
記住我


Acute urethritis in men is mostly caused by sexually transmitted infection (STI) Chlamydia trachomatis (CT) or Neisseria gonorrhoeae (NG).1 Distinction between gonococcal urethritis and nongonococcal urethritis (NGU) can be readily made by examination of Gram stains of discharge.2 Empirical treatment is often preferred over delay of treatment awaiting definite molecular test results. Empirical treatment in cases of gonococcal urethritis is ceftriaxone with or without azithromycin.3–5
In most clinical guidelines, identifying a pathogen in NGU is based on molecular testing.3,4,6,7 Recommendations on what pathogens to test vary somewhat, depending on local prevalence. All guidelines recommend testing for CT. The association of Mycoplasma genitalium (MG) with NGU was first described in the 1980s,8 and in the last 2 decades only after molecular tests became available, its role has become more apparent.1,9–11 Some guidelines, such as the Australian,6 have rapidly incorporated testing for MG. In contrast to Australian6 and European guidelines,7 the Centers for Disease Control and Prevention3 and Dutch4 guidelines currently do not recommend standard screening for MG in urethritis, but only in persisting or recurrent NGU.
Different treatment recommendations exist also for treatment of NGU, in part as a consequence of different testing guidelines for MG. Dutch guidelines4 still recommend the macrolide azithromycin (1 g single dose), whereas Australian6 and European guidelines7 recommend doxycycline (100 mg twice daily for 7 days). The Centers for Disease Control and Prevention changed its recommendation from single-dose azithromycin to a course of doxycycline in their recently updated guidelines.3 According to the Australian guidelines, patients with MG urethritis should be additionally treated with azithromycin (1 g stat then 500 mg daily for 3 days) or moxifloxacin (400 mg daily 7 days) after doxycycline resulting in a 10- to 14-day treatment course.6 The European guidelines recommend treatment with azithromycin (500 mg stat, then 250 mg for 4 days) in case of MG urethritis instead of treatment with doxycycline.7
According to a recent study performed at the STI clinics in Amsterdam and The Hague in 2018, the prevalence of MG among men with urogenital symptoms at the STI clinic in Amsterdam is 29%, whereas it was only 6% in 2014.12,13 Among the MG positive samples in the recent study, MG macrolide resistance-associated mutations (MRAM) was detected in 66%.13
A review showed that there is a correlation between MG infection and persistent or recurrent NGU.14 Read et al.15 observed that recurrent or persistent urethral symptoms were more common in patients without microbiological cure (34 of 44 [77%]; 95% confidence interval [CI], 62%–89%) compared with those who were cured (10 of 63 [16%]; 95% CI, 8%–28%; P < 0.001) after azithromycin treatment. Treatment failure was thus associated with MG-MRAM. This—in combination with the high prevalence of MG and rapid increase of antibiotic resistance16—may indicate that current Dutch treatment guidelines for NGU need to be updated and take MG presence and MRAM into account. This study was designed to evaluate the clinical outcome of empirical treatment for both gonococcal urethritis and NGU and whether MG infection and MRAM are of influence.
METHODS Setting of the ClinicThe study was performed at the STI clinic in Amsterdam, the Netherlands. The clinic is part of the Public Health Service, which means it is free of charge for members of the public at risk for STI, with or without referral. Diagnostics and treatment, including empirical treatment, are done according to Dutch guidelines.4 Testing in cases of male urethritis according to those guidelines includes CT and NG, but not MG. Testing for MG is currently only considered optional in cases of (persisting) urethritis. We performed this study to assess if testing for MG would benefit our patient population.
Cases IncludedFrom May 2018 to November 2019, we included all men with urethritis at the STI outpatient clinic in Amsterdam. Men received standard care and treatment and could be included for different episodes. Urethritis was defined as presence of >10 leucocytes per high-power field in Gram stains of urethral discharge. Symptoms were dysuria, discharge, or urethral discomfort. Additional presence of intracellular gram-negative diplococci defined a presumptive diagnosis of gonococcal urethritis.
TreatmentEmpirical treatment for gonococcal urethritis was 1 g ceftriaxone given intramuscularly and for NGU 1 g azithromycin per os, according to local and national guidelines.4 When the use of macrolides was contraindicated in a man with NGU, doxycycline 100 mg twice daily for 1 week was prescribed. Patients were asked to return to the clinic when molecular diagnostics showed NG and patients had not been given ceftriaxone previously, when rectal CT was detected and additional treatment with doxycycline needed, and when syphilis was detected and additional benzathine penicillin was needed.
Molecular Detection of STIsFirst-void urine was collected and routinely tested for NG and CT (Aptima Combo 2; Hologic Inc, San Diego, CA). Samples with equivocal results were retested using the Aptima CT single assay (Hologic Inc) and for NG with a quantitative polymerase chain reaction targeting opa genes.17 Urine samples were tested for MG using transcription-mediated amplification (TMA) assays (Aptima, Hologic Inc). From all samples that tested positive for MG in the MG-TMA assay, DNA was extracted with isopropanol precipitation and subsequently tested for macrolide resistance using the MG-MRAM quantitative polymerase chain reaction to detect wild-type (MG-WT) or any mutations (MRAM) in the 23S rRNA gene at nucleotide positions 2058 and 2059 (Escherichia coli numbering).18Mycoplasma genitalium and MRAM testing were done for study purposes only, and results were disclosed neither to the men nor to the healthcare professionals. A subset of samples was tested for Trichomonas vaginalis (TV) using TMA assays (Aptima, Hologic Inc).
Text MessageMen diagnosed with urethritis at initial consultation were informed about and asked to respond to an online survey sent to them by text message 2 weeks later. The text message was sent in Dutch and English. The question was, “How are the physical complaints that caused you to visit our clinic?” The answer options provided were as follows: “I did not have physical complaints,” “The physical complaints are gone,” “I'm doing better,” “The same, not improved,” and “I'm doing worse.”
Statistical AnalysisOnly men with an initial consultation for urethritis were included in the analysis. Sociodemographic data, sexual behavior, the presence of clinical symptoms, recent antibiotic treatment, and antibiotics prescribed for the current case were extracted from electronic patient files. The variable “Education” was categorized into low (no education, primary school, lower secondary vocational education and intermediate secondary general education), mid (higher secondary general education, senior secondary vocational education, and preuniversity secondary education), and high (higher professional or university education). In the analysis, the answers “The physical complaints are gone” and “I'm doing better” were combined into one category, “improvement”; the answers “The same, not improved” and “I'm doing worse” were combined into one category, “no improvement.” We performed an additional analysis with a more stricter definition of clinical improvement: (1) the physical complaints are gone and (2) still having physical complaints (combining the other 3 answers in one category). The following men with urethritis were considered evaluable for clinical improvement analysis: men who indicated to have symptoms at the time of the consultation; who were tested for NG, CT, and MG; who were informed about the text message; who responded within 28 days after treatment; and of whom text message data were recorded. Treatments that were considered in analysis were treatments given up to 2 days before the completion of the online questionnaire regarding clinical improvement; several patients have received additional treatment after that time point. Univariable logistic regression analysis using generalized estimating equation was performed to compare the characteristics and infections of evaluable and nonevaluable cases and to compare cases indicating improvement to those reporting no improvement. Factors associated with clinical improvement were examined using generalized estimating equation logistic regression analysis. Variables included a priori in multivariable analysis were NG, CT, MG genotype, and age; variables with P < 0.20 in univariable analysis were considered in multivariable analysis, but only retained if P < 0.05. Significance was assessed 2-sided for all variables, applying a cutoff value of P < 0.05. Data were analyzed using Stata Intercooled 15 (StataCorp LLC, College Station, TX).
Ethics StatementMen of the STI outpatient clinic Amsterdam were informed of the “opt-out” system regarding research on remnants of patient material. All data were pseudonymized before analysis. The study protocol was evaluated by the Medical Ethics Committee of the Academic Medical Center in Amsterdam (W18.013#18.024) and deemed not to require a full review of the board; signed informed consent was not deemed to be required.
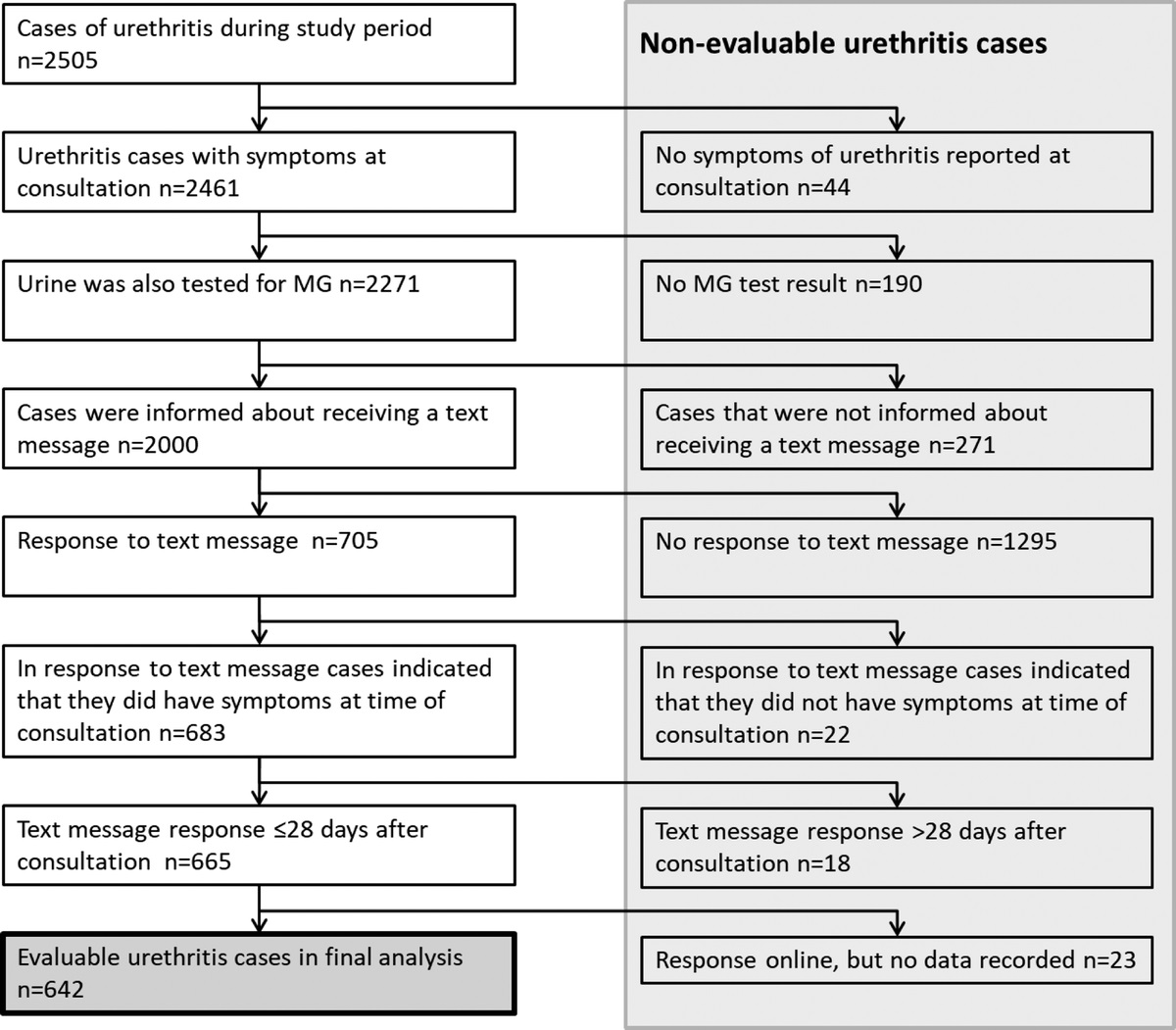
RESULTS Characteristics and Infection Status of All Urethritis CasesWe registered 2505 cases of urethritis in 2095 men in the study period (Fig. 1 and Supplementary Table 1, https://links.lww.com/OLQ/A781). Mean (SD) age was 31.2 (10.4) years. The majority of cases were men who have sex with men (53%), most were of Dutch origin (41%) and had a high education level (63%), and 12% of the cases were HIV positive. Neisseria gonorrhoeae, CT, and MG test results were available from 2288 urethritis cases. In 768 (34%) cases, none of the 3 microorganisms were detected (Table 1). Neisseria gonorrhoeae, CT and MG were detected in, respectively, 26%, 29%, and 23% of urethritis cases. Mycoplasma genitalium MRAM genotyping was successful in 439 of 522 MG positives (84%). Macrolide resistance-associated mutation was detected in 74% (327 of 439) of the successful MG-MRAM genotyped cases. Single infections were detected in 18% for NG, 21% for CT, and 14% for MG. Dual infections occurred in 4% for each pathogen combination and a triple infection in 1% of the urethritis cases (Table 1).
 Figure 1:
Figure 1: Flowchart of men included in the study. In the study period 2505 urethritis cases in 2095 men were observed. In the final analysis, data of 642 cases of 593 men were included, who were tested for Neisseria gonorrhoeae (NG), Chlamydia trachomatis (CT), Mycoplasma genitalium (MG) and responded within 28 days to the text message. N, number of urethritis cases.
TABLE 1 - Infection Status (Single, Dual, or Triple) of Urethritis Cases, by Evaluation Status and Reported Improvement, STI Clinic in Amsterdam, May 2018 to November 2019 NG CT MG Total, n (%) Evaluable*, n (%) No Improvement in Evaluable Cases†, n (%) − − − 768 (34) 208 (27) 48 (23) + − − 417 (18) 120 (29) 8 (7) − + − 486 (21) 155 (32) 24 (15) − − + 320 (14) 87 (27) 33 (38) + + − 95 (4) 14 (15) 1 (7) + − + 93 (4) 32 (34) 3 (9) − + + 81 (4) 18 (22) 7 (39) + + + 28 (1) 8 (29) 3 (38) Total 2288 642 (28) 127 (20)*χ2 Test was used to determine overall significance between evaluable and nonevaluable cases, P = 0.028.
†χ2 Test was used to determine overall significance between cases reporting improvement and no improvement, P < 0.001.
CT indicates Chlamydia trachomatis; MG, Mycoplasma genitalium; NG, Neisseria gonorrhoeae; STI, sexually transmitted infection.
In 642 (25.6%) cases, clinical improvement after empirical treatment could be evaluated (Fig. 1). Evaluable cases were older (mean age, 32.7 vs. 30.7 years; P < 0.001), were more often men who have sex with men (P = 0.002), were more often of Dutch origin (P = 0.042), and reported less often to have had urethritis symptoms in the past 2 years (P = 0.037) compared with nonevaluable cases (Supplementary Table 1, https://links.lww.com/OLQ/A781). Infection rates did not differ between evaluable and nonevaluable cases (Supplementary Table 1, https://links.lww.com/OLQ/A781).
Reported Clinical Improvement of Urethritis After Empirical TreatmentOne hundred twenty-seven of the 642 evaluable cases (20%) indicated that their symptoms had not improved (Table 2). Patients infected with MG-MRAM had an OR of 3.38 (95% CI, 2.11–5.40) for no improvement 2 weeks after therapy, compared with patients not infected with MG. This association remained after adjusting for CT and NG coinfection, age, ethnicity, and text-message response delay (not immediately responding to the text message but on days 15–28; adjusted odds ratio [aOR], 3.58; 95% CI, 2.05–6.24). Treatments with ceftriaxone and azithromycin were considered in the multivariable model but were both not significant. In the analysis in which we used a more stricter definition of clinical improvement, similar results were found (Supplementary Table 2, https://links.lww.com/OLQ/A781), except for ethnicity and CT infections, but these factors did not have a major effect on the association between MG-MRAM and clinical improvement. We performed a separate analysis for all NGU cases in which patients with MG-MRAM had a similar OR of 3.44 (95% CI, 2.04–5.80) for no improvement compared with patients with NGU not infected by MG (Supplementary Table 3, https://links.lww.com/OLQ/A781).
TABLE 2 - Clinical Improvement by Characteristics of 642 Evaluable Cases With Urethritis, STI Clinic in Amsterdam, May 2018 to November 2019 No. Cases Without Clinical Improvement as a Fraction of Evaluable Cases P OR 95% CI aOR* 95% CI Total 127/642 (20%) Age in years, n (%) <25 43/176 (24%) 0.065 1 25–34 53/247 (21%) 0.79 0.50–1.27 35–44 19/109 (17%) 0.72 0.39–1.32 ≥45 12/110 (11%) 0.39 0.19–0.78 Age per 10 y, mean (SD) Mean age of 33 (11) y in cases with clinical improvement vs. mean age of 30 (10) y in cases without clinical improvement 0.012 0.77 0.63–0.93 0.83 0.66–1.05 Sexual risk group, n (%) MSW 66/263 (25%) 0.008 1 MSM 61/379 (16%) 0.58 0.39–0.87 Country of origin, n (%) The Netherlands 49/296 (17%) <0.001 1 1 Turkey, Morocco, North Africa 5/48 (10%) 0.60 0.22–1.60 0.51 0.19–1.36 Suriname 38/90 (42%) 3.66 2.14–6.26 3.38 1.91–6.00 Europe, outside the Netherlands 12/86 (14%) 0.86 0.43–1.71 0.73 0.36–1.47 Other 23/122 (19%) 1.20 0.68–2.09 1.02 0.56–1.87 Educational level†, n (%) Low 11/56 (20%) 0.280 1 Medium 39/152 (26%) 1.20 0.57–2.50 High 68/391 (17%) 0.82 0.41–1.64 Urethritis symptoms past 2 y, n (%) No 87/446 (20%) 0.893 1 Yes 40/196 (20%) 1.03 0.66–1.60 Antibiotic use previous, n (%) None 103/525 (20%) 0.591 1 Last 7 d 2/14 (14%) 0.72 0.17–3.00 Last 14–21 d 1/14 (7%) 0.39 0.08–1.91 Last 30 d 6/29 (21%) 1.32 0.61–2.87 Last 90 d 15/60 (25%) 1.30 0.69–2.44 Text message response in days, n (%) 14 68/395 (17%) 0.048 1 1 15–28 59/247 (24%) 1.48 1.00–2.18 1.60 1.04–2.44 HIV, n (%) Negative 93/425 (22%) 0.104 1 Positive 11/94 (12%) 0.47 0.23–0.95 Unknown 23/123 (19%) 0.84 0.51–1.38 No. sex partners in the last 6 mo‡, n (%) 0 or 1 10/54 (19%) 0.397 1 2–4 56/241 (23%) 1.33 0.66–2.69 5–9 32/173 (18%) 0.93 0.44–1.95 ≥10 29/172 (17%) 0.90 0.43–1.92 Received azithromycin, n (%) No 22/192 (11%) 0.001 1 Yes 105/450 (23%) 2.52 1.44–4.39 Received doxycycline, n (%) No 118/586 (20%) 0.152 1 Yes 9/56 (16%) 0.55 0.25–1.24 Received ceftriaxone, n (%) No 110/467 (24%) <0.001 1 Yes 17/175 (10%) 0.36 0.21–0.63 NG, n (%) Negative 112/468 (24%) <0.001 1 1 Positive 15/174 (9%) 0.32 0.18–0.56 0.28 0.15–0.52 CT, n (%) Negative 92/447 (21%) 0.517 1 1 Positive 35/195 (18%) 0.87 0.56–1.33 0.67 0.40–1.11 MG, n (%) Negative 81/497 (16%) <0.001 1 Positive 46/145 (32%) 2.20 1.41–3.45 MG genotype, n (%) Negative for MG 81/497 (16%) <0.001 1 1 WT 4/28 (14%) 0.59 0.12–2.90 0.58 0.17–2.05 MRAM 38/94 (40%) 3.38 2.11–5.40 3.58 2.05–6.24 Unknown 4/23 (17%) 1.16 0.44–3.07 1.10 0.35–3.50Univariable and multivariable logistic regression with GEE was used to determine risk factors for no improvement.
*All variables with P < 0.20 were considered for the multivariable model; in the final model, the following variables were included: MG genotype, CT, NG, age, country of origin, response in days.
†Data missing from 43 patients.
‡Data missing from 2 patients. In the final model, 642 patients were included.
aOR indicates adjusted odds ratio; GEE, generalized estimating equation; MG, Mycoplasma genitalium; MRAM, macrolide resistance-associated mutations; MSM, men who have sex with men; MSW, men who have sex with women only; NG, Neisseria gonorrhoeae; OR, odds ratio; STI, sexually transmitted infection; WT, wild-type.
We additionally analyzed improvement considering single, dual, and triple infections (Fig. 2). Few patients with single NG infection, or with dual infections of NG + CT or NG + MG reported no clinical improvement (7%–9%; Table 1 and Supplementary Fig. 1, https://links.lww.com/OLQ/A782). Patients infected with single MG, dual CT + MG, or triple NG + CT + MG infection most often reported no improvement of symptoms (37%–39%). In a subanalysis on all cases with an MG infection, cases with MG-MRAM had an OR of 4.00 (95% CI, 1.27–12.58) for no improvement 2 weeks after therapy compared with cases with MG-WT. After adjusting for CT and NG coinfection, age, and text-message response delay, the aOR for patients with MG-MRAM was 5.86 (95% CI, 1.88–18.3) compared with MG-WT.
 Figure 2:
Figure 2: Reported improvement of evaluable cases, by infection status (single, dual, or triple), STI clinic in Amsterdam, May 2018 to November 2019. Percentages above the bars indicate the proportion of evaluable cases without improvement. Overall χ2 test, P < 0.001. STI, sexually transmitted infection; NG, Neisseria gonorrhoeae; CT, Chlamydia trachomatis; MG, Mycoplasma genitalium.
Men of Surinamese origin significantly more often reported no clinical improvement (42% [38 of 90]) compared with men of Dutch origin (17% [49 of 296]; P < 0.001). Surinamese men had an OR of 3.66 (95% CI, 2.14–6.26) of no clinical improvement compared with men of Dutch origin, and this remained similar after adjusting for CT and NG coinfection, age, and text-message response delay (aOR, 3.38; 95% CI, 1.91–6.00). We subdivided the infection status and MG genotype by country of origin (Supplementary Table 4, https://links.lww.com/OLQ/A781) and found a significant difference in infection status between the different counties of origin. Surinamese men have relatively less often NG infections, but more MG infections and also more coinfections. This is not significantly different from other ethnicities, however. In a subset of 55 of 90 Surinamese men, we found that only one man was infected with TV, not explaining the high number of men reporting no clinical improvement.
Antibiotic Treatment and Clinical ImprovementThe majority of patients received only antibiotic treatment during their initial consultation (575 of 642 [90%]). Patients who reattended the clinic after empirical treatment did this with an median of 7 days (range, 2–14 days). Patients were asked to reattend the clinic in case of additional diagnostic findings on specimens taken at entry visit. Fifty-five patients received additional treatment at reattendance: 18 patients received ceftriaxone, 10 patients received azithromycin, 26 patients received doxycycline, and 1 patient received benzathine benzylpenicillin. Treatments that were considered in analysis were treatments given up to 2 days before the completion of the online questionnaire regarding clinical improvement. From all evaluable cases with an NG monoinfection, 98 of 120 (82%) had been treated with ceftriaxone alone, and 7% (7 of 98) indicated that their symptoms had not improved (Table 3). From the evaluable cases with a CT monoinfection, 131 of 155 (85%) were treated with azithromycin alone, and 17% (22 of 131) indicated no improvement. Evaluable cases with an MG monoinfection were treated with azithromycin alone in 81 of 87 of the cases (93%), and 40% (32 of 81) indicated that their symptoms had not improved (Table 3). Cases that were infected with MG-MRAM (monoinfection and coinfection) and that were treated with azithromycin indicated no improvement in 46% (33 of 71), whereas cases infected with MG-WT who were treated with azithromycin indicated no improvement in 15% (4 of 26; P = 0.005).
TABLE 3 - Treatment Given and Reported Improvement of Evaluable Urethritis Cases, by Infection Status (None, Single, Dual, or Triple), STI Clinic in Amsterdam, May 2018 to November 2019 Treatment Infections No NG, CT or MG, n (%) NG Only, n (%) CT Only, n (%) MG Only, n (%) NG + CT, n (%) NG + MG, n (%) CT + MG, n (%) NG + CT + MG, n (%) Total, n (%) Azithromycin 39/175 (22) 0/1 (0) 22/131 (17) 32/81 (40) 0/1 (0) 0/2 (0) 5/13 (38) 0/1 (0) 98/405 (24) Ceftriaxone 1/3 (33) 7/98 (7) 0 0 1/3 (33) 2/25 (8) 0 2/4 (50) 13/133 (10) Doxycycline 4/13 (31) 0/1 (0) 1/6 (17) 0/1 (0) 0/2 (0) 0 1/1 (100) 0 6/24 (25)
留言 (0)