
記住我
A basic principle of allergy diagnosis is that reactions depend on exposure to the relevant antigen, and the pattern of reactivity is reproducible and abnormal.1 In most clinical settings, identifying relevant exposures in the clinical history and assessing reproducibility on repeated exposure to candidate antigens form the cornerstone of the diagnostic process. So, for example, a peanut allergy diagnosis would be in doubt for a patient who reacts to peanut ingestion on one occasion but tolerates peanut on other occasions, or has similar symptoms both with and without peanut exposure or has symptoms after eating peanut which are not abnormal.
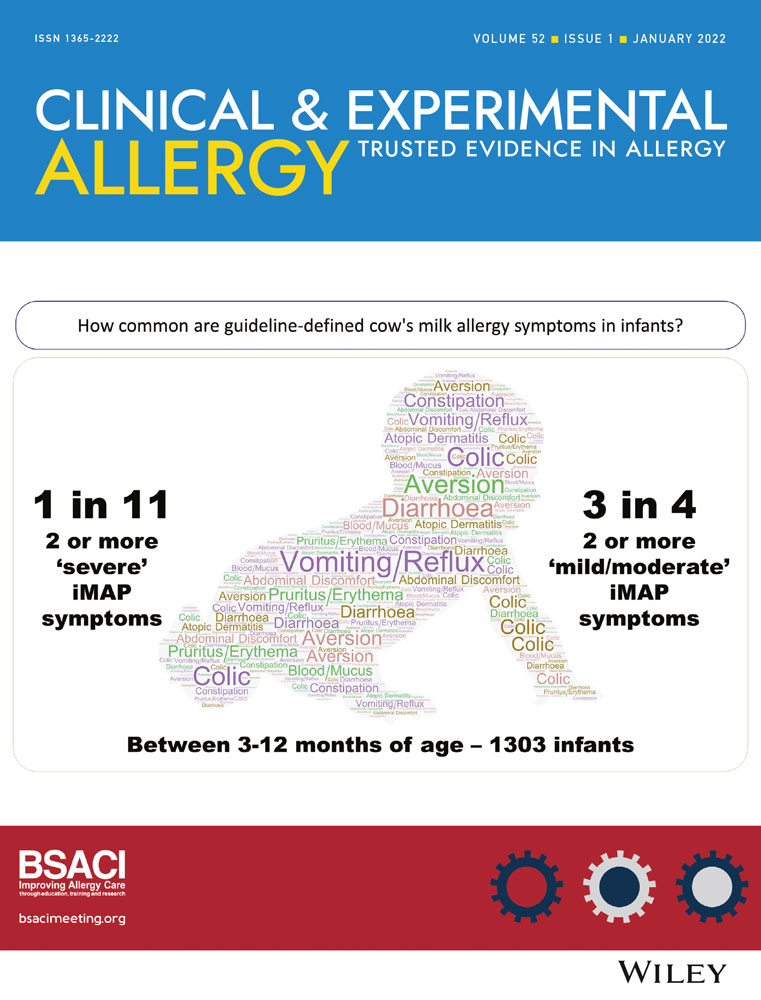
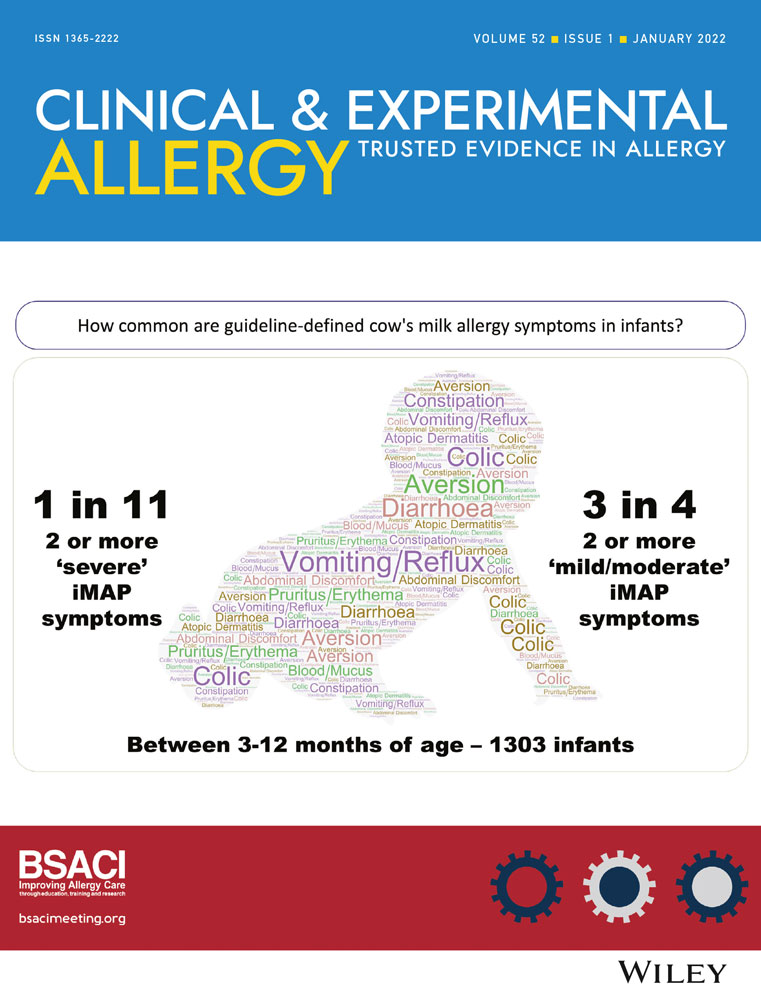
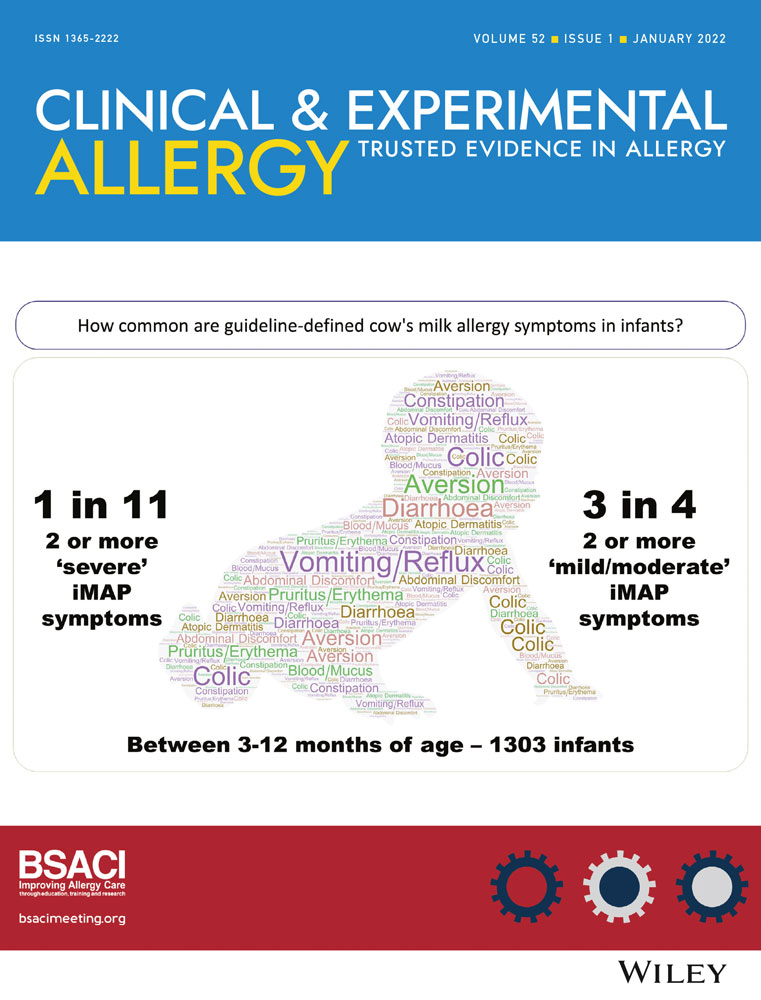
A striking exception to these widely accepted principles of allergy diagnosis is the approach taken to diagnosing cow's milk allergy in infancy. In this setting, the nature of the allergenic exposure is often ignored in guidelines—milk allergy diagnosis in breastfed infants, who consume either no cow's milk protein or nanogram quantities, is often approached similarly to formula-fed infants, who consume grams of cow's milk protein. Moreover, symptoms that are neither abnormal during infancy nor temporally related to cow's milk ingestion are posited to signify the presence of cow's milk allergy. In this month's issue, Vincent et al.2 demonstrate how misleading this approach can be for healthcare practitioners. They used the Enquiring About Tolerance (EAT) study dataset, which has detailed records of parent-reported symptoms in over 1000 infants, to assess how helpful milk allergy guidelines are for detecting potential cow's milk allergy. In EAT, 0.6% of children developed an IgE-mediated cow's milk allergy by the age of 3 years. This is consistent with double-blind placebo-controlled food challenge proven IgE- or non-IgE-mediated milk allergy rates in population-based studies. In this secondary analysis of the EAT study dataset, the authors found 74% of participants reported ≥2 symptoms of “mild/moderate” non-IgE-mediated milk allergy and 9% ≥2 “severe” symptoms between age 3 and 12 months. These rates represent the potential for a 10- to 100-fold over-diagnosis of these forms of milk allergy, using the guideline which is currently recommended by the UK General Practice Infant Feeding Network. While the EAT study population were likely to be more attuned to allergies than other populations, Vincent's analysis may have underestimated the cumulative incidence of these common infant symptoms, as data for the first 3 months of life were not available.
In the second assessment of milk allergy diagnosis in this issue, Smith et al.3 reviewed all primary care milk allergy guidelines in England. They identified 70 separate guidelines, which generally took a similar approach to the guideline assessed in Vincent's study by proposing a milk allergy diagnosis for common infant symptoms. Symptoms such as constipation, diarrhoea, colic, gastro-oesophageal reflux, blood or mucus in stools, feeding issues and rashes were almost universally cited as indicators of cow's milk allergy. For most infants, these symptoms have no connection with milk allergy—and as recently described in this journal, even blood in the stools of infants consuming cow's milk formula is most often not a reproducible cow's milk allergy.4 Every primary care guideline reviewed by Smith et al. advised maternal dietary restrictions during breastfeeding, which can be associated with anxiety, weight loss and early cessation of breastfeeding. No primary care guideline suggested any difference in diagnostic criteria between infants fed cow's milk formula and breastfed infants.
Conflicts of interest have been cited as a major issue in developing and disseminating cow's milk allergy guidelines. Recent data show approximately 10-fold over-diagnosis of milk allergy in some countries.5 The data presented in this issue by Vincent and Smith support the need for new milk allergy guidance that aligns with the basic principles of allergy diagnosis—but they do also strengthen the case for allergists and allergy societies to reconsider their relationships with the formula industry (Figure 1).6
 Graphical representation of findings from analysis of guideline-defined milk allergy prevalence in the Enquiring About Tolerance study infants. When the iMAP guideline was used to define milk allergy symptoms, “milk/moderate” or “severe” milk allergy rates were many times higher than the true prevalence of cow's milk allergy during infancy 2
Graphical representation of findings from analysis of guideline-defined milk allergy prevalence in the Enquiring About Tolerance study infants. When the iMAP guideline was used to define milk allergy symptoms, “milk/moderate” or “severe” milk allergy rates were many times higher than the true prevalence of cow's milk allergy during infancy 2
One of the most notable publications in our first year as editors in chief of Clinical and Experimental Allergy is the world-first report by Sellaturay et al7 confirming polyethylene glycol (PEG) as a cause of anaphylaxis to the Pfizer COVID-19 vaccine. PEG allergy is rare, with perhaps the largest series reporting ten patients described in this journal a year ago.8 In this issue, Sellaturay et al.9 address the question of whether patients with PEG allergy, for whom the Pfizer vaccine is contraindicated, can safely receive the Astra-Zeneca vaccine. The theoretical basis for addressing this potential cross-reactivity is that the Astra-Zeneca COVID-19 vaccine contains the excipient polysorbate-80, chemically related to PEG. In one recent series, 3 of 10 patients with PEG allergy had a positive skin prick test to polysorbate-80.8 Reassuringly, Sellaturay et al.9 report that in their relatively large cohort of eight patients with previous PEG anaphylaxis and positive PEG skin tets, all patients tolerated the Astra-Zeneca COVID-19 vaccine without reaction. This means that for people who have PEG allergy and therefore cannot receive the Pfizer or Moderna COVID-19 vaccines, there is still a safe route to COVID-19 vaccination.
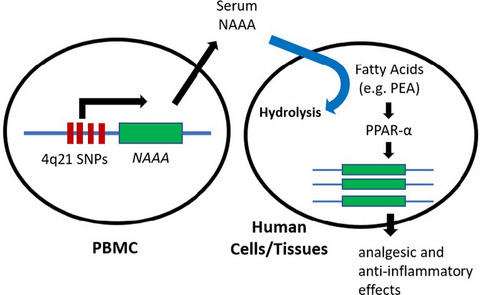
Finally, Margaritte-Jeannin et al.10 report findings from a genome-wide association study that focuses on the combined phenotype of asthma/eczema. While many individuals suffer from just one allergic condition, those with the more troublesome disease usually have multiple allergic conditions. Thus, it is relevant to evaluate whether specific genetic risk factors exist for phenotypes other than single allergic diseases. Margaritte-Jeannin et al demonstrate the value of this approach by identifying two different single nucleotide polymorphisms at the same locus, which are associated with asthma/eczema but not with either condition alone. The oculocutaneous albinism II (OCA2) locus has not previously been associated with allergic diseases, but is associated with skin and lung diseases and with epithelial barrier and immunological mechanisms. The association between this OCA2 locus and allergic diseases is worthwhile interrogating further with replication and functional studies (Figure 2).
 Margaritte-Jeannin et al. undertook a genome-wide association study and meta-analysis of other similar studies to identify whether there were specific single nucleotide polymorphisms associated with the combined phenotype of asthma/eczema, different to those linked with asthma or eczema alone. They identified two polymorphisms in a novel locus, OCA2, which has not previously been linked with asthma or eczema.10
Margaritte-Jeannin et al. undertook a genome-wide association study and meta-analysis of other similar studies to identify whether there were specific single nucleotide polymorphisms associated with the combined phenotype of asthma/eczema, different to those linked with asthma or eczema alone. They identified two polymorphisms in a novel locus, OCA2, which has not previously been linked with asthma or eczema.10
留言 (0)