
記住我



Congenital syphilis, a life-threatening infection caused by the transmission of Treponema pallidum from a woman to her fetus during pregnancy, can result in miscarriage, stillbirth, preterm birth, low birth weight, and infant death.1 Whereas many infants with congenital syphilis are asymptomatic at birth,2 classic signs can appear in the first 2 years of life, including rash, copious nasal discharge (“snuffles”), hepatosplenomegaly, jaundice related to syphilitic hepatitis, bone deformities, and neurologic involvement. Although these sequelae can be prevented when maternal syphilis is diagnosed and treated 30 days or more before delivery,3 the incidence of congenital syphilis in the United States is increasing.2
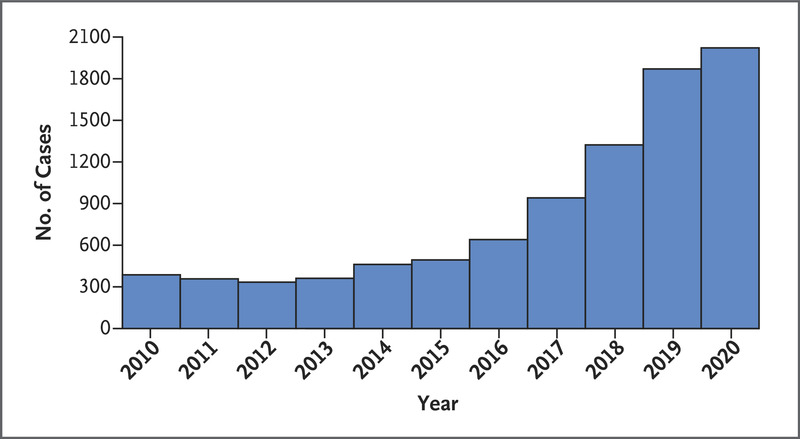
Figure 1. Figure 1. Reported Cases of Congenital Syphilis among U.S. Infants Born 2010–2020.
Figure 1. Reported Cases of Congenital Syphilis among U.S. Infants Born 2010–2020. The case counts for congenital syphilis for 2010–2019 were previously published in the 2019 STD Surveillance Report.2 The case counts for 2020 include cases reported to Centers for Disease Control and Prevention as of July 29, 2021. The reporting period for 2020 cases ends in October 2021.
Congenital syphilis is a reportable condition in all 50 states and the District of Columbia and is nationally notifiable (surveillance criteria for case notification are summarized in the Supplementary Appendix, available with the full text of this letter at NEJM.org). As of July 29, 2021, a total of 2022 infants born in 2020 had been reported to the Centers for Disease Control and Prevention (CDC) as having congenital syphilis (Figure 1). This number already surpasses the 1870 cases reported in 2019, represents the highest case count since 1994, and is likely to continue to rise until the reporting period ends in October 2021. Forty-seven states and the District of Columbia reported at least 1 case of congenital syphilis in 2020, with 32 states and the District of Columbia already reporting case increases over 2019. Of the 2022 cases currently reported, 139 (6.9%) involved death related to congenital syphilis.
The increases in the case counts of congenital syphilis predate the coronavirus disease 2019 (Covid-19) pandemic and have persisted during pandemic-related disruptions of health care and public health systems. Recent increases reflect increases in untreated syphilis among women and their male sex partners. Syphilis — once concentrated in urban areas and the U.S. South — has dispersed geographically. In 2010, a total of 846 U.S. counties (27%) reported at least one case of syphilis in a woman of reproductive age; by 2019, the number of counties had grown to 1568 (50%). The resurgence of syphilis among women and its spread to previously unaffected areas underscore the fact that congenital syphilis can occur anywhere.
Stopping community transmission of syphilis is the most effective way to prevent congenital syphilis; however, identification and treatment of syphilis in pregnant women remain invaluable for preventing infant death and disability. The CDC recommends universal screening for syphilis at the first prenatal visit, with repeat screening at 28 weeks of gestation and at delivery for women who live in areas with high morbidity or who are at increased individual risk.
The implementation of strategies that reduce perinatal transmission of the human immunodeficiency virus (HIV) — including the prevention of infection in women, increased prenatal testing, and advances in maternal treatment — has been associated with a decline in annual cases of perinatal HIV from an estimated 1760 in 1991 to fewer than 40 in 2019.4,5 A similar commitment of resources could reduce or eliminate congenital syphilis.
Virginia B. Bowen, Ph.D., M.H.S.
Robert McDonald, M.D., M.P.H.
Jeremy A. Grey, Ph.D.
Anne Kimball, M.D., M.P.H.
Elizabeth A. Torrone, Ph.D., M.S.P.H.
Centers for Disease Control and Prevention, Atlanta, GA
[email protected]
Disclosure forms provided by the authors are available with the full text of this letter at NEJM.org.
5 References1. Cooper JM, Sánchez PJ. Congenital syphilis. Semin Perinatol 2018;42:176-184.
2. Centers for Disease Control and Prevention. Sexually transmitted disease surveillance 2019. Atlanta: Department of Health and Human Services, 2021 (https://www.cdc.gov/std/statistics/2019/default.htm).
3. Workowski KA, Bolan GA. Sexually transmitted diseases treatment guidelines, 2015. MMWR Recomm Rep 2015;64:RR-3:1-137.
4. Nesheim SR, Wiener J, Fitz Harris LF, Lampe MA, Weidle PJ. Brief report: estimated incidence of perinatally acquired HIV infection in the United States, 1978–2013. J Acquir Immune Defic Syndr 2017;76:461-464.
5. Centers for Disease Control and Prevention. HIV surveillance report, 2019. Atlanta: Department of Health and Human Services, May 2021 (http://www.cdc.gov/hiv/library/reports/hiv-surveillance.html).
留言 (0)