
記住我



According to the “Law of the People's Republic of China on the Prevention and Treatment of Infectious Diseases,”1 infectious diseases are grouped into 3 classes: class A, class B, and class C. Class A infectious diseases, including plague and cholera, are severe infectious diseases that require mandatory management. Class B infectious diseases mainly include severe acute respiratory syndrome (SARS), AIDS, viral hepatitis, and other strictly managed infectious diseases. Class C infectious diseases include epidemic hemorrhagic parotid gland rash, acute hemorrhagic mucositis, leprosy, and so on. Some class B diseases, such as SARS, pulmonary anthrax, and highly pathogenic avian influenza, may be addressed and treated as class A diseases, given their special characteristics such as transmission mode or mortality. Novel coronavirus disease 2019 (COVID-19) is an infectious disease that is mainly spread via the respiratory tract. It is thought to cause severe and harmful consequences for individuals and society. Thus, based on the “Law of the People's Republic of China on the Prevention and Treatment of Infectious Diseases,” COVID-19 is classified as class B infectious disease but managed as a class A infectious disease; class A diseases, namely, sudden, new, or severe infectious diseases, are managed with patient quarantine, treatment, and medical observation of close contacts (tracking) in China.
The prevalence of COVID-19 has become widespread, but there are few reports on nursing care of infants with suspected/confirmed COVID-19. Because of their immature immune systems, infants are more susceptible to community- and/or hospital-acquired infections, and there may be vertical transmission during pregnancy or delivery by mothers with confirmed or suspected COVID-19.2 The clinical manifestations of newborns, especially preterm infants, may be unremarkable and nonspecific, requiring careful observation.3 Our hospital is located in Wuhan City, Hubei Province. It is a tertiary class A comprehensive hospital that includes the Main Hospital Area, Optical Valley Branch, and Sino-French New City Branch. All of these facilities have been designated special treatment centers for COVID-19 in Hubei. From January 23, 2020, to March 23, 2020, a total of 26 infants born to mothers with suspected/confirmed COVID-19 were admitted to our neonatal intensive care unit (NICU). Our clinical nursing care experience is outlined here to provide a reference for other medical institutions.
PATIENT INFORMATIONThe case data of infants admitted to the NICU of the Main Hospital Area and Sino-French New City Branch from January 23, 2020, to March 23, 2020, were analyzed. All 26 infants were delivered by women with suspected/confirmed COVID-19.
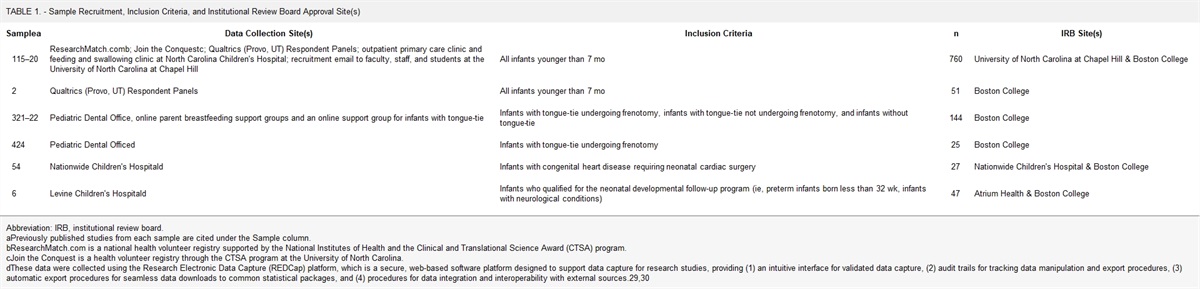
Among the 26 pregnant women with suspected/confirmed COVID-19, 8 patients had only fever; the highest temperature was 38.8°C. Three patients had only cough; 1 patient had fever accompanied by cough; 1 patient had fever accompanied by diarrhea; 1 patient had fever, cough, and wheezing; 1 patient had fever, cough, wheezing, and dyspnea; and 3 patients had none of the aforementioned symptoms. Lung computed tomographic scans of 18 patients indicated suspicious viral pneumonia, and pharyngeal swab of 14 patients were positive for SARS-CoV-2 nucleic acids. Additional information is shown in Table 1.
TABLE 1. - Demographic Information of Pregnant Women Cases Basic Information Qiaokou Main HospitalAbbreviations: IEL, intraepithelial lymphocyte; IgG, immunoglobulin G; IgM, immunoglobulin M; Spo2, saturation of peripheral oxygen; WBC, white blood cell.
The 26 newborns included 20 full-term infants and 6 premature infants, with gestational ages ranging from 28 5/7 to 41 2/7 weeks. Their Apgar scores were 7 to 8 at 1 minute or 8 to 9 at 5 minutes. They had no fever, cough, or respiratory symptoms. Two premature infants were treated with continuous positive airway pressure (CPAP) due to shortness of breath, nasal flaring, and retraction.
ROUTINE PRACTICES FORMULATED FOR INFECTION PREVENTION AND CONTROLBased on the transmission characteristics and clinical manifestations of COVID-19 as well as the 2019 new coronavirus infection prevention and control guidelines and literature, a series of routine clinical practices were formulated by our group to prevent and control infections in the NICU. Our routine practices included 4 components: (1) setting up isolation wards; (2) conducting isolation protection and control measures; (3) hand hygiene; and (4) disinfection.
Setting Up Isolation WardsBefore the outbreak of COVID-19, children admitted to the NICU of our hospital were all considered noninfectious infants. In accordance with the expert consensus issued by the Neonatal Pediatrician Branch of the Chinese Medical Doctor Association,4 infants born to mothers with suspected/confirmed COVID-19 were transferred to a neonatal isolation observation ward or an isolation observation ward/isolation diagnosis and treatment ward for disease management.
Therefore, based on the actual situation of our hospital and the regulations outlined in the expert consensus mentioned earlier, isolation NICUs were established in the Main Hospital Area and Sino-French New City Branch. The following outlines the establishment of the NICU isolation ward.
An isolation observation ward was set up in the Main Hospital Area for isolation, observation, and care of newborns with suspected COVID-19 infection who were in a stable condition after birth. The Sino-French New City Branch was identified as a COVID-19–designated hospital and thus the Sino-French New City Branch established an isolation observation ward area and isolation diagnosis and treatment ward area for the admission and treatment of infants born to mothers with suspected/confirmed COVID-19.
Isolation Prevention and Control MeasuresCOVID-19 in infants can be transmitted via close contact or droplets (from caregivers, family members, family visitors) and can be hospital-acquired or community-acquired.5 Therefore, we took strict disinfection and isolation measures for prevention and control.
We chose to place infants in incubators, with bedside quarantine measures. Infants were not placed on an open infrared radiation platform (radiant warmer) during their care in the NICU.3 During general diagnosis and treatment of infants, secondary protection,6 namely, medical protective masks, work clothes, isolation clothing and/or medical protective clothing, shoe covers, gloves, work caps, and goggles or protective masks, were worn when necessary. During treatment and operations that were prone to generate aerosols, such as sputum suctioning or throat swab sampling, tertiary protection was worn.7 Tertiary protection was the same as secondary protection with the addition of positive pressure headgear or a full-scale respirator.7 Diagnosis and treatment procedures, such as blood sampling or fluid infusion, were centralized and completed simultaneously by the medial staff to minimize contact with the infants.
Hand HygieneHand hygiene for the prevention and control of viral infection includes hand washing and hand disinfection. Antibacterial hand sanitizer was used for hand washing and disinfection. Chlorhexidine has been reported to have no effect on the virus.7 Under special conditions, such as contact with a patient highly suspected of having COVID-19, 3% hydrogen peroxide disinfectant or 0.05% chlorine disinfectant was used to wipe or soak the hands.8
Disinfection TreatmentCombined with relevant Chinese laws and regulations,8–11 the regulation of “New Coronavirus Pneumonia Prevention and Control Measures and Procedures in Tongji Hospital” was formulated; some of the measures are as follows.
In crowded places, we opened doors or windows to increase ventilation. When suspected/confirmed patients were present, the use of air-conditioning and ventilation systems was forbidden.12 Daily air disinfection was carried out. In occupied rooms, we opened the windows at least twice a day for 30 minutes each time. Unoccupied rooms were irradiated with ultraviolet light once a day for 1 hour or longer each time. Patient rooms were disinfected by one of the following procedures. Ultraviolet light was initially used to irradiate the room for 1 hour and then a solution of 3% hydrogen peroxide or 5000 mg/L peracetic acid or 500 mg/L chlorine dioxide in an ultra-low-volume sprayer (20-30 mL/m3) was sprayed for 2 hours. The doors and windows were closed during disinfection, and the room was fully ventilated after disinfection. Alternatively, ultraviolet light was initially used to irradiate the room for 1 hour and then peracetic acid (1 g/m3) was used for heating and fumigation. The doors and windows were closed before disinfection and opened for thorough ventilation after disinfection.8
The domestic waste of children was treated as infectious waste. Since COVID-19 can be isolated from feces and urine, exposure to aerosols or contact with feces or urine in the environment was addressed.6 Thus, we transport disposable diapers to a temporary storage room for medical waste, sprayed them with 1000 mg/L chlorine-containing disinfectant for at least 10 minutes, discarded them into a yellow garbage bag and sealed them. During the handover, 1000 mg/L chlorine-containing disinfectant was sprayed on the outside of the yellow garbage bag, then an additional yellow garbage bag was added, and finally the plastic bag was wrapped tightly.9–11,13
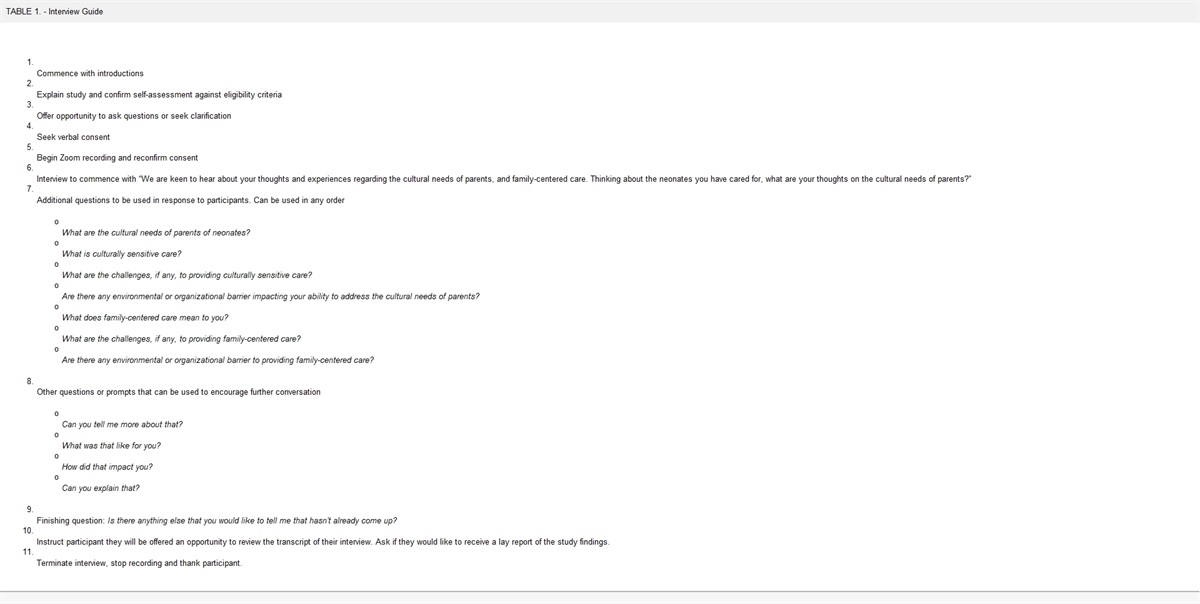
NURSING CAREConsidering the main clinical manifestations of SARS-CoV-2 infection, nursing intervention measures in our hospital were formulated.
Body Temperature Monitoring and NursingThe newborns were placed in an incubator to keep their body temperature within the normal temperature range of 36.5°C to 37.5°C. The temperature monitoring mode was changed from rectal temperature monitoring to continuous skin temperature monitoring to reduce the transmission of the virus by fecal contact.8
During hospitalization of the 26 infants, 2 infants had a fever during phototherapy, with body temperatures of 38.2°C and 38.5°C, respectively. Since infection indicators, such as blood C-reactive protein, were within the normal range, the fevers were considered “false fevers” caused by phototherapy.14 The body temperature of the patients returned to within the normal range within half an hour of decreasing the temperature of the incubator by 0.5°C. There was no evidence of fever in other infants.
Respiratory Symptom Monitoring and NursingRespiratory symptoms are typical manifestations of COVID-19. Some of the infants had atypical symptoms, such as lethargy and labored breathing.8 Following admission, the respiratory rate and blood oxygen saturation of the 26 infants were monitored for 24 hours using electrocardiogram monitors. The infants were placed in different positions, and the physiological body positions were continuously supported and promoted to keep the respiratory tract unobstructed and maintain effective breathing.14
Early chest radiographs in 2 infants showed small patchy shadows, which were considered to be related to amniotic fluid inhalation. One premature infant showed decreased Spo2 (saturation of peripheral oxygen) while feeding; the Spo2 recovered spontaneously after feeding was stopped, and no respiratory support was necessary. Two preterm infants (31 and 2857) weeks, respectively) received continuous CPAP-assisted ventilation at 24 hours of age due to shortness of breath, progressive dyspnea, nasal alar flaring, 3-concave inhalation sign, and decreased blood oxygen saturation, which were related to immature respiratory center development and newborn respiratory distress syndrome. No shortness of breath, cyanosis of the lips or face, respiratory retraction, or breathing difficulty was observed in the other infants.
When CPAP-assisted ventilation was administered, prone positioning was used to improve lung ventilation in 2 premature infants. After lung auscultation, suctioning was performed in the premature infants. Since their respiratory secretions were thick and viscous, they were given aerosolized Mucosolvan (Ambroxol) 15 mg and Pulmicort (Budesonide) 0.5 mg and received chest percussion. The CPAP treatment times in the 2 preterm infants were 72 and 510 hours, respectively, and no invasive ventilation was used. However, when the invasive ventilator was used to aspirate sputum from the infants, tertiary protection was applied. Inline closed-system suctioning was used to reduce the interruption of ventilation and prevent the ejection of sputum from the airway, thereby minimizing the chance of infection.5
Skin CareGenerally, the infants were removed from their incubators and given a bath when their condition stabilized. In this study, the incubator was used as a barrier, so all 26 newborns were given sponge baths in the incubator. It has been reported that infants with COVID-19 present with gastrointestinal symptoms such as vomiting and diarrhea.8 Diarrhea was not observed in the 26 infants in this study. When providing buttock skin care for infants, absorbent and soft diapers were used and changed at least every 3 hours to keep the buttock skin clean and dry.
Nutrition and FeedingThe World Health Organization recommends that infants born to mothers with suspected, possible, or confirmed COVID-19 should be fed in accordance with the Standard Infant Feeding Guidelines, while necessary preventive infection control measures should be taken.15 The US Centers for Disease Control and Prevention recommend that mothers with confirmed COVID-19 should temporarily separate themselves from their infants16; after performing hand hygiene and while wearing a face mask, they should express human milk using a dedicated breast pump. In contrast, in our hospital, mother's own milk is not recommended for infants of mothers with suspected or confirmed infections and active confirmed cases; rather, pasteurized, donated human milk is used for feeding. The 26 infants were fed formula during hospitalization. Based on the severity of disease, different feeding initiation times and feeding methods were selected. Twenty-four infants received initial feeding immediately after admission, and 2 premature infants treated with CPAP received delayed initial feedings; the infants were fed orally at the 26th hour and 7th day after admission, respectively. When feeding the infants, it was necessary to be patient to observe whether the infants showed milk spilling or choking and whether they experienced vomiting or diarrhea. During the hospitalization of the 26 newborns, there was no vomiting, diarrhea, or evidence of feeding intolerance.
Family SupportDuring the COVID-19 epidemic, visits to the neonatal ward were suspended. If conditions permitted, family members could visit the infants only after uniform monitoring and investigation by the hospital, and only family members with negative nucleic acid test results could enter the hospital for visitation.4 These measures also resulted in limited interaction and contact between parents and infants during the hospitalization period. Telephone consultations and medical notifications were provided to the parents. A WeChat parent group for the infants in this study was established to answer questions, provide guidance, and notify parents of follow-up visits. In addition, the application of cloud video-based family support during the epidemic was explored. After coordinating with the information department of the hospital and establishing a temporary communication network, the parents of the infants could observe the condition of their children in the hospital in real time by using the WeChat app on their mobile phones. Individualized and effective family support strategies were provided to relieve parents' psychological stress and anxiety caused by COVID-19 and mother–infant separation.
Discharge ManagementThe discharge standards were as follows: body temperature within the normal range for more than 3 days with no signs of respiratory distress; significant improvements in respiratory symptoms; significant improvement in acute exudative lesions on pulmonary imaging; and 2 consecutive negative SARS-CoV-2 nucleic acid tests from respiratory tract samples, with a sampling interval of at least 1 day. When the criteria were met, the infants could be removed from isolation and discharged.8
Discharge EducationZeng and colleagues17,18 reported 2 cases of SARS-CoV-2 infections in infants who were aged 17 and 19 days, respectively. This suggests that the infants were exposed to the infection through close family contact. Therefore, attention should be given to the home-based care of infants and the management of COVID-19 by family caregivers to prevent horizontal transmission. We recommended that caregivers measure body temperature twice a day and wear a face mask. In addition, windows should be opened at least twice a day for 30 minutes to maintain air circulation in the room. Hands should be carefully washed before and after contacting infants. Infants need to keep warm, and their body temperature should be checked twice a day. Infants should have sufficient rest and be fed carefully. If infants have a fever, cough, shortness of breath, lethargy, poor feeding, or diarrhea, they should be taken to the hospital immediately.
Follow-up and OutcomesNucleic acid testing of throat swabs, anal swabs, urine, and blood was carried out in 26 infants at 24 hours, 7 days, and 14 days after admission to our hospital. One infant had a positive viral nucleic acid test result at 36 hours after birth. However, the same sample was rechecked by the laboratory, and the results were negative; thus, the former test was considered a false-positive. The other 25 infants had negative viral nucleic acid test results. During isolation, the vital signs of all 26 infants remained stable, their general condition was good, and no complications occurred. The medical staff performed care in strict accordance with the infection control measures as outlined earlier, and no SARS-CoV-2 infection occurred among infants or medical staff during infant admission.
Twenty-five of the newborns (one infant remained in the hospital) returned to the neonatal follow-up clinic for follow-up at approximately 1 month after discharge. Follow-up consisted of physical examination (neonatal behavioral neurological assessment; hearing screening; body length, weight, and head circumference measurements; etc), nucleic acid testing and antibody testing for COVID-19, routine blood examination, and blood biochemical examination.
The “+” notes that nucleic acid antibody testing can be used as an auxiliary diagnosis of COVID-19.8 Positivity for IgM antibody indicates a recent acute infection, and a positivity for IgG antibody indicates previous infection. A test result of 10.0 AU/mL is considered reactive (positive), and a lower result is considered negative.19 The follow-up results showed that 4 newborns were IgG+, IgM− and 21 newborns were IgG−, IgM−. Four newborns (3 full-term and 1 premature) developed physiological anemia, and their parents were instructed to provide iron supplementation. The infants' physical development and nervous system assessments were normal.
DISCUSSIONThe “2019 Expert Advice on Infection Prevention and Control of COVID-19 for the Neonatology Department” specifies that a neonatal isolation ward or isolation observation area/isolation diagnosis and treatment area should meet the requirements for single-patient isolation rooms.4 During the epidemic period, many infants needed to be isolated for observation or diagnosis and treatment, and it was difficult for most medical institutions to meet the single-room isolation requirements.20 Respiratory droplet transmission is the main route of transmission of SARS-CoV-2, and infants are very susceptible to exposure if contaminated droplets produced by coughing or sneezing by infected patients are inhaled at a close range.20 In view of the fact that neonatal pneumonia is usually not accompanied by coughing, the infant incubator is a relatively closed and isolated space with an inherent barrier. Moreover, the existing evidence does not indicate that infants born to mothers with suspected/confirmed COVID-19 will become infected. Therefore, in our department, the infants who were in generally good condition and were born to mothers with suspected COVID-19 were housed and treated in the same isolation room. All newborns were placed in infant incubators, the distance between the incubators was increased to 1.5 m, and the bedsides were well isolated. A separate isolation gown was placed next to each newborn's incubator. When contacting infants, the nursing staff wore isolation gowns outside of a protective suit, changed their gloves, and used rapid hand sanitizer for hand hygiene. No SARS-CoV-2 infection occurred in the 26 infants or medical staff during nursing care. Therefore, we recommended that infants born to mothers with suspected/confirmed COVID-19 should be housed in a single-patient room in an infant incubator for isolation observation and/or treatment; the bed space should be increased, and each bedside should be isolated.
In terms of levels of protection, some have proposed that the secondary protection should be worn when caring for infants born to mothers with suspected/confirmed COVID-19.6 It has also been suggested that infants born to mothers with confirmed COVID-19 should be separated from their mothers immediately after birth, and isolation (first level of protection) and medical observation should be performed.20
Generalized mother-to-child transmission routes include intrauterine vertical transmission, contact with maternal blood and amniotic fluid during childbirth, and close postnatal contact, especially during breastfeeding. Specialized mother-to-child transmission refers to only intrauterine vertical transmission. Recent studies have shown that COVID-19 is not transmitted vertically from mother to child.21,22 Our infant team conducted nucleic acid testing of human milk, gastric juice, umbilical cord blood, throat swabs, feces, and urine of the infants immediately after birth. The results showed that all the samples were negative, which does not support the hypothesis of specialized mother-to-child transmission of SARS-CoV-2. The results of this study were similar to those of Zhu et al23 and Chen et al,24 who recently published the clinical outcomes of infants born to mothers with COVID-19. Two studies published online by the Journal of the American Medical Association (JAMA) suggested the possibility of mother-to-child transmission,25,26 but there was also an analysis suggesting that the results of these two studies should be further analyzed. Recently, a French research team published a case report in Nature Communications.27 Through detailed inspection and careful verification, it was confirmed that SARS-CoV-2 could be transmitted from mother to child through the placenta. However, such cases are very rare. Because the number of cases analyzed in related studies was limited and the study period was short, more samples and longer follow-up times are needed to confirm the existence of vertical transmission. We consider that environmental contamination by suspected/confirmed COVID-19 patients during the delivery process and contact transmission by medical staff were the main routes of neonatal transmission. “Environmental contamination” is a term that refers to all the ways in which humans contaminate their surroundings. Shared objects are capable of transmitting the virus via indirect transmission. Therefore, our concept paid more attention to secondary protection when first contacting and caring for infants born to mothers with suspected/confirmed COVID-19.
CONCLUSIONDuring the COVID-19 epidemic, medical staff should strictly follow infection control measures while performing infant care. Increased attention should be given to secondary protection measures when contacting infants born to mothers with suspected/confirmed COVID-19. In addition, because the study was conducted at the early stage of the epidemic, the experimental design was not perfect, and the anxiety state of the infant's parents before and after treatment was not measured. In future research, relevant evaluation tools should be used to measure changes in the stress and anxiety states of parents and to verify the feasibility and reliability of family support programs.
What we know:COVID-19 is classified as class B legal infectious disease for management by the National Health Committee; the prevention and control measures for class A infectious diseases should be adapted.
Because of the immature immune system, neonates are susceptible to community- and/or hospital-acquired infections due to vertical transmission during pregnancy and delivery in confirmed and suspected cases with COVID-19.
What needs to be studied:Further large-scale studies of the neonates delivered by pregnant women with suspected/confirmed SARS-COV-2 infection are needed to check whether they can be placed in one room for isolation observation and/or treatment.
Further large-scale studies are needed to compare the incidence of nosocomial infection rate, using secondary protection when first contacting and caring for the neonates or in the whole medical process.
What can we do today:The nursing intervention measures based on the neonatal nursing routine combined with the main clinical manifestations of SARSCoV-2 infection are effective for these cases.
Hand hygiene, including hand washing and hand disinfection, should be emphasized in the prevention and control of virus infection.
Neonates should be placed in the incubator with the bedside quarantine measures.
Close the humidification function of air-conditioning and ventilation systems.
留言 (0)