L. Pipe, MD,*,‡ and Jennifer L. Reed, PhD*,†,§
Affiliations: *Exercise Physiology and Cardiovascular Health lab, Division of Cardiac Prevention and Rehabilitation, University of Ottawa Heart Institute, Ottawa; †School of Human Kinetics, Faculty of Health Sciences, University of Ottawa; ‡School of Medicine, Faculty of Medicine, University of Ottawa; and §School of Epidemiology and Public Health, Faculty of Medicine, University of Ottawa.
Objective: Some research has shown that high-intensity interval training (HIIT) improves symptoms and quality of life in patients with atrial fibrillation (AF). Yet, the acute responses to HIIT remain understudied, leaving clinicians and patients hesitant about prescribing and engaging in high-intensity exercise. We present 4 cases of acute exercise responses to HIIT in patients with permanent AF.
Study design: Retrospective case series.
Subjects: Four white males (58-80 years old) with permanent AF, different co-morbidities (eg, diabetes, coronary artery disease, Parkinson's disease, asthma) and physical limitations (ie, low back, knee pain).
Intervention: Ten weeks (3 d/wk) of supervised HIIT at a tertiary care cardiovascular health centre. Each 23-minute HIIT session involved a 2-minute warm-up at 50% peak power output (PPO, based on an exercise test to exhaustion), 16 minutes of HIIT consisting of 2x8-minute blocks (30-second high-intensity bouts at 80%-100% PPO interspersed with 30-second low-intensity bouts at 25% PPO) with a 4-minute active/passive recovery between blocks, and a 1-minute cool-down at 25% PPO.
Outcome measures: Power output, heart rate, blood pressure and any symptoms were recorded during each HIIT session. Ratings of perceived exertion (RPE; 6-20 Borg scale) were recorded after each session.
Results: The participants exercised at a mean PPO of 82% (n = 2), 85% (n = 1) and 90% throughout the 10 weeks. The increases in heart rate (average + 31 to +60 bpm) and blood pressure during HIIT were modest across all participants, regardless of age and medication use, and decreased following cool-down (−22 to −67 bpm) without adverse events. These findings align with the typical exercise responses noted in other cardiovascular populations. The average RPE were in the moderate- (n = 3) and vigorous- (n = 1) intensity range. Differences in RPE responses were observed; the oldest participant perceived the sessions as more challenging despite lower mean heart rate values. This should be considered when monitoring exercise.
Conclusions: Patients' concerns regarding high-intensity exercise may discourage them from participating in HIIT, yet 4 male patients with permanent AF tolerated HIIT without adverse events and similar acute exercise responses than other cardiovascular populations. To facilitate HIIT participation in this population, further investigation and knowledge dissemination are warranted.
Keywords: acute exercise, atrial fibrillation, case report, exercise training, HIIT, physical activity, high-intensity interval training.
Assessing Acute:Chronic Workload Ratio Methodologies for the Prediction of Knee Pain in Men's Elite VolleyballFaraz Damji, MD (cand),* Kerry MacDonald, PhD,†,‡ Michael A. Hunt, PhD,§ Jack Taunton, MD,¶ and Alex Scott, PhD §
Affiliations: *Faculty of Medicine, University of British Columbia, Vancouver, BC, Canada; †Department of Athletics and Recreation, University of British Columbia, Vancouver, BC, Canada; ‡School of Kinesiology, Faculty of Education, University of British Columbia, Vancouver, BC, Canada; §Department of Physical Therapy, Faculty of Medicine, University of British Columbia, Vancouver, BC, Canada; and ¶Division of Sports Medicine, Faculty of Medicine, University of British Columbia, Vancouver, BC, Canada.
Objective: Predicting sports injuries is a complex phenomenon and recent evidence suggests that the acute:chronic workload ratio (ACWR) is a potentially useful tool for quantifying athlete workloads, with athletes at increased risk of injury when the ACWR is higher relative to a lower ACWR. The original definition of the ACWR is the previous week's amount of work compared to the previous 4 week's average amount. The objective of this research study was to assess different definitions of the ACWR for predicting knee pain in elite volleyball athletes. We expected to see agreement with the literature in that ACWR would be positively associated with knee pain.
Study Design: Retrospective, exploratory analysis on a data set collected over the course of one season from a University varsity volleyball team.
Subjects: Twelve male varsity volleyball players enrolled in their first-5th year of University. By position: 2 setters, 4 middles, 4 leftsides, 2 opposites.
Intervention: To analyze how the relationship between ACWR and injury is influenced by methodological choices, we calculated a total of 5 different ACWR variants from the data set: (a) 7:28/coupled/RA, (b) 7:28/uncoupled/RA, (c) 7:21/coupled/RA, (d) 3:21/coupled/RA, and (e) 7:28/coupled/EWMA. RA = rolling average, EWMA = exponentially weighted moving average.
Outcome Measures: The main outcome measurement was knee pain score on a scale that runs from 0 to 10 (0 = No Pain; 10 = Worst Pain). Players self-reported these values immediately after each practice and match throughout the season.
Results: Our mixed effect modelling indicated that the coefficient estimates for the ACWR variants were small and statistically insignificant.
Conclusions: The variant used did not have a major influence on the relationship with knee pain score, and the strength of the relationship was weak. While our findings did not demonstrate statistical significance, we observed concordance with other studies in that the variants of 3:21/coupled/RA and 7:28/coupled/EWMA appeared to be slightly more sensitive. In terms of the ACWR variant of choice for load monitoring, we would recommend using the most traditional variant such that comparisons can be made with other teams, alongside the EWMA variant which has been shown in recent studies to perform better.
Original paper in Transl Sports Med. 2021; 00:1–7.
Rotator Cuff Repair With Graft Augmentation Improves Clinical and Structural Outcomes: A Meta-AnalysisCasey Imbergamo, MD, Sean Sequeira, MD, and Heath Gould, MD
Affiliations: MedStar Orthopaedic Institute, Union Memorial Hospital, Baltimore, Maryland.
Objective: Despite advances in surgical technique, retear rates following rotator cuff repair (RCR) remain high. This has prompted the utilization of grafts to augment repairs. The purpose of this meta-analysis is to evaluate clinical outcomes and retear rates following RCR with autograft or allograft augmentation.
Data Sources: A literature search was conducted using the Medline database. Inclusion criteria for this study were: 1) clinical studies of RCR with autograft or allograft augmentation which included control groups; 2) functional outcome scores and retear rates (confirmed with imaging) reported with minimum one year follow up; 3) minimum sample size of 10 subjects in both experimental and control groups. Each study was reviewed, and data was extracted for number of participants, mean follow-up (months), graft type, retear rates, and clinical outcome measures. Statistical analysis, including student-tests and univariate analysis of variance (ANOVA), were performed.
Main Results: Six studies were included in the meta-analysis, with a total of 257 shoulders (137 graft, 120 control). Two studies each utilized acellular human dermal matrix allograft, fascia lata autograft, and biceps tendon autograft. Average length of follow up was 29.1 months. Mean retear rate in the graft group was 29.2%, compared to 44.2% in the control group (P = 0.008). Mean improvement in UCLA score for graft versus control group was 17.4 (±1.57) versus 15.2 (±1.23) (P < 0.001) Mean improvement in Constant score for graft versus control group was 32.8 (±6.61) versus 28.1 (±7.81) (P = 0.002).
Conclusions: Rotator cuff repair with autograft or allograft augmentation yielded statistically significant improvements in all evaluated outcome measures. However, the clinical implications of these differences must be considered. Further research is warranted to continue investigating the use of graft augmentation in RCR, including human tissue grafts, as well as xenografts and synthetic grafts.
What's All the Ruck-Us About? A Systematic Review and Meta-Analysis of Rates, Risk Factors and Prevention Strategies for Injury and Concussion in Youth RugbyStephen W. West, PhD,*,† Isla J. Shill, MSc,*,‡ Stuart Bailey, PhD,§ Reid A. Syrydiuk, BA,*,¶ K. Alix Hayden, PhD,‖ Debbie Palmer, PhD,§ Amanda M. Black, CAT(C), PhD*,†,‡,¶ Brent Hagel PhD,* Keith A. Stokes PhD Carolyn A. Emery PhD*,†,‡,¶,††,‡‡,¶¶
Affiliations: *Sport Injury Prevention Research Centre, Faculty of Kinesiology, University of Calgary, Calgary, AB, Canada; †O'Brien Institute of Public Health, University of Calgary, Calgary, AB, Canada; ‡Hotchkiss Brain Institute, University of Calgary, Calgary, AB, Canada; §Edinburgh Sports Medicine Research Network, Institute for Sport, PE and Health Sciences, University of Edinburgh, Scotland; ¶Alberta Children's Hospital Research Institute, University of Calgary, Calgary, AB, Canada; ‖Libraries and Cultural Resources, University of Calgary, Calgary, AB, Canada; **Department for Health, University of Bath, Bath, United Kingdom; ††Human Performance Laboratory, Faculty of Kinesiology, University of Calgary, Calgary, AB, Canada; ‡‡Department of Community Health Sciences, Cumming School of Medicine, University of Calgary, Calgary, AB, Canada; and §§Department of Pediatrics, Cumming School of Medicine, University of Calgary, Calgary, AB, Canada.
Objective: This systematic review (SR) and meta-analysis investigates rates and aetiology of injury and concussion, injury risk factors and evaluation of primary prevention strategies in youth rugby.
Data Sources: Nine databases were searched using 3 concepts: injury, youth, and rugby. The search was not limited by date and searches of reference lists of previous reviews was undertaken. Eligible studies were meta-analysed using a DerSimonian Laird random effect model for each age group and sex. Full search strategy and list of sources available on pre-registered Prospero (Ref: CRD42017065645).
Main Results: Sixty-four studies were included in this SR. The rates of match injury (using a 24-hour time loss definition) were 41.7/1000 match-hours (95% CIs: 13.6-69.9) in males and 53.0/1000 match-hours (95% CIs: 37.0-76.0) in females. Concussion rates were 6.2/1000 player-hours (95%CIs: 5.0-7.4) for males and 27/1000 player-hours (95% CIs: 13-41) for females. The most common injury site was the lower limb (males) and the head/neck (females). The most common injury type was ligament (males) and concussion (females). The mechanism of injury was a contact event for 84% of injuries, with the majority occurring in the tackle specifically (54% male, 62% females: in matches and training combined). Median injury severity was 21 days for males and 17 days for females. Twenty-one risk factors were reported in the literature, as well as 8 tackle-specific risk factors. The risk factors with the strongest evidence were higher level of play and increasing age. Primary injury prevention strategies were the focus of only 6 studies and included law changes (n = 2), equipment (n = 3) and training (n = 2) and targeted catastrophic injury (n = 3), all injury (n = 3) and traumatic brain injury/concussion (n = 4). The prevention strategies with the most promising evidence were mouthguard use and neuromuscular training.
Conclusions: There is a significant lack of empirical evidence in the female youth game, suggesting the need to prioritize female rugby players in future research. A focus on high-quality risk factors and primary prevention studies should be considered in examining risk factors for injury. Targeting primary prevention strategies and stakeholder education remain key strategies in the prevention, recognition, and management of injuries and concussions in youth rugby.
Acknowledgements: Stephen West is supported by O'Brien Institute of Public Health and Canadian Institutes of Health Research postdoctoral fellowships. Carolyn Emery holds a Canada Research Chair (Tier 1) in Concussion. Isla Shill is supported through a Hotchkiss Brain Institute doctoral award.
Organizational Risk Profiling and Education Associated with Reduction in Professional Pitching Arm Injuries: A Natural ExperimentEllen Shanley, PT, PhD, OCS, Charles A. Thigpen, ATC, PT, PhD, Gary S. Collins, PhD, Nigel K. Arden, MD, FRCP, Thomas K. Noonan, MD, Michael J. Kissenberth, MD, Douglas J. Wyland, MD, and Garrett S. Bullock, PT, DPT, DPhil
Affiliation: ATI Physical Therapy, Greenville, South Carolina.
Objective: To evaluate the influence of risk profiling and education on arm injury incidence in minor league (MiLB) pitchers and to stratify by injury severity.
Study Design: Natural experiment.
Subjects: Two hundred ninety-seven pitchers (Pre: 119, Post: 178) were included.
Intervention: A prospective cohort was conducted from 2013 to 2019 on MiLB pitchers. Beginning in the 2015 season, pitchers were examined and risk profiled for arm injury. Shoulder external (ER) and internal (IR), total range of motion (TROM), horizontal adduction (HA), and humeral torsion (HT) were measured. Organizational risk profiling and education was implemented in 2015 based on preseason assessments. χ2 were performed to investigate potential differences between shoulder ROM risk categories between the 2013 to 2014 (Pre) and 2015 to 2019 (Post) seasons. Interrupted time series analyses were performed to assess the effect organizational risk profiling and education on arm injury in MiLB pitchers and repeated by injury severity.
Outcome Measures: Shoulder IR ROM risk was defined as <= −15 degrees, ER ROM risk as ≥ 15 degrees, TROM risk as <= −10 degrees, and dominant HA risk as < 0°. Arm injury severity were defined as overall, 7 to 27 days, and 28 + days arm injuries in MiLB pitchers.
Results: Arm injury incidence was 1.5 arm injuries per 1000 athletic exposures. Pitchers in the 2015 to 2019 seasons demonstrated increased preseason shoulder injury risk for IR (P = 0.003) and ER (P = 0.007), while the 2013 to 2014 seasons demonstrated greater HA risk (P = 0.004). There were no differences between seasons for TROM risk (P = 0.760). There was a significant adjusted time loss arm injury reduction for the 2015 to 2019 seasons [0.68 (0.47-0.99)]. Similar relationships were observed for 7 to 27 days [0.62 (0.42-0.93)], but not for 28 + days [0.71 (0.47-1.06)].
Conclusions: Organizational risk profiling and education appear to reduce professional pitching overall and 7 days arm injury risk by 33%-38% but not for 28 days injury risk. This suggests that while injury risk increased over time, organizational risk profiling mitigated the expected increase in arm injury rates. Risk profi
留言 (0)