
記住我


A 72-year-old man with a 40 pack-year smoking history, chronic obstructive pulmonary disease, hypertension, and hyperlipidemia presented with a 1-week loss of right visual fields, gait instability, and forgetfulness. On examination, he was found to have right homonymous hemianopia. Gardening was one of his hobbies, and he would regularly sustain scratches and punctures during gardening but denied major head or skin trauma. He was not immunocompromised and did not abuse intravenous drugs or participate in adventurous travel.
A head CT followed by an MRI showed a 3.4 cm left occipital lesion with extensive surrounding vasogenic edema on T2, central diffusion restriction on diffusion-weighted imaging, and irregular rim enhancement on contrast-enhanced T1-weighted imaging (Figure 1). A metastatic workup including CT of the chest, abdomen, and pelvis was negative. He underwent a craniotomy which demonstrated a mass with a liquified necrotic-appearing core that was resected en bloc with a portion sampled for microbiology studies.

MRI showing a 3.4 cm left occipital lesion with rim enhancement (arrow) on contrast-enhanced T1-weighted imaging
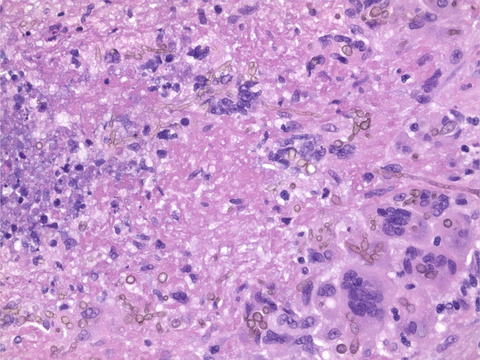
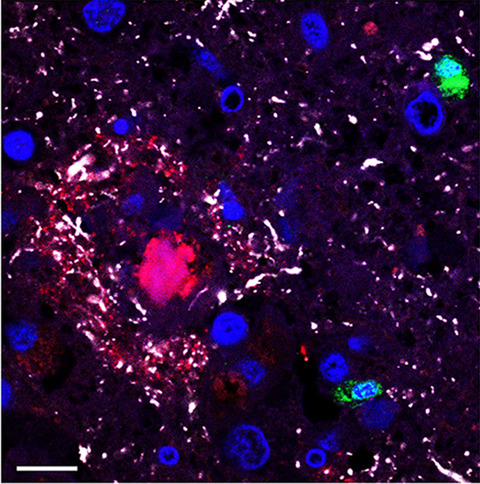
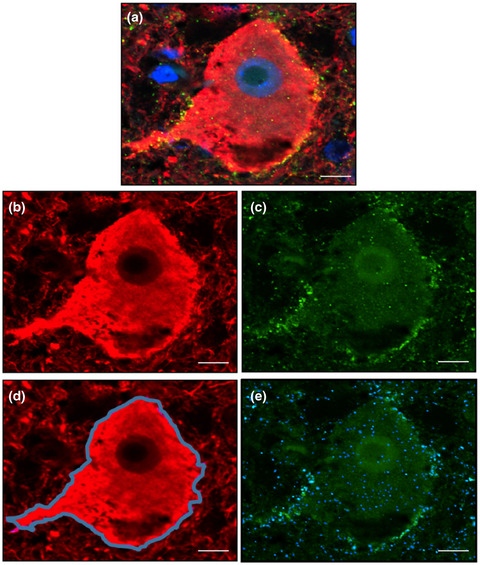
Microscopic examination demonstrated florid necrotizing granulomatous inflammation with frequent histiocytes, lymphocytes, and multinucleated giant cells palisading large areas of geographic necrosis (Box ) (Figure 2A). There were numerous admixed pigmented branched hyphae with irregular swellings and septa with constrictions, as well as conidia. The organisms were also present within multinucleated giant cells (Figure 2B) and focally within the walls of small vessels. The hyphae were highlighted by Grocott-Gomori methenamine silver stain (GMS) (Figure 2C) and periodic acid-Schiff stain (PAS) (Figure 2D). The surrounding brain tissue showed gliosis, vacuolization, and focal dystrophic calcification.

(A) Histologic sections demonstrate prominent granulomatous inflammation and necrosis (40x) (B) with pigmented branched hyphae focally within multinucleated giant cells (H&E, 400x). Septate hyphae with irregular swellings are highlighted on (C) GMS and (D) PAS stains (400x)
2 FINAL DIAGNOSISCladophialophora bantiana brain abscess (cerebral phaeohyphomycosis).
Cultures on brain tissue sent intraoperatively grew C. bantiana. A formalin-fixed paraffin-embedded block was sent to the University of Washington Medical Center Molecular Microbiology Laboratory for fungal identification by PCR which detected C. bantiana DNA.
3 DISCUSSIONPhaeohyphomycosis describes infections caused by dematiaceous fungi which are pigmented molds found in soil and plants worldwide [1, 2]. Pigmentation is because of hyphae and conidia containing melanin, considered a major virulence factor. The pigment is able to protect the fungi against a wide range of toxic insults, possibly by scavenging reactive oxygen species and binding hydrolytic enzymes produced by the host's immune response [2]. Strains of Cryptococcus neoformans and Exophiala (Wangiella) dermatitidis that lack melanin have shown decreased virulence in mouse studies [2]. Most of the dematiaceous fungi that cause cerebral phaeohyphomycosis are from the order of environmental fungi, Chaetothyriales, such as C. bantiana (previously known as Cladosporium trichoides, Cladosporium bantianum, Torula bantiana, Xylohypha bantiana, and Xylohypha emmonsii), Rhinocladiella mackenziei, and E. dermatitidis [1, 2].
Unlike many life-threatening fungal infections which are often associated with severe immunosuppression, cerebral phaeohyphomycosis is seen in immunocompetent as well as immunocompromised patients [2]. C. bantiana has a particular neurotropism, with almost all infections confined to the central nervous system (CNS), and, although rare, is the most common cause of cerebral phaeohyphomycosis, frequently presenting as brain abscesses [1, 2]. The mechanism underlying the neurotropism is unknown but may be associated with its ability to convert phenolic compounds in the human brain [1]. Infections with C. bantiana occur more often in immunocompetent than in immunocompromised patients, with a male predilection for unclear reasons although increased environmental exposure has been postulated [2, 3].
The route of infection is not well understood. Localization throughout the cerebrum, most commonly in the frontal and parietal lobes and less commonly in the occipital lobe, as well as the involvement of the cerebellum and ventricles, suggests hematogenous spread, possibly from cutaneous traumatic inoculation or pulmonary infection, although most patients show no evidence of prior pulmonary involvement, [1, 3]. Angioinvasion is rarely seen on microscopic examination, described only in two transplant patients [1]. Our patient may have been exposed through implantation of fungal organisms in his skin during gardening.
Over half of the patients with cerebral infection by C. bantiana present with headaches and one third with seizures and altered mental status [1, 3]. Other common symptoms include hemiparesis, dysarthria, and nausea and vomiting. Visual disturbances have been reported in 7–11% of patients and walking difficulties in 3–8% [1, 3]. Ring-enhancing lesions are often seen on MRI [1].
Characteristic neuropathologic features include necrotizing granulomatous inflammation with multinucleated giant cells. Brown, irregularly swollen fungal hyphae with branching and septa can usually be readily seen on routine H&E staining although they stain intensely with PAS and GMS stains [1, 2]. As the hyphae may not appear pigmented early in infection, melanin stains such as the Fontana-Masson stain may be useful in detecting melanin pigment; however, nondematiaceous fungi such as Aspergillus species and Zygomycetes also occasionally stain positively [1, 2].
Although there is no standard treatment for CNS phaeohyphomycosis [3], complete resection and combination amphotericin B, flucytosine, and itraconazole have been associated with improved survival [2, 3]. Itraconazole and voriconazole have the most potent activity with the newer azole, voriconazole, able to achieve both cerebrospinal fluid and brain parenchymal penetration [2].
C. bantiana infection is associated with a high mortality rate ranging from 60 to 70% even with aggressive surgical and antifungal therapy and is almost always fatal without treatment [2, 3]. As recurrences can occur months after therapy, long-term follow-up (over a year) is recommended [2]. Our patient was started on intravenous amphotericin B with the addition of fluconazole and was subsequently switched to oral voriconazole. At follow-up 9 months after resection, there was no clinical evidence of recurrence.
In conclusion, cerebral phaeohyphomycosis by C. bantiana is an important consideration in the differential diagnosis of ring-enhancing lesions in both immunocompetent and immunocompromised patients. Although it has been associated with high morbidity and mortality, prompt surgical resection and treatment with newer antifungal drugs may lead to improved prognosis.
ACKNOWLEDGMENTSWe thank the University of Washington Medical Center Molecular Microbiology Laboratory for assistance with fungus identification.
CONFLICT OF INTERESTThe authors declare no conflicts of interest.
AUTHOR CONTRIBUTIONSShino Magaki, Laura Denham, and Jeremy Deisch performed acquisition and analysis of pathologic data. Warren Boling, Ingrid Blomquist, and Sheri Harder performed acquisition and analysis of clinical data. Shino Magaki and Jeremy Deisch drafted and revised the manuscript with input from the authors. All authors have read and approved the final manuscript.
留言 (0)