
記住我

Treatment with topical corticosteroids is commonly utilized by clinicians in the treatment of olfactory loss, irrespective of the etiology. The literature supportive of the use of topical corticosteroids is largely extrapolated from the treatment of CRS-related olfactory dysfunction [8••, 9, 10]. Although studies showing benefit to olfaction from topical corticosteroids in non-CRS-related olfactory loss are limited, the risk for this intervention is low and may be considered as monotherapy or as an adjunct with other treatment (e.g., olfactory training) with appropriate patient counseling [11•].
Systemic CorticosteroidsSystemic corticosteroids can also be effective in treating olfactory loss in CRS with nasal polyps. The patient’s response to this systemic treatment may also help distinguish an inflammatory etiology from other causes. The mechanism underlying the benefit is thought to be related to reduction of inflammatory mediators, but recent research has also shown that olfactory gene expression may also be influenced by this systemic therapy [12].
As the precise biological mechanism remains a topic of active research, several clinical studies have demonstrated benefit in olfaction after systemic corticosteroids using objective measures, beyond what would be expected from spontaneous recovery [13]. However, these studies are heterogeneous in etiology and often lack a control group, thereby limiting the generalizability. Additional studies have also sought to evaluate the potential additive effect of adjunctive treatments, particularly along with zinc in traumatic loss and with vitamin B supplementation [14, 15]. These studies have demonstrated that there may be additive benefit to olfactory function using these additional treatments, beyond corticosteroid monotherapy alone.
Clinicians who elect to offer patients treatment with systemic corticosteroids should have a thorough discussion the potential adverse effects of this therapy given the lack of sound evidence. Additional studies are needed to better determine the effective dose and duration of this treatment as well as the interactive effects of adjunctive treatments.
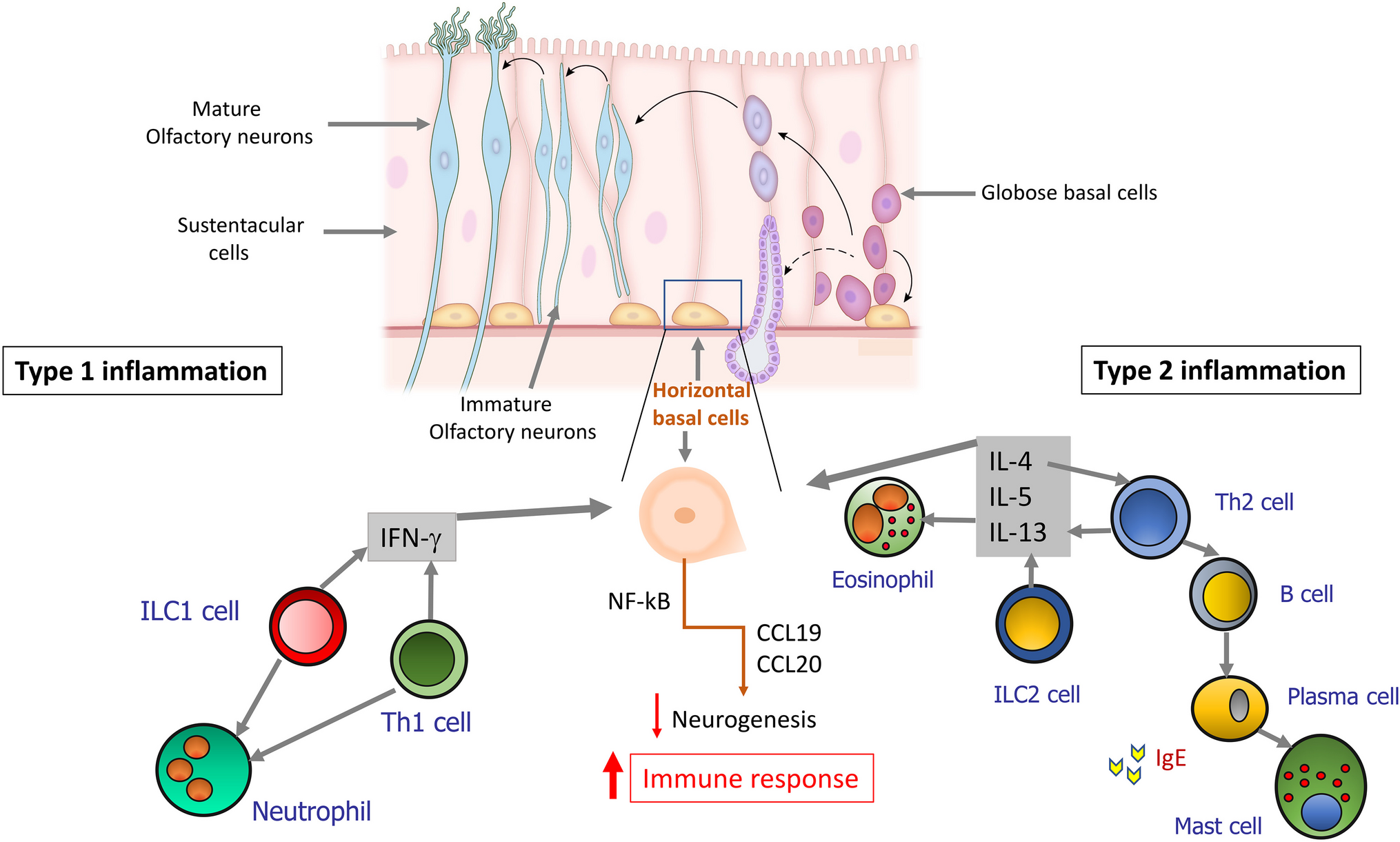
BiologicsBiologics are an emerging treatment in CRS with nasal polyps and refer to a class of drugs that target the immune pathway underlies this inflammatory disease. These drugs consist of monoclonal antibodies which target the key effectors of type 2 inflammation. For example, omalizumab is a medication targeted against IgE, a mast cell activator. Although this medication has been shown to be effective in decreasing polyp scores and improving quality of life, its impact on olfaction is not clear and only small studies exist. Pinto et al. conducted a study of 14 patients, 7 in each arm, where olfactory testing (UPSIT) did not show a significant difference between groups [16]. Similarly, mepolizumab (Anti IL-5) is designed to disrupt the maturation and recruitment of eosinophils; however, the effect of this medication on olfaction is not well studied. Dupilumab is a monoclonal antibody to the IL 4 receptor alpha subunit, which is shared with IL-13. This drug inhibits the cytokine signaling central to type 2-mediated inflammation. Bachert et al. demonstrated an improvement in olfaction (UPSIT) in the dupilumab group compared to controls following treatment [17]. Most recently, in a pooled analysis by Mullol et al., dupilumab was shown to provide a rapid and sustained improvement in olfaction, as measured by UPSIT [18]. Thus, dupilumab has the most evidence for improvement in olfaction in patients with CRS with nasal polyps to date.
Intranasal Calcium BuffersAs calcium ions within mucus may have an inhibitory role in olfactory signaling, calcium buffers (e.g., sodium citrate) have emerged as an intuitive method to treat olfactory loss. In recent years, Whitcroft and colleagues showed clinical improvement after a single topical administration of sodium citrate in patients with post-infectious smell loss, including a prospective single-blinded, placebo-controlled trial [19, 20]. This was followed by a subsequent double-blinded study evaluating this same treatment in a more diverse etiologic cohort [21]. Although the benefit was transient, it could provide patients with episodes of olfactory improvement during critical times such as during meals. This therapy has a compelling mechanistic basis and future clinical research could be helpful to discern the durability of benefit and range of benefit based on degree of olfactory loss.
Phosphodiesterase InhibitorsPhosphodiesterase inhibitors (PDI) prevent the degradation of intracellular cyclic adenosine monophosphate (cAMP) and cyclic guanosine monophosphate (cGMP), thereby increasing levels of these molecules within olfactory epithelial cells. Theoretically, this would lead to a more efficient signal transduction cascade to the olfactory bulb. However, clinical results from PDI inhibitors (e.g., theophylline, sildenafil, caffeine, and pentoxifylline) have been mixed. Theophylline is the most widely studied PDI, with initial reports by Henkin et al. reported subjective improvement in approximately half of patients with olfactory loss with oral treatment, although a proper controlled study was lacking [22]. Given the potential for adverse systemic effects (e.g., restlessness, gastrointestinal discomfort, and sleep disturbance), topical intranasal administration was also studied and reported to be effective in some patients [23, 24].
The literature with regard to other PDIs, however, is less promising and raises questions regarding the presumed biological basis. For instance, a recent double-blind placebo-controlled study of a single administration of caffeine (65 mg) had no effect on olfactory function, and similarly, a study of 6 patients with post-traumatic hyposmia treated with penoxifylline also showed no olfactory benefit [25, 26]. Overall, the benefit for PDI treatment has yet to be established given the lack of control arm, etiologic heterogeneity, and data derived mostly from subjective assessments rather than validated instruments.
OtherSeveral other therapies have recently been investigated in the treatment of olfactory loss. Supplementation with alpha-lipoic acid, vitamin A, omega-3, and treatment with intranasal insulin has been studied with mixed results. The rationale for these treatments is their presumed neuroregenerative potential and anti-oxidant properties. Oral administration of alpha-lipoic acid (600 mg/day) was studied in 23 patients and approximately 60% experienced an improvement in olfaction on objective assessments [27]. Furthermore, in 2017, Hummel et al. found that those patients undergoing treatment with topical, intranasal vitamin A used in conjunction with olfactory training showed significant benefit to odor discrimination compared to those who did not [28]. Additionally, Yan et al. conducted a multi-institutional, prospective, randomized controlled trial of 110 patients undergoing transsphenoidal surgery in 2019 and found that treatment with omega-3 demonstrated led to less persistent olfactory loss compared to controls [29]. Also, a pilot study of intranasal administration of insulin demonstrated improved odor sensitivity, and a more recent randomized-controlled trial improved odor identification and overall olfactory function among 38 patients with hyposmia [30, 31]. Overall, the utility of these treatments is yet to be proven in larger trials with etiologic diversity in olfactory loss beyond spontaneous improvements, which can be up to 35% in some forms of smell loss [32].
Procedural InterventionsOlfactory TrainingThere is substantial evidence to suggest that olfactory training is effective in the treatment of olfactory loss. This treatment was first described by Hummel et al. in 2009 in a prospective controlled study of 24 patients with diverse etiologies for olfactory loss. In the described paradigm, patients underwent repeated exposures to four odors (i.e., rose, eucalyptus, clove, and lemon) twice daily for 3 months and olfactory function was assessed using Sniffin’ Sticks [33]. There was significant benefit in olfactory function from this intervention.
The rationale for this treatment is that repetitive stimulation of the olfactory system could enhance regenerative capacity and/or allow for proper neuron survival and targeting during recovery. Subsequent studies have elaborated on this paradigm, with variations on the treatment duration, odor concentrations, and with change in odorants after every 3 months with some additional benefit. However, other groups have suggested that the benefit from olfactory training may be similar to spontaneous recovery [34,35,36,37]. Further research would be helpful to determine the benefit of this intervention beyond that of spontaneous recovery and with more specific inclusion criteria (i.e., etiologic homogeneity) and standardized treatment durations. Based on the available current evidence, we routinely recommend olfactory training in symptomatic cases of olfactory loss which has been persistent, including following COVID-19 infection. The olfactory training paradigm adopted by the authors is included as Fig. 1.
Fig. 1
Olfactory Training Paradigm, adopted by the authors (adapted from Altundag et al. [30]) Caption: A set of four odorants as described below are selected every three months for olfactory training. Each odorant is smelled for 15 seconds, with a 10 second rest between odorants. The set of odorants are smelled twice daily
Recent research has focused on the neurobiological basis of the effect and whether the effects are central (cortical) or at the level of the sensory epithelium. In 2018, Hummel et al. showed that electro-olfactogram (EOG) recordings from olfactory epithelium were higher in patients after OT, supporting the presumed effect on neuronal signaling and plasticity [38•]. More recently, Al Aïn et al. showed increased cortical thickness in olfactory processing areas of the brain after 6 weeks of olfactory training [39]. Further neuroimaging studies of patients with post-traumatic olfactory loss undergoing OT have suggested that the benefit in this group could be due to functional cortical changes rather than enhancements at the sensory epithelium [40, 41]. It is entirely possible that both central and peripheral processes are impacted by this intervention, but further studies are needed to better understand the underlying biological changes.
AcupunctureTraditional Chinese Acupuncture (TCA) has been used for centuries as treatment for a variety of medical conditions. This technique was studied by Dai et al. in 50 patients with post-viral olfactory loss refractory to various conventional treatments (oral steroids, vitamin B, olfactory training, or intranasal steroids) [42]. After 3 months of three-times weekly TCA, 11 of 25 patients in the treatment group reported improved olfactory function of at least 4 points on the University of Pennsylvania Smell Identification Test, whereas 4 of 25 reported improvement in the no treatment group (p = 0.031). Similar to other interventions, patients with shorter symptom duration, and those with hyposmia rather than total smell loss tended to be more likely to improve. Another study of 15 patients with post-viral olfactory loss showed that those who underwent once-weekly TCA for 10 weeks were more likely to improve their olfactory function compared to those who received vitamin B (53.3% vs. 13.3%, respectively) [43].
SurgeryOne of the cardinal symptoms of chronic rhinosinusitis is olfactory dysfunction and is present in a substantial portion of affected patients. The etiology of this dysfunction may be related to physical obstruction of odorants reaching the olfactory cleft (i.e., conductive loss) and/or inflammatory mediators affecting the functioning of the neuro-epithelium. There is considerable evidence that endoscopic sinus surgery benefits olfaction [44], presumably by controlling the underlying disease process through ventilation of the paranasal sinuses and facilitation of topical therapies. This improvement may be even more apparent and likely in patients who undergo concomitant septoplasty, have obstructive nasal polyps, and have more severe baseline olfactory dysfunction [45•]. This literature, however, is heterogenous in terms of the measures used to assess olfaction (i.e., subjective, odor-identification, or odor-threshold).
In addition to surgery for chronic rhinosinusitis, nasal surgery including septoplasty and septorhinoplasty has also been studied as interventions which may improve olfaction by facilitating airflow and topical delivery to the olfactory cleft. However, this data is mixed, with a recent study indicating that there are no beneficial effects while others have demonstrated favorable responses. The literature related to septorhinoplasty is more limited, but early results suggest a modest benefit to olfactory function [46, 47]. It is important to note that these interventions also carry inherent risk for olfactory impairment due to iatrogentic injury related to trauma or scarring of the olfactory cleft, or surgical disruption of the olfactory system during endoscopic skull base surgery.
Occasionally, patients with olfactory disorders including significant parosmias or phantosmias unresponsive to medical therapies and with significant impact on quality of life may be considered for surgical removal of the olfactory epithelium. This has been shown in several small series to be effective in resolving phantosmia symptoms [48–50]. However, the risks associated with this intervention should be carefully considered against the potential benefits. Specifically, given that olfactory disturbances may be the sign of recovery and may improve with treatment. This procedure should be considered only after careful evaluation and selection by a surgeon with experience in olfactory disorders at a facility equipped to manage the possible complications (e.g., cerebrospinal fluid leak).
Emerging TreatmentsCommensurate with advancements in our understanding of the biological basis of olfactory loss, novel therapeutic options have also recently emerged.
Researchers have recently studied the use of N-acetylcysteine (100 mg/kg twice daily) after acute olfactory neuronal injury in animal models with promising results [51]. These researchers found a neuroprotective effect with this treatment, with significantly fewer olfactory neurons undergoing apoptosis in the group undergoing the treatment. Given the potential protective effects of this medication on a molecular level, there is some promise that this therapy could also provide clinical benefit to olfaction in humans, perhaps after head trauma.
The inherent regenerative capacity of the olfactory epithelium offers a compelling therapeutic target for treatment. Yan et al. recently reported the use of platelet-rich-plasma (PRP), which is derived from the patient’s blood and with known pro-regenerative properties. Seven patients (2 with anosmia, 5 with hyposmia) with olfactory loss without signs of sinonasal inflammation recalcitrant to olfactory training and topical corticosteroids were included. Three of the patients with hyposmia achieved normosmia at 3-month follow-up [52]. Future studies are needed in a larger cohort with controls to determine the potential benefit of this intervention.
Metaplastic respiratory epithelial replacement and aneuronal degeneration can occur with various forms of olfactory loss. Therefore, activation or replacement of the stem cells typically responsible for the normal maintenance and repair of olfactory epithelium is another promising future therapeutic option [53, 54]. Kurtenbach et al. used this concept in a mouse model of hyposmia and showed improvement in function with nasal infusion of stem cells [55]. These methods may provide a future new era of treatment for those suffering smell loss related to disorders of the olfactory epithelium including post-viral causes, toxic exposure, and aging. However, more central causes would not be expected to benefit from this technique.
Electrical neurostimulation of the olfactory bulb or more central pathways provides another potential therapeutic intervention similar to other sensory systems such as hearing, balance, and vision [56, 57]. As a recent proof-of-concept study demonstrating the ability to electrically stimulate the olfactory bulb, three of five patients reported perception of smell with stimulation transnasally through the ethmoid sinus [58••]. Further studies are underway with the ultimate goal toward an olfactory implant system, similar to other available electrical neurostimulatory devices to restore olfaction in patients with olfactory loss in the future.
留言 (0)