
記住我

Psoriasis is a chronic inflammatory autoimmune disease consisting of psoriasis vulgaris, erythrodermic psoriasis, pustular psoriasis, etc., which often occurs with inflammatory response in joints, nails, or other organs and frequently associates with a high risk of comorbidities, such as obesity, psoriatic arthritis, and Crohn's disease.1-4 Its prevalence is approximately 2% worldwide, which varies among different races, countries, and regions.3 Although the management of psoriasis has been improved over the past few decades and treatment methods are effective for psoriasis patients, including biological agents, vitamin D analogues, immune inhibitors, topical corticosteroids, and phototherapy, non-response to treatment still exists and bothers patients and their families.5, 6 Therefore, it might be necessary to find out new biomarkers to better reflect psoriasis risk, disease activity, and treatment outcome, then further improving the management of psoriasis patients.
Dual specificity phosphatase 22 (DUSP22), also named C-Jun N-terminal kinase (JNK) pathway-associated phosphatase (JAKP), is a tyrosine phosphatase with 184 amino acid residues extensively expressed in human tissues and systems.7 It is reported that DUSP22 involves in T-cell activity and immunity. For instance, via activating lymphocyte-specific protein tyrosine kinase (Lck), DUSP22 suppresses T-cell receptor (TCR) signaling, which contributes to the T cell-mediated immunity and autoimmunity7; DUSP22 inhibits T-cell activation, while its knockout in mice triggers autoimmunity and participates in the pathogenesis of systemic lupus erythematosus (SLE).8 Meanwhile, in patients with psoriasis, functional defects in CD4+CD25+ forkhead box protein 3 (Foxp3)+ regulatory T cells (Tregs) inhibit the excess immune response and mediate homeostasis, further contributing to the pathogenesis of psoriasis.9 Besides, it is also suggested that DUSP22 plays clinical functions in immune- or inflammation-related diseases. For example, DUSP22 has positive association with treatment response in rheumatoid arthritis (RA) patients10; blood DUSP22 negatively associates with T helper (Th)1 and Th 17 in sepsis patients.11 Since psoriasis is an immune disease accompanied by inflammatory indications and based on the above information, we hypothesized that DUSP22 might serve as a potential biomarker for disease activity and treatment outcome of psoriasis.
This study aimed to investigate the abnormality of DUSP22 level, its longitudinal change with time, and its correlation with clinical characteristics and treatment response in psoriasis patients.
2 METHODS 2.1 SubjectsFrom January 2018 to November 2020, one hundred and twenty psoriasis patients were consecutively enrolled in this study. The enrolled patients were required to meet the following conditions: (a) diagnosed as psoriasis; (b) more than 18 years old; (c) confirmed as moderate to severe psoriasis, which was defined as psoriasis area severity index (PASI) score >8 and the psoriatic body surface area (BSA) >10%; (d) plaque type applicable and were willing to receive etanercept-based treatment. The patients were excluded from the study for any of the following reasons: (a) presented as pustular psoriasis or psoriatic arthritis; (b) history of cancers or hematological malignancies; and (c) pregnant or lactating women. In addition, from January 2018 to November 2020, fifty patients with other skin inflammations and fifty health subjects were also enrolled in the study as disease controls (DCs) and health controls (HCs), respectively. To eliminate the potential bias, the age and gender of DCs and HCs were matched to the psoriasis patients. All subjects provided written informed consents before enrollment, and the study was approved by the Institutional Review Board.
2.2 Data collectionDemographic characteristics of all subjects were gathered for the study use. For psoriasis patients specifically, clinical characteristics were also collected, which included disease duration, psoriatic BSA, PASI score, history of topical therapy, history of phototherapy, history of systemic non-biologic treatment, and history of systemic biologic treatment. In addition, current treatment regimens apart from etanercept of psoriasis patients were recorded as well.
2.3 Sample collection and assessmentSerum samples were collected from psoriasis patients at admission as well as from DCs and HCs after enrollment. For psoriasis patients, serum samples were also obtained at month 1 (M1), month 3 (M3), and month 6 (M6) after initiation of etanercept-based treatment. Sequentially, serum samples were used to assess the level of DUSP22 by enzyme-linked immunosorbent assay (ELISA) using commercial human ELISA kits (Shanghai Enzyme-linked Biotechnology Co., Ltd). The ELISA procedures were carried out according to the instruction from the manufacturer.
2.4 Treatment and assessmentAll patients were treated by etanercept subcutaneously at a dose of 25 mg twice a week.12 Meanwhile, topical therapy, phototherapy, or systemic non-biologic treatment was applied as combination therapy based on clinical needs. During treatment, PASI score was assessed at baseline (M0), M1, M3, and M6 after initiation of the treatment, which was assessed on the basis of erythema, scales, and thickness at four anatomical sites of head, upper extremities, trunk, and lower extremities. PASI score ranged from 0 (no disease) to 72 (most severe disease). On the basis of the PASI score, PASI 75 response and PASI 90 response were used to evaluate treatment efficacy. PASI 75 response was defined as patients achieving a 75% decrease in PASI score from the baseline; PASI 90 response was defined as patients achieving a 90% decrease in PASI score from the baseline. Based on the PASI 75 response at M6 and PASI 90 response at M6, the psoriasis patients were divided as response patients and non-response patients.
2.5 Statistical analysisA total of 16 psoriasis patients lost follow-up during 6 months, which were analyzed with the last observation carried forward (LOCF) method. Statistical analysis and graph plotting were completed by SPSS 24.0 (IBM Corp., Armonk, New York, USA) and GraphPad Prism 6.01 (GraphPad Software Inc.), respectively. Comparison of DUSP22 between two groups was determined by the Wilcoxon rank sum test, and receiver operating characteristic (ROC) curve analysis was used to evaluate the performance of DUSP22 in distinguishing different subjects. Correlation of two continuous variables was determined by the Spearman's rank correlation test, and correlation of continuous variable and dichotomous variable was analyzed by the Wilcoxon rank sum test. The change of DUSP22 level over time was assessed by the Friedman test. A p value <0.05 indicated a statistical significance.
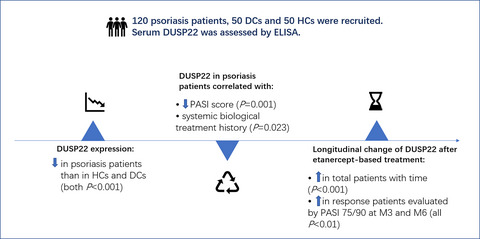
3 RESULTS 3.1 Clinical characteristics of psoriasis patientsA total of 120 psoriasis patients were recruited in this study, whose clinical characteristics are shown in Table 1. In short, the mean age of psoriasis patients was 52.7 ± 11.7 years. There were 43 (35.8%) females and 77 (64.2%) males. Besides, the median (interquartile range) psoriatic BSA was 17.0 (14.0–22.0) % and the mean PASI score was 13.3 ± 4.9 in psoriasis patients. Moreover, in terms of the current treatment, 100 (100.0%), 94 (78.3%), 62 (51.7%), and 46 (38.3%) patients received etanercept, topical therapy, phototherapy, and systemic non-biologic treatment, respectively.
TABLE 1. Clinical characteristics of psoriasis patients Items Psoriasis patients (N = 120) Demographics Age (years), mean ± SD 52.7 ± 11.7 Gender, no. (%) Female 43 (35.8) Male 77 (64.2) BMI (kg/m2), mean ± SD 23.9 ± 3.4 Disease characteristics Disease duration (years), median (IQR) 7.0 (4.0–14.8) Psoriatic BSA (%), median (IQR) 17.0 (14.0–22.0) PASI score, mean ± SD 13.3 ± 4.9 Treatment history History of topical therapy, no. (%) No 9 (7.5) Yes 111 (92.5) History of phototherapy, no. (%) No 19 (15.8) Yes 101 (84.2) History of systemic non-biologic treatment, no. (%) No 41 (34.2) Yes 79 (65.8) History of systemic biologic treatment, no. (%) No 102 (85.0) Yes 18 (15.0) Current treatment Etanercept, no. (%) No 0 (0.0) Yes 100 (100.0) Topical therapy, no. (%) No 26 (21.7) Yes 94 (78.3) Phototherapy, no. (%) No 58 (48.3) Yes 62 (51.7) Systemic non-biologic treatment, no. (%) No 74 (61.7) Yes 46 (38.3) Abbreviations: BMI, body mass index; BSA, body surface area; IQR, interquartile range; PASI, psoriasis area severity index; SD, standard deviation. 3.2 DUSP22 in psoriasis patients, HCs, and DCsDUSP22 was decreased in psoriasis patients than in HCs (p < 0.001); meanwhile, the receiver operating characteristic (ROC) curve showed that DUSP22 possessed good capability in discriminating psoriasis patients from HCs with area under curve (AUC) of 0.886 (95% confidence interval (CI): 0.836–0.936) (Figure 1A-B). Besides, DUSP22 in psoriasis patients was also lower than that in DCs (p < 0.001); meanwhile, DUSP22 had certain ability of distinguishing psoriasis patients from DCs, of which AUC was 0.743 and 95%CI was 0.665–0.821 (Figure 1C-D). Moreover, DUSP22 was declined in DCs compared with HCs (p = 0.001). Furthermore, DUSP22 possessed certain potential in differentiating DCs from HCs, with AUC of 0.689 and 95%CI of 0.584–0.794 (Figure 1E-F).

Comparison of DUSP22 among psoriasis patients, HCs and DCs. DUSP22 in psoriasis patients and HCs (A); ability of DUSP22 to distinguish psoriasis patients from HCs (B); DUSP22 in psoriasis patients and DCs (C); potential of DUSP22 in discriminating psoriasis patients from DCs (D); DUSP22 in HCs and DCs (E); capability of DUSP22 in differentiating DCs from HCs (F). DUSP22, dual specificity phosphatase 22; HCs, health controls; AUC, area under curve; CI, confidence interval; DCs, disease controls
3.3 Correlation of DUSP22 with clinical characteristics in psoriasis patientsDUSP22 was negatively correlated with PASI score (rs = −0.313, p = 0.001), but positively associated with history of systemic biological treatment (p = 0.023) in psoriasis patients; however, no correlation was found in DUSP22 with other clinical features in psoriasis patients (all p > 0.05) (Figure 2A-J).

Correlation of DUSP22 with psoriasis patients' features. Association of DUSP22 with age (A), gender (B), BMI (C), disease duration (D), psoriatic BSA (E), PASI score (F), history of topical therapy (G), history of phototherapy (H), history of systemic non-biologic treatment (I), history of systemic biologic treatment (J) in psoriasis patients. DUSP22, dual specificity phosphatase 22; BMI, body mass index; BSA, body surface area; PASI, psoriasis area severity index
3.4 Correlation of DUSP22 with treatment responseThe treatment response rate evaluated by PASI 75 at M1, M3, and M6 was 13.3%, 34.2%, and 68.3%, respectively, and that evaluated by PASI 90 at M1, M3, and M6 was 1.7%, 18.3%, and 35.0%, respectively (Table 2). After treatment, DUSP22 elevated over time in psoriasis patients (p < 0.001) (Figure 3).
TABLE 2. Treatment response rate at different time points Items PASI 75 PASI 90 M1 M3 M6 M1 M3 M6 Number of patients (n) 16 41 82 2 22 42 Percentage (%) 13.3 34.2 68.3 1.7 18.3 35.0 Abbreviations: M1, one month; M3, three months; M6, six months; PASI 75, psoriasis area severity index score declines more than 75%; PASI 90, psoriasis area severity index score declines more than 90%.
Change of DUSP22 with time. DUSP22, dual specificity phosphatase 22; M, month
Notably, DUSP22 increased with time in response patients evaluated by PASI 75 (p < 0.001), response patients evaluated by PASI 90 (p < 0.001), and non-response patients evaluated by PASI 90 (p < 0.001); however, no difference was discovered in DUSP22 at different time points among non-response patients evaluated by PASI 75 (p = 0.659) (Figure 4A-D). Furthermore, DUSP22 at M3 (p = 0.004) and M6 (p < 0.001), but not at M0 or M1, was higher in the response patients than in the non-response patients evaluated by PASI 75 (Figure 5A). Additionally, DUSP22 at M3 (p < 0.001) and M6 (p = 0.003), but not at M0 or M1, was also increased in the response patients compared with the non-response patients evaluated by PASI 90 (Figure 5B). Furthermore, according to the forward stepwise multivariate logistic regression analysis, DUSP22 at M6 (p = 0.003, odds ratio (OR) = 1.015) and history of topical therapy (yes vs. no) (p = 0.060, OR = 4.196) were independently associated with better treatment response in psoriasis patients evaluated by PASI 75 at M6, and DUSP22 at M6 was also independently correlated with satisfactory treatment response in psoriasis patients evaluated by PASI 90 at M6 (p = 0.001, OR = 1.012) (Table S1).

DUSP22 plaque type in response or non-response patients. Change of DUSP22 with time in response (A) and non-response patients (B) evaluated by PASI 75, as well as in response (C) and non-response patients (D) evaluated by PASI 90. DUSP22, dual specificity phosphatase 22; PASI, psoriasis area severity index; M, month

Comparison of DUSP22 between response patients and non-response patients. Comparison of DUSP22 between response and non-response patients evaluated by PASI 75 (A); comparison of DUSP22 between response and non-response patients evaluated by PASI 90 (B). DUSP22, dual specificity phosphatase 22; PASI, psoriasis area severity index; M, month
4 DISCUSSIONIn the present study, we found that: (1) DUSP22 was decreased in psoriasis patients than in HCs and DCs; besides, DUSP22 could distinguish psoriasis patients from HCs and DCs; (2) DUSP22 was negatively associated with PASI score and positively correlated with history of systemic biologic treatment in psoriasis patients; (3) DUSP22 increased with time after treatment and its longitudinal elevation positively associated with treatment response to etanercept in psoriasis patients.
Regarding the DUSP22 level in patients with immune diseases and HCs, a precious study shows that DUSP22 is lower in juvenile idiopathic arthritis (JIA) patients than in HCs.13 Another study suggests that DUSP22 is downregulated in patients with active Crohn's disease and ulcerative colitis compared to HCs.14 Additionally, DUSP22 in RA patients is reduced than that in HCs.10 In our study, we observed that DUSP22 was lower in psoriasis patients than in HCs and DCs, which could be explained by that: DUSP22 inhibited TCR and attenuated T cell-mediated immune response through inactivating Lck, which might affect the development of psoriasis.7 In addition, we also found that DUSP22 could discriminate psoriasis patients from HCs and DCs, indicating the potential of DUSP22 as a biomarker for psoriasis risk.
In terms of the association of DUSP22 with clinical features in inflammation-related diseases, it is reported that DUSP22 correlates with milder disease severity and lower level of inflammation cytokines in sepsis.15 It is also revealed that in asthmatic exacerbation children, DUSP22 negatively associates with eosinophil count and immunoglobulin E.16 Besides, DUSP22 is negatively correlated with Unified Parkinson's Disease Rating Scale (UPDRS)-I score and UPDRS-III score in Parkinson patients.17 In our study, we discovered that DUSP22 was negatively associated with PASI score and positively correlated with history of systemic biologic treatment in psoriasis patients. Possible reasons might be that: (1) DUSP22 could suppress T-cell activation and the proliferation of CD4+ T cells through JNK pathway,14 which would alleviate inflammation and subsequently result in less serious skin lesion in psoriasis; DUSP22 could suppress the activity of T-cell immune response, which played an important role in the function of keratinocytes, then further slowing down the aberrant proliferation of keratinocytes and causing a lower disease activity in psoriasis patients.7, 18 Thus, DUSP22 showed a negative correlation with PASI score in psoriasis patients; (2) as DUSP22 was negatively correlated with inflammatory levels (as in various inflammation-related diseases),7, 15, 16 and systemic biologic treatment had strong anti-inflammation effect, and thus, DUSP22 was positively correlated with history of systemic biologic treatment in psoriasis patients.
Concerning the correlation of DUSP22 with treatment response in inflammation-related disease, it has been illustrated that DUSP22 increases gradually with treatment time and positively associates with treatment response in RA patients10; meanwhile, increment of DUSP22 during etanercept treatment is also correlated with satisfactory treatment response in RA patients.19 Moreover, circulating DUSP22 relates to treatment response and serves as a novel biomarker for predicting clinical response in Crohn's disease patients.7 In our study, we also conducted this rare analysis in psoriasis; subsequently, we discovered that DUSP22 increased over time after treatment and its longitudinal elevation was positively associated with treatment response to etanercept in psoriasis patients. Explanations could be listed as follows: (1) etanercept was a tumor necrosis factor (TNF)-α inhibitor, which inhibited inflammation and immune response,20 and DUSP22 reflected decreased inflammation level,15 thus DUSP22 elevated with time; (2) DUSP22 was associated with milder disease activity as above mentioned; therefore, it might indirectly reflect better treatment response.
Although a lot of findings were identified in this study, there still existed several limitations. First, the sample size could be expanded to improve the statistical power. Second, since etanercept was only suitable for plaque type patients, patients with other types of psoriasis were excluded from this study. Thus, our findings were not applicable in patients with other types of psoriasis except the plaque type. The potential of DUSP22 as a biomarker in these patients might be further explored in future. Third, this study did not investigate the molecular mechanism of DUSP22 in the progression of psoriasis, and thus, in vivo and in vitro experiments could be conducted. Fourth, we did not detect the keratinocyte level, and thus, subsequent study could be performed on the correlation of DUSP22 in keratinocyte with clinical features and treatment response in psoriasis.
Conclusively, DUSP22 is insufficiently expressed and negatively correlated with disease activity in psoriasis patients, while its longitudinal increase with time reflects satisfactory treatment response in psoriasis patients.
ACKNOWLEDGMENTThis study was supported by Fund project of Hubei Health Commission (No. WJ2019F048).
CONFLICTS OF INTERESTThe authors declare that they have no conflicts of interest.
留言 (0)