
記住我
Postpartum hemorrhage (PPH) is a major cause of maternal mortality worldwide.1 In Japan, PPH is the main cause of maternal death, accounting for 19% in the last 10 years.2-4 Most PPH associated deaths occur due to a reduction in circulating plasma volume, leading to a depletion shock, due to delayed diagnosis and treatment. The “Guidelines for Handling Critical Obstetric Hemorrhage 2017” in Japan recommend transporting the patient to a higher medical institution as soon as PPH is determined.5 However, an analysis of 213 deaths in Japan noted delayed transport to a higher medical institution in 30 cases.6, 7
In Japan, the perinatal transfer system to hospitals has been established on a prefectural basis. The Kanagawa Prefecture, where our hospital is located, is divided into six blocks and 28 hospitals are designated as hospitals with perinatal emergency services.8 The Tokyo Prefecture has established a comprehensive perinatal center that accepts all cases, shortening the time required to select a recipient center.9 In the Netherlands, if maternal transport is required, the law requires an arrival time from the emergency call to a higher medical institution within 45 min.10 However, despite the abovementioned efforts, guidelines do not provide a standard transfer time, and we could not find any studies on the transfer time of PPH patients in Japan. Therefore, this study aimed to describe the transport time and timing of transfer of patients with PPH to a tertiary care institution in an urban area.
METHODS Study patientsWe undertook a retrospective cohort study on all patients with PPH transferred to our hospital by ambulance, and covered by the hospital’s original system, “Puerperium call” from April 2016 to March 2020. When an obstetrician receives a patient with PPH, the emergency physician issues the “Puerperium call.” Resultantly, the laboratory prepares blood products, an operating room is secured, and emergency physicians and obstetricians begin to prepare for the initial response. We excluded cases that did not meet the definition of PPH. Postpartum hemorrhage has traditionally been defined as a blood loss of 500 mL or 1,000 mL after a vaginal birth or cesarean section, respectively.11, 12 However, in recent years, it has been recommended that PPH be defined as bleeding of more than 1,000 mL or bleeding with signs of low circulation within 24 h after delivery, regardless of whether the birth is vaginal or by cesarean section, and this definition was adopted in this study.13, 14 Cases with missing data on vital signs and time course of transport were excluded.
Patient-related and clinical dataPatient-related and clinical data were collected. The causes of PPH were classified into four categories: tonus due to poor uterine contraction, trauma due to laceration or hematoma, tissue due to placental remnant or adherent placenta, and thrombin due to coagulation disorder. The time zone of the transfer request was defined as day shift, from 9:00 a.m. to 5:00 p.m., and other times. Transfer time was divided into the following four categories: (i) from transfer request to emergency call, (ii) from emergency call to arrival of the emergency team, (iii) from arrival of the emergency team to beginning of transport, (iv) from beginning of transport to hospital arrival. Patient information and time lapse data were extracted from medical records and emergency transport records.
Shock indexThe shock index (SI) is commonly used as an indicator of PPH severity and urgency and reported to be more useful than vital signs.15, 16 In Japan, guidelines and obstetric emergency workshops such as the Japan Maternal Lifesaving System Promotion Council (JCIMELS) and Advanced Life Support in Obstetrics (ALSO) recommend considering transfer to a higher-level medical institution for SI of 1.0 or higher, and the patient should be transferred to a higher-level medical institution for SI of 1.5 or higher.7, 17 Thus, the SI is an important indicator of the severity of PPH. Therefore, in this study, we examined the SI at the time of the transfer request and at the time of arrival at the hospital, as well as the change in SI before and after transfer.
Cardiac arrest casesCases in which cardiac arrest occurred during or after transport were considered separately. The SI at the time of transfer request and transfer time were examined to determine whether there was a need for improvement in the transfer process.
Statistical analysisWe used descriptive statistics with all variables in this study. First, we calculated the median and interquartile range for age (years), birth to transfer request (min), transfer time (min), time from transfer request to emergency call (min), time from emergency call to arrival of the emergency medical team (EMT )(min), time from arrival of EMT to beginning of transport (min), time from beginning of transport to hospital arrival, SI at the time of transfer request, and SI at the time of hospital arrival. We also calculated frequencies and percentages of each diagnosis (tonus, trauma, tissue, and thrombin), cardiac arrest on arrival, and poor neurological prognosis. All analyses were carried out using JMP® 15 (SAS Institute Inc., Cary, NC).
RESULTS Patient selectionDuring our study's 4-year period, a “Puerperium call” was issued in 101 cases, 11 of which did not meet the definition of PPH. Among these cases, 11 had insufficient data; thus, 79 cases were finally included in the study (Fig. 1).

Flow of patient selection in this study of patients with postpartum hemorrhage (PPH) transferred to hospital from a perinatal care facility.
Patients' characteristicsThe median (interquartile range [IQR]) age was 29 (33–37) years. Trauma was the most common diagnosis in 36 cases (46%), tonus in 27 (34%), and bleeding from tissue in 16 cases (20%). No cases were transported with thrombin. The median (IQR) of transfer time was 53 (47–64) min. The most time-consuming breakdown of transfer time was from beginning of transport to hospital arrival with a median (IQR) of 17 (13–20) min. The next longest time was from transfer request to emergency call with a median time of 15 (8–22) min. The median (IQR) SI at the time of transfer request was 0.87 (0.67–1.10) and at the time of arrival at our hospital was 0.85 (0.69–1.13). There were no deaths, but two cases of cardiac arrest on arrival and one of poor neurological prognosis (Table 1).
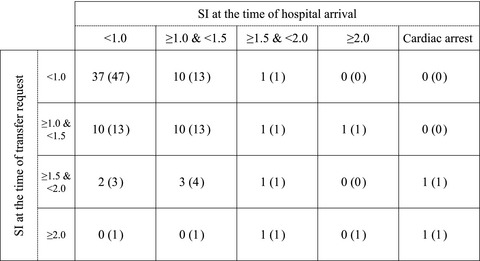
Table 1. Characteristics of patients with postpartum hemorrhage transferred to hospital from a perinatal care facility Characteristics Frequency (%) or median (IQR) Age 33 (29–37) Diagnosis Tonus 27 (34) Trauma 36 (46) Tissue 16 (20) Thrombin 0 (0) Transfer requests during the day shift 22 (28) Birth to transfer request (min) 186 (99–285) Transfer time (min) 53 (47–64) From transfer request to emergency call 15 (8–22) From emergency call to arrival of EMT 6 (5–8) From arrival of EMT to beginning of transport 14 (12–17) From beginning of transport to hospital arrival 17 (13–20) Shock index at the time of transfer request 0.87 (0.67–1.10) Shock index at the time of hospital arrival 0.85 (0.69–1.13) Cardiac arrest on arrival 2 (3) Mortality 0 (0) Poor neurological prognosis 1 (1) EMT, emergency medical team; IQR, interquartile range. Shock index before and after transferThirty-seven of the cases (47%) had SI less than 1.0 both before and after transfer. In 70 of the cases (89%), the request for transfer was submitted before the patient reached SI of 1.5, which is the criteria for transfer per guideline. There were seven severe cases with SI of 1.5 or more at the time of arrival, some with high SI and some with low SI at the time of transfer request. Two cases with cardiac arrest at hospital arrival already had SI of at least 1.5 at the time of transfer request (Fig. 2).

Classification of patients with postpartum hemorrhage according to the shock index (SI) at the time of transfer request and arrival at the hospital. Data are shown as the number of cases (percentage).
Cardiac arrest casesTwo cases of cardiac arrest occurred, both due to uterine rupture; they were resuscitated after arrival at the hospital, and treated with total hysterectomy and endovascular treatment. Case 1 had a transfer time of 65 min and an SI of 1.71 at the time of transfer request, and was discharged home on foot on day 22 of admission. Case 2 had a transfer time of 44 min and an SI on transfer of 3.50. Although the patient was resuscitated, the neurological prognosis was poor due to hypoxic encephalopathy (Table 2).
Table 2. Comparison of cardiac arrest cases among patients with postpartum hemorrhage transferred to hospital from a perinatal care facility Transfer time (min) From transfer request to emergency call (min) From emergency call to arrival of EMT (min) From arrival of EMT to beginning of transport (min) From beginning of transport to hospital arrival (min) Shock index at the time of transfer request Shock index at the time of hospital arrival Median of all cases (IQR) 53 (47–64) 15 (8–22) 6 (5–8) 14 (12–17) 17 (13–20) 0.87 (0.67–1.10) 0.85 (0.69–1.13) Case 1 65 34 3 13 15 1.71 Cardiac arrest Case 2 44 −1 9 23 16 3.50 Cardiac arrest EMT, emergency medical team; IQR, interquartile range. DISCUSSIONIn this study, we described the transport time and timing of transfer of postpartum hemorrhage cases to higher medical institutions in urban areas. We found that patients with PPH were transferred to a higher medical institution within a median (IQR) of 53 min (47–63 min). In 89% of cases, the transfer request was made before the SI reached 1.5. The median (IQR) SI before and after transfer was 0.87 (0.67–1.10) and 0.85 (0.69–1.13), respectively, with no worsening of SI. In addition, there were two cases of cardiac arrest during transport.
In 90% of the PPH cases transferred to our hospital, the transfer was done before SI was greater than 1.5, which is recommended by the guidelines. It has been reported that death occurs within 1–3 h from the first sign of PPH.6 The median (IQR) transfer time to our hospital was 53 min (47–63 min), and there was no increase in the median SI before and after transfer. This result suggests that patients were transferred to a higher medical institution at an appropriate time before the increase in blood loss and hemorrhagic shock progression worsened the SI. One of the reasons is the cooperative relationship in the community, and that referring doctors request transport at the right time. We aim to reduce the hurdle of transfer by building effective interpersonal relationships with the local hospital staff and educating them on PPH handling through the hosting of JCIMELS in the hospital. In 90% of cases, the request for transfer was submitted before the patient reached an SI of 1.5, which is the criteria for transfer per guideline. This could be a result of our efforts, and also because the city of Yokohama, where our hospital is located, has an extensive transportation network and ample medical facilities that shorten the duration of ambulance transport. In Yokohama City, the average time from the beginning of transport to arrival is 9.2 min, shorter than the national average of 11.6 min.18, 19
Two patients had cardiac arrest during transfer; thus, it is important not only for a referring physician to request transport at the appropriate time, but also to shorten the transport time. The transfer time was divided into several categories: (i) time from transfer request to emergency call, (ii) time from emergency call to arrival of the emergency team, (iii) time from arrival of the emergency team to beginning of transport, (iv) time from beginning of transport to patient arrival. Compared to the average of all emergency transports in Yokohama City, categories (ii) and (iii) were shorter.19 However, category (iv), with a median (IQR) of 17 min (13–20 min), was longer than the average 9.2 min in Yokohama City.18 This time is difficult to shorten because critically ill patients are transported from a wide area. However, it may be possible to shorten category (i). In fact, in one of the cases of cardiac arrest during transport the SI at the time of the request for transfer was 1.71, which required immediate transport, but (i) took 34 min (Table 2). The delay of (i) might be associated with the preparation of a referral letter and explanation to the patient and family. Eliminating the need for referral letters could reduce this time. In addition, our hospital, which operates a doctor car service, is considering introducing a system in which emergency physicians and obstetricians visit the obstetrics hospital and perform resuscitation or make an emergency call as soon as a transport request is received.
Our study had a few limitations. First, it was a single-center, retrospective study. There are large regional differences in transportation time, and it is desirable to undertake comparisons in each region. Furthermore, our sample size was limited. We also could not examine the treatment by the referring doctor. Most patients were transferred from small hospitals with one or two obstetricians, but some were transferred from higher medical institutions for endovascular treatment or emergency surgery, and their condition might not have worsened during transportation because they had received adequate treatment by their referring doctors.
CONCLUSIONSThe study described the transport time and timing of transfer of PPH cases to higher medical institutions in urban areas. We found that patients with PPH were transferred to a higher medical institution in less than 1 h. In addition, two cardiac arrests occurred during transport.
ACKNOWLEDGMENTSWe thank the staff at the Advanced Critical Care and Emergency Center and the Perinatal Center for Maternity and Neonates, Yokohama City University Medical Center, for their cooperation.
DISCLOSUREApproval of the research protocol: Ethics Committee of Yokohama City University (approval no. B200700036).
Informed consent: N/A.
Registry and registration no. of the study/trial: N/A.
Animal studies: N/A.
Conflict of interest: None.
ETHICS APPROVALThe protocol for this research project was approved by a suitably constituted Ethics Committee, and conforms with of the Declaration of Helsinki.
留言 (0)