
記住我
In this triple blinded randomized controlled trial(i.e.the participants,the data analyzer and researchers taking measurements was blinded). 34 elderly people with LBP were recruited as volunteers. This sample was divided into two groups (intervention and control) by random lists. Random grouping was performed using SPSS 20.0 software (fixed value: 20190727). The study protocol was approved by the ethics committee of the First Affiliated Hospital of Sun Yat-sen University in Guangzhou, China. It was done in accordance with the Declaration of Helsinki, good clinical practices, and applicable laws and regulations, and it meets standards of the CONSORT guidelines (approval number#2019469). Written informed consent was obtained from all participants before the experiment.
ParticipantsThe calculation of statistical power was performed a priori using G Power Software. We estimated the sample size according to the number of two basic averages. According to previous research [17], the balance data of the experimental group were selected as the effect index. With a power analysis set power of 0.80, effect size of 0.75 [18], and 10% loss rate, 12 participants were required for each group.
Participants with LBP were recruited after responding to a recruitment advertisement that was launched through the local community and different activity centers for the elderly. Then they came to the First Affiliated Hospital of Sun Yat-sen University and were diagnosed by a physician specialized in physical medicine and rehabilitation (physiatrist) .
The inclusion criteria were as follows: (1) age ≥ 60 years; (2) nonspecific LBP for at least 3 months in the last year; (3) a Mini-Mental State Examination (MMSE) score > 24 (out of 30) and Montreal Cognitive Assessment (MoCA) score > 26 (out of 30); and (5) Pain score on the visual analog scale (VAS) ≥ 3 (out of 10). Participants with LBP were excluded from the study if any of the following exclusion criteria were met: (1) a history of spinal surgery, rheumatological diseases of the spine, severe spinal pathologies or deformities, or spinal tumors; (2) a history of recent low-extremity injury, endocrine or neuromuscular disease, arthritis or orthopedic disease, orthostatic hypotension, vision problems, vestibular system disease, or any other physical injury that might affect balance; and (3) the use of psychoactive or antihypertensive drugs (antidepressants, antipsychotics, sedatives/hypnotics, antiepileptics, or antiparkinsonian drugs).
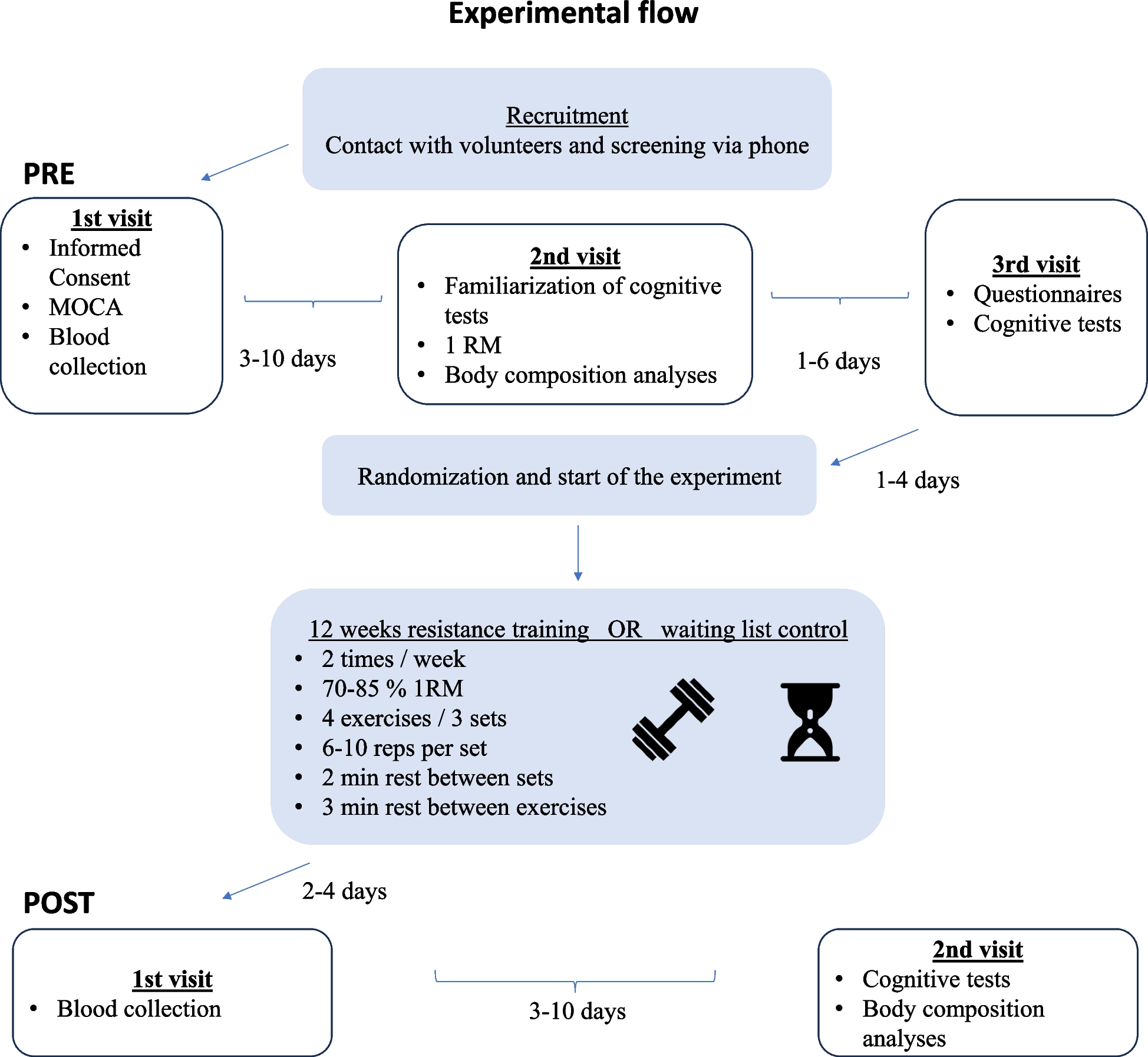
ProceduresThe protocol of the present study is showed in Fig. 1.
Fig. 1
Flowchart showing participate screening and the experimental protocol
Basic evaluations (sociodemographic evaluation, MMSE, MoCA, VAS, ODI)The experiment was conducted in bright light in a safe and quiet physiotherapy room. At the beginning, sociodemographic information of each participant was recorded in an individual information sheet. Weight, height, and body mass index (BMI) were also assessed. MMSE and MoCA scale was used to assess the cognitive function. The 10-cm VAS and Oswestry Disability Index (ODI) were used to assess the pain-related clinical outcomes. The whole experiment took approximately 30 min.
Pain-related clinical outcomesPain intensity was measured by a VAS (0 = no pain, 10 = pain as bad as it could be). The Oswestry disability questionnaire (0 = no disability, 100 = totally disabled) was filled out by the participants. Pain and disability were measured before and after the training [19].
ODIThe ODI is commonly used in clinical trials to measure the functional status of participants with LBP [20]. It is comprised of 10 dimensions, with 6 levels being set in each dimension. Specifically, a score of 0 represents the lowest disability level, while 5 indicates the highest disability level. Moreover, the total score is converted into percentage, with a consequent maximum of 100% [21].
Congitive function (MoCA and MMSE)The MMSE and MoCA are both global cognitive screening measures with the same range of scores (0–30), the two tests emphasize different aspects of cognition. The MMSE is a 30-question assessment of cognitive function that evaluates attention and orientation, memory, registration, recall, calculation, language and the ability to draw a complex polygon [22]. The MoCA has six cognitive domains: short-term memory, visuospatial abilities, executive functions, attention and working memory, language, and orientation to time and space. The score range is 0 to 30; the threshold for normal cognitive function is ≧26 [23].
Ultrasound imaging measurementUltrasound imaging measurement was conducted before and after the training using SonixGPS ultrasound (SonixTablet, Ultrasonix, Canada) with a 15-MHz linear transducer. To standardize the technique, a supine crook-lying position (hips flexed to approximately 135°, knees flexed to 90°) was adopted by all of the participants [24]. And the evaluations were taken by the same researcher. The transducer was positioned at just above the iliac crest in the midaxillary line. Following a deep inspiration and then a forced expiration, participants were asked to continue to breathe out (further expiration). Images were collected during this period. TrA muscle thickness was measured as the distance between the superior and inferior hyperechoic muscle fascias, at the middle of the ultrasound image (Fig. 2). The ultrasound imaging measurement was repeated three times, and the mean values of were used for data analysis.
Fig. 2 Mobility functions (TUG, 10 M-WT and FSST)
Mobility functions (TUG, 10 M-WT and FSST)All the participants completed 3 assessments for mobility functions, which involved the timed up-and-go (TUG) test, 10-m walking test (10 M-WT), and four-square step test (FSST).
The TUG test required the participant to start with standing up from a chair without handles and then walking 3 m as quickly as possible. After that, the participant turned around an obstacle, walked back, and finally sat down on a chair.
In the 10 M-WT test, participants were instructed to walk at their self-perceived comfortable pace. The time to complete 10-m walking was recorded using a stopwatch [25].
The FSST included four squares, and the participant was required to start in the first square (facing the second square) and step over a cane to enter each additional square while moving in a clockwise direction. They then moved in the counter clockwise direction as quickly as possible without touching the canes (Fig. 3). The trials were repeat if the participant’s foot touched the canes.
Fig. 3
In the three dynamic balance tests, participants could have one or two practice trials before each test. Each test was repeated three times and were assigned randomly to the participants. The completion time were recorded during the experiment, and the mean values were used in the following analysis.
InterventionsAll study personnel were trained and certified to implement study protocols in an effort to ensure standardization within and across sites. The intervention period was 4 weeks. Exercise therapists were trained to deliver exercises and physiotherapy.
Core stability groupParticipants in the training group (TG) received core stability training (25-30 min) + physiotherapy (40 min).
Participants underwent intervention for 4 weeks (4 sessions per week, 65–70 min each session) .
The education session was performed at the clinic by a trained doctor at the first visit. Moreover, a printed pamphlet with instructions on how to perform the exercises was given to each participant.
Abdominal respiration skills are learned before the intervention, the exercise movements selected in this study were mainly focus on abdominal muscles such as TrA [14]. Exercises were designed 4 sets, two static exercises (Fig. 4, A and B) and two dynamic exercises (Fig. 4, C and D), from 8 to 10 repetitions and contractions from 10 s to 20 s. Rest intervals were set as 10 s between the sets and 2 mins between the exercises. Core muscle stability training for intervention group included:
1.crawl position exercise (Fig. 4, A)
2.the quadruped exercise with yoga blocks (Fig. 4, B)
3.abdomen exercise with swiss ball in supine position (Fig. 4, C)
4.abdomen exercise with resistance band in supine position (Fig. 4, D)
Fig. 4
Image of training. Core stabilization exercises: (A). crawl position exercise, (B). the quadruped exercise with yoga blocks, (C). abdomen exercise with swiss ball in supine position (D). abdomen exercise with resistance band in supine position
The physiotherapy treatment included interference wave and magnetic resonance thermal therapy. Two pairs of interference wave electrodes (SK-9SDX, MINATO, Japan) intersected with each other around the painful point of back for 20 min. For magnetic resonance thermal therapy (magneto-vibration heat treatment (LGT-2600B, China), the participants were positioned in a supine position, the foldable electrodes were placed in the participant’s waist pain site, setting mode 1(vibration therapeutic apparatus:50–120 beats/s, temperature:40–58 °C), underwent for 20 min. The training for the TG took about 1 h. There were 4 weeks of training at 4 times per week.
CG groupParticipants in the CG received physiotherapy that included interference wave + magnetic resonance thermal therapy for a total of 40 min every time at 4 times a week for 4 weeks.
Statistical analysisDifferences in demographic variables between groups were tested using an independent t-test. Two-way repeated-measures ANOVA was conducted to analyze the data from the ultrasound imaging measurement, VAS, ODI, and dynamic balance tests. The effect size for the statistical analysis was reflected by ƞ2p. The value of low effect size, moderate effect size and high effect size was 0.04, 0.25 and 0.64 [26]. The between-subject factor was the group (TG or CG), and the within-subject factor was time (pre-experiment and post-experiment). Greenhouse-Geisser correction was used when Mauchly’s test of sphericity was violated. Post hoc pairwise comparisons with Bonferroni adjustment were applied when significant interaction effects were observed. The thickness change of Tra was selected to explore the associations between the change of mobility functions. The significance level was set at P < 0.05 for all statistical tests. All data were analyzed using the software SPSS 20.0.
留言 (0)