This study used Cox and Cure regressions to identify factors associated with the survival of Iranian patients with COVID-19. It was the first time that mixture cure regression was applied for survival analysis of Iranian patients suffering from COVID-19. According to the Incidence part of this model, older ages, respiratory distress, hypertension, diabetes, CVDs, cough, and fever reduced the odds of cure, whereas the latency part of this model indicated that older ages, respiratory distress, hypertension, and CVD increased the hazard rate. In agreement to mixture cure, Cox regression identified that older ages, respiratory distress, history of CVDs, and hypertension were associated with higher hazard rates.
In line with the findings of this study, a review study reported that having comorbid diseases, such as obesity, diabetes and high blood pressure in patients with COVID-19 worsens the patients’ conditions. Worsening of patients’ condition can damage important organs of the body, such as the heart, liver, and kidney [24].
Few studies across the world have been performed to determine factors associated with the survival of COVID-19 patients using the mixture cure model. A study applied this model on Indian patients and showed that patients’ age was associated with odds of cure, which was in accordance with the results of our study [25]. Undoubtedly, identification of factors related to the cure and severity of the disease can effectively contribute to effective patient management and provide care for patients who display these risk factors in order to increase the rate of cure and survival.
Several studies on the survival of COVID-19 patients all around the world showed that a number of factors, such as older age, muscle pain, pneumonia, sore throat, impaired renal function, increased C-reactive protein, leukocytosis, heart damage, hyperglycemia, and high-dose corticosteroids use were associated with increased risk of COVID-19-related death [21, 26, 27]. Besides, patients with high blood pressure may experience more severe conditions with a higher risk of death compared to non-hypertensive patients [28]. In Iran, studies on COVID-19 survival have shown that diabetes, hypertension, CVDs, BMI > 35, lung cancer, chronic kidney disease, and immunodeficiency have been associated with increased odds of death due to COVID-19 [29]. In another study conducted in Iran, the prevalence of anemia in admitted COVID-19 patients was high and these conditions of anemia were associated with mortality, ventilator requirement, and the risk of ICU admission [30]. In a national study in Iran on 62,955 patients in 1034 hospitals between 20 February and 20 April 2020, the cumulative risk of death in hospitals was reported as 24.4% [31]. Differences in disease mortality rates in various parts of the world can be due to differences in patients, admission criteria, clinical characteristics of patients, as well as patients’ access to treatment and specialized care at admission and specific country conditions.
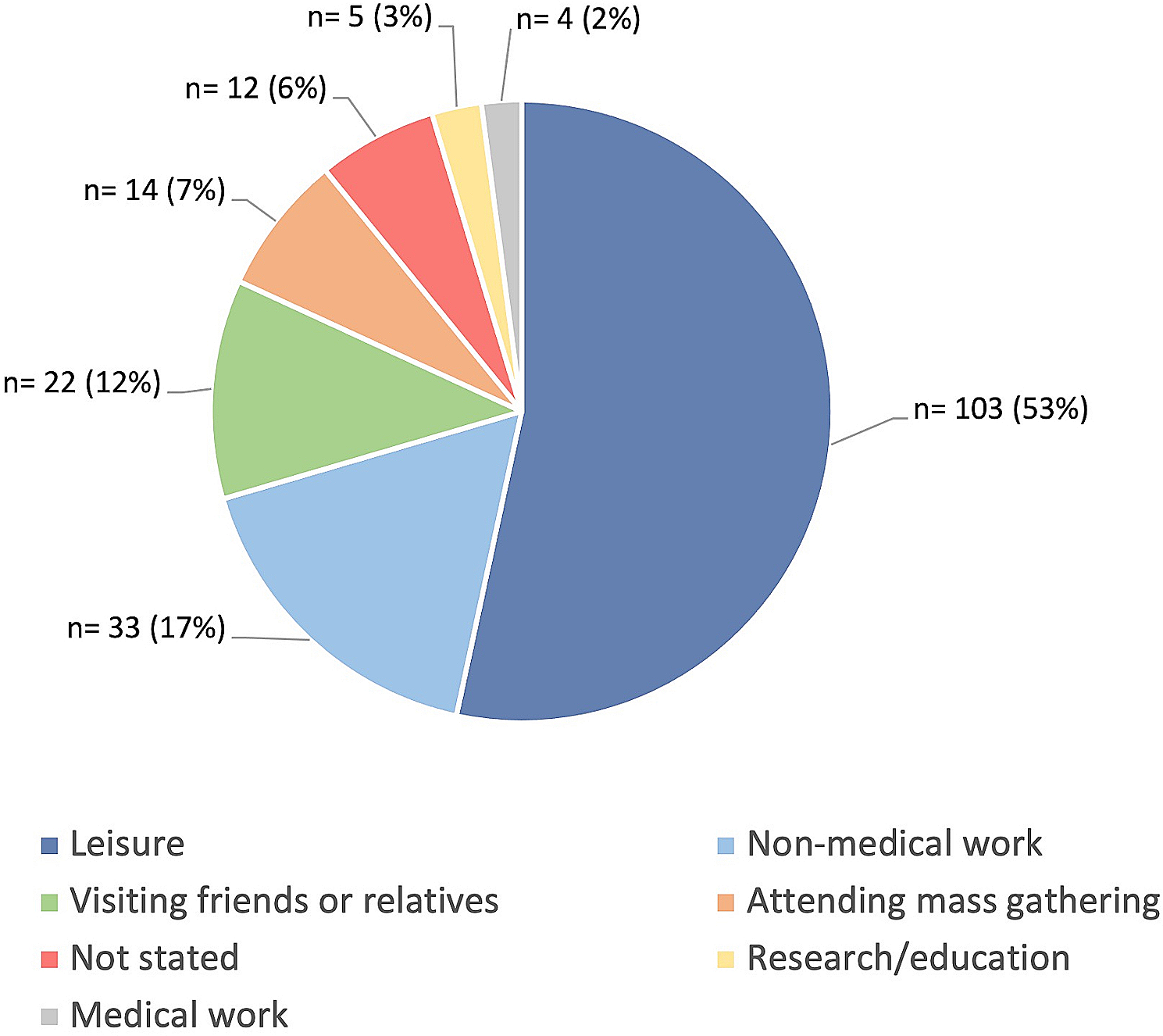
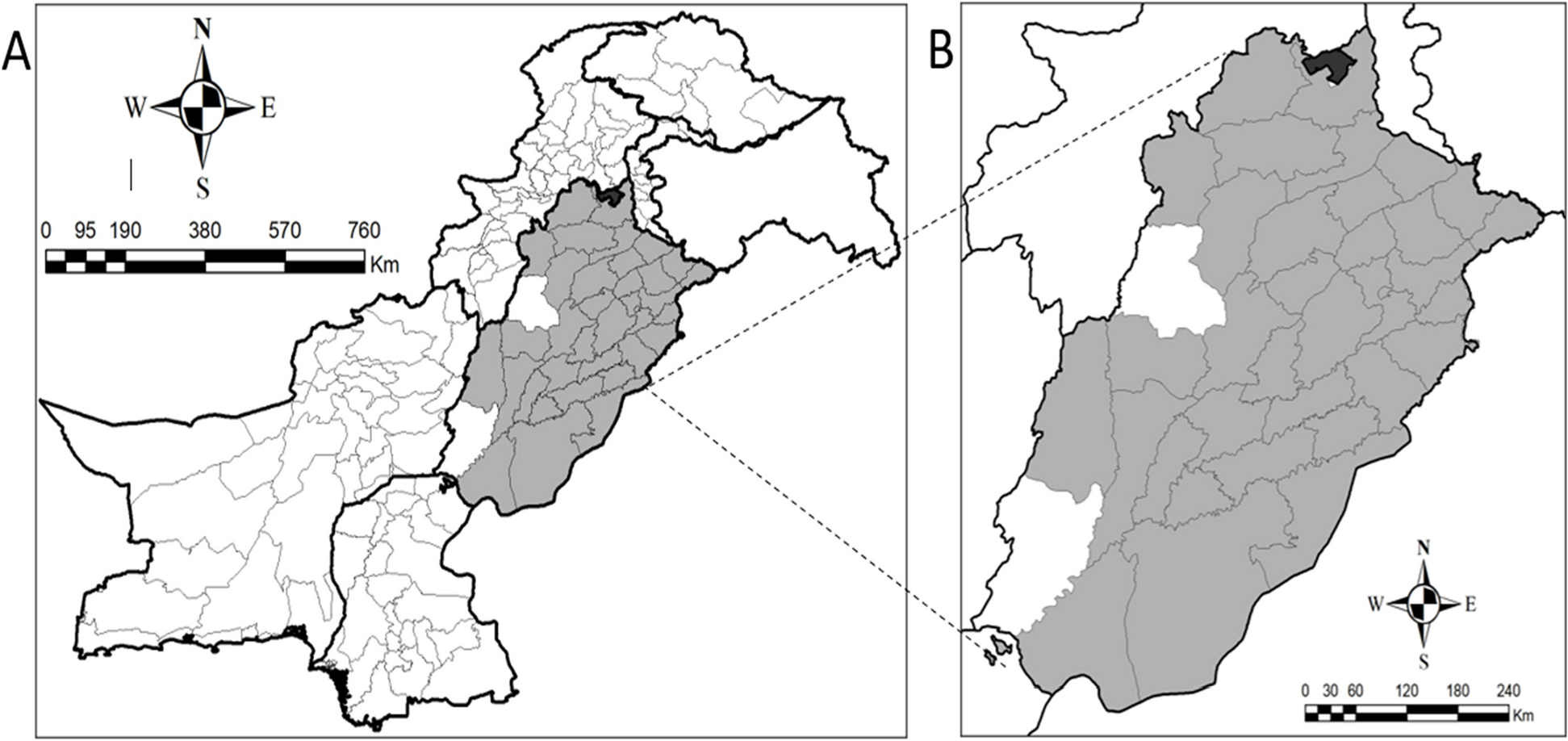
The findings of this study showed a shorter overall length of hospital stay in Iran, compared to other countries. The median length of hospital stay in Iran was 5 days, while it was reported as 21 days in Vietnam, 6.9 days in France, and 13.8 days in Ghana [32,33,34]. Also, age, area of living, and source of infection were significantly associated with the length of hospital stay. Global studies have shown that the time from the exposure to onset of symptoms, onset of symptoms to hospital admission, and conditions and characteristics of countries were significantly associated with the length of hospital stay [32,33,34]. This difference in hospitalization duration in different parts of the world can be attributed to different criteria for admission and discharge and pandemic conditions of the disease across various countries [19]. The shorter length of hospital stay among patients in this study can be due to two major factors such as clinical indices and post-discharge facilities. Clinical indices define as the patient’s clinical condition at the time of admission and patient discharge conditions, which include not having clear shortness of breath, improvement in patient’s CT scan results and reduction of inflammatory factors. Facilities which are provided by Fasa University of Medical Sciences, such as transfer from hospital to a convalescent home, having patient care conditions at home, oxygen supply, home isolation and Telemedicine home care program constitute the post-discharge facilities.
In most survival studies, the most important assumption is that if the duration of the follow-up period is long enough, all subjects will experience the desirable event. But in some cases, such as patients with COVID-19, a significant proportion of people do not experience the event (death) even after a long follow-up, and these patients are considered immune. Under these conditions, mixture cure models are used as an effective statistical method [35, 36]. In our study, the cure rate is 81.5% and a significant percentage of patients were censored. As a result, the common Cox Regression models are less effective than the mixture cure models.
Finally, it should be noted that the AIC of mixture cure model was much smaller than its counterpart, Cox regression, indicating more goodness of fit for cure model. Additionally, the mixture cure model not only recognized all significant variables in Cox regression, but also identified more risk factors that were reported in previous studies. Therefore, it could be claimed that the mixture cure model provided a better fit and identified more variables related to the survival of COVID-19 patients.
Limitations and strengths of the study
The assessed variables in this study were extracted from the hospitalized patients’ records in the syndromic surveillance system, and no more variables were available. On the other hand, high-quality patients’ information records, without any missing data, were mentioned as the study strength.



留言 (0)