
記住我
The risk of liquid nicotine exposure has increased recently because of the popularity of e-cigarettes; this exposure can be fatal.1 We describe a case of a suicide attempt through ingestion of 600 mg of liquid nicotine resulting in cardiac arrest.
CASE PRESENTATIONA 55-year-old man was found unconscious on a riverbank and was brought to our hospital by ambulance. His medical history included depression, hyperlipidemia, and type 2 diabetes mellitus, but no coronary artery disease. His family history was unremarkable. He left a suicide note at his home, and two open bottles of liquid nicotine were found near him. A total of 600 mg of liquid nicotine had been used. The following vital signs were noted: his blood pressure could not be measured, but carotid artery pulsation was palpable; heart rate, 82 b.p.m; percutaneous oxygen saturation, 74% on ambient air. His Glasgow Coma Scale (GCS) score was 3. His pupils were 6 mm in diameter bilaterally, and no light reflex was observed. Although the paramedics delivered oxygen and assisted ventilation, the patient developed bradycardia, followed by asystole during transport (Fig. 1). Basic life support (BLS) was immediately performed by paramedics, and spontaneous circulation resumed within approximately 2 min. At presentation to our hospital, his weight was 52 kg, and his vital signs were as follows: blood pressure, 163/96 mm Hg; heart rate, 145 b.p.m; percutaneous oxygen saturation, 98% on 10 L O2/min. The patient's GCS score, pupil size, and light reflex were the same as assessed by the paramedics. A 12-lead electrocardiogram (ECG) revealed sinus tachycardia. An arterial blood gas analysis revealed respiratory and metabolic acidosis: pH, 7.040; partial pressure of CO2, 73.0 Torr; partial pressure of O2, 526.0 Torr; bicarbonate, 19.7 mmol/L; lactate, 8.8 mmol/L. His blood glucose level was 375 mg/dL, and no renal or hepatic dysfunction was observed. His high-sensitivity troponin I value was 27.0 pg/mL. The anion gap was 18 mmol/L and ketones were not detected. Whole-body computed tomography revealed no findings responsible for the coma. His urine drug screen was negative, including for phencyclidines, benzodiazepines, cocaine, cannabis, morphine, and barbituric acids. He had increased secretions and transient seizures on the day of admission, but no fasciculations. Shortly after presentation, his GCS score improved to full, and blood tests showed no hepatic, renal, or coagulation abnormalities. Brain magnetic resonance imaging revealed no obvious abnormalities. An anticonvulsant was administered for 2 days, and no convulsions occurred thereafter. The patient admitted ingesting the liquid nicotine with the intention of committing suicide. This case was judged to be cardiac arrest due to nicotine poisoning, although the patient's blood nicotine and cotinine levels could not be measured. He was informed about the treatment provided, and he adhered to and tolerated the treatment well. He was treated by a psychiatrist for depression during his hospitalization and discharged after 24 days without any neurological defects or sequelae related to nicotine intoxication.

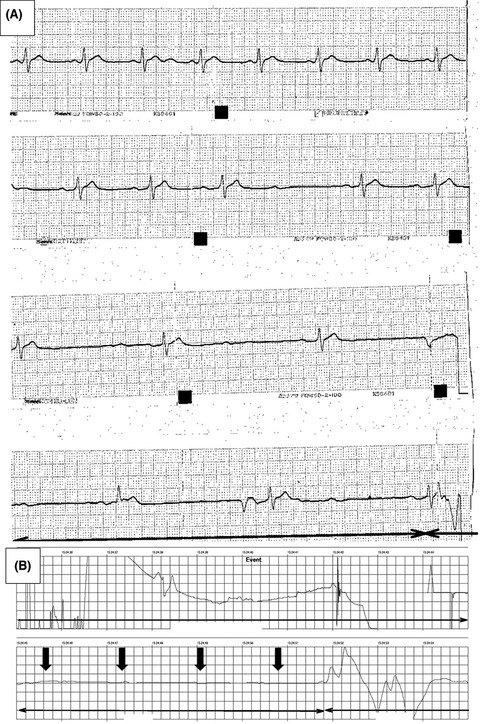
Electrocardiogram (ECG) tracings from the ambulance monitor: (A) ECG tracing from the automated external defibrillator (AED); (B) ECG tracing during transport on the ambulance. The waveform gradually transitioned from sinus rhythm to sinus bradycardia to asystole after the AED was applied (arrows).
DISCUSSIONNicotine addiction has received attention recently with the widespread use of liquid nicotine.1 This report reveals a patient's ECG readings over time, including during cardiac arrest, after he orally ingested a potentially lethal dose of nicotine. To the best of our knowledge, this is the first report of a monitor capturing the moment of cardiac arrest due to nicotine intoxication. After ingestion, nicotine is absorbed through the intestinal mucosa and metabolized primarily in the liver,2 where it is converted to a lactam derivate via cytochrome oxidase pathways involving cytochrome P450 2A6.3 The first-pass effect reduces nicotine bioavailability by 30%–40%4; plasma nicotine has a half-life of 40–120 min.5 Clinical manifestations of nicotine stimulation can be explained by autonomic nervous system stimulation. Nicotine stimulates nicotinic acetylcholine receptors in the sympathetic and parasympathetic nervous systems, inducing a mixed response.3, 6 Sympathetic nervous system symptoms, (e.g., nausea, salivation, tachycardia, increased bronchial secretions, anxiety, hypertension, seizures, and muscle spasms) occur first, followed by paradoxical suppression symptoms, (e.g., drowsiness, paralysis, dyspnea, bradycardia, and hypotension).7 Our patient’s ECG waveform shifted from sinus rhythm to sinus bradycardia to asystole. Although we do not have evidence, cardiac arrest seen in our patient most likely occurred because of parasympathetic nervous system stimulation with high-dose nicotine. Vasovagal reflex following tachycardia associated with sympathetic stimulation may have been involved.8
A lethal dose of nicotine is 60 mg, although adults can reportedly survive oral ingestion of nicotine doses >500 mg6; the amount of nicotine orally ingested by our patient was 600 mg, equivalent to 11.5 mg/kg body weight. This case had a favorable neurological outcome because the cardiac arrest was witnessed by the paramedics, under oxygen supply, and BLS was immediately performed, leading to return of spontaneous circulation within ~2 min. Our case may underscore the reversibility of cardiac arrest due to nicotine poisoning and the importance of prompt initiation of BLS.
CONCLUSIONWe have reported a case of a patient who presented with cardiac arrest following ingestion of a high dose of nicotine and who was successfully treated with prompt initiation of BLS because of the rapid metabolism of the nicotine. Currently, there are limited data on the clinical features and treatments for intentional ingestion of potentially fatal amounts of liquid nicotine. This report provides emergency physicians with valuable information regarding the management of nicotine intoxication.
ACKNOWLEDGEMENTSWe thank Christine Burr for English language editing.
DISCLOSUREApproval of the Research Protocol with approval No. and committee Name: Not applicable.
Informed Consent: Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Registry and the Registration No. of the study/Trial: Not applicable.
Animal Studies: Not applicable.
Conflict of Interest: All authors of this manuscript have no conflicts of interests and have no commercial, financial, and any other relationships related to the subject of this article as per the ICMJE conflict of interest guidelines.
REFERENCES
1Maessen GC, Wijnhoven AM, Neijzen RL et al. Nicotine intoxication by e-cigarette liquids: A study of case reports and pathophysiology. Clin. Toxicol. (Phila.) 2020; 58: 1– 8. 2Mishra A, Chaturvedi P, Datta S, Sinukumar S, Joshi P, Garg A. Harmful effects of nicotine. Indian J. Med. Paediatr. Oncol. 2015; 36: 24– 31. 3Benowitz NL. Pharmacology of nicotine: Addiction, smoking-induced disease, and therapeutics. Annu. Rev. Pharmacol. Toxicol. 2009; 49: 57– 71. 4Paik JH, Kang S, Durey A et al. Symptomatic bradycardia due to nicotine intoxication. Rev. Bras. Ter. Intensiva 2018; 30: 121– 6. 5Benowitz NL, Jacob P 3rd. Nicotine and cotinine elimination pharmacokinetics in smokers and nonsmokers. Clin. Pharmacol. Ther. 1993; 53: 316– 23. 6Mayer B. How much nicotine kills a human? Tracing back the generally accepted lethal dose to dubious self-experiments in the nineteenth century. Arch. Toxicol. 2014; 88: 5– 7. 7Schep LJ, Slaughter RJ, Beasley DM. Nicotinic plant poisoning. Clin. Toxicol. (Phila). 2009; 47: 771– 81. 8Brignole M, Menozzi C, Del Rosso A et al. New classification of haemodynamics of vasovagal syncope: beyond the VASIS classification: Analysis of the pre-syncopal phase of the tilt test without and with nitroglycerin challenge. Europace 2000; 2: 66– 76.
留言 (0)