
記住我

There have been many studies on the spinal morphology and alignment of asymptomatic Asian and Western subjects1-6. many studies have revealed the tremendous help of sagittal spine parameters on mechanisms and therapeutic strategies for spinal disease1, 3, 6. Spinopelvic alignment parameters are closely correlated with spine typing and spinal sagittal curve3. Pelvic incidence (PI) as a widely used anatomical parameter increases in childhood and adolescence, but is stable in adulthood7. There is an intrinsic relationship between PI, pelvic tilt(PT) and sacral slope (SS), namely, PI = PT + SS. PT and SS are also regarded as forceful indicators for determining pelvic location and are strongly related to spine sagittal curves8. Matching lumbar lordosis (LL) to pelvic incidence (PI) to within 10° is one of the key radiographic components associated with successful outcome in adult spinal deformity surgeries9. Therefore, one of the purposes of the surgeon's corrective surgery is to obtain an adequate LL to achieve a harmonious spinopelvic alignment (PI-LL 10°or less). In addition, occipitocervical alignment, cervicothoracic alignment, cervical parameters, thoracic parameters, and lumbar parameters also play an important role in the diagnosis and treatment of spinal imbalance or spinal diseases at their respective segments2, 4, 6, 8, 10.
However, many of these studies do not consider variation in the number of vertebrae. Most people have 12 thoracic vertebrae (TVs) (T1–T12) and five lumbar vertebrae (LVs) (L1–L5). However, some asymptomatic individuals have variation in the number of TVs or LVs, including a reduced number of TVs due to bilateral 12th rib loss and lumbosacral transitional vertebrae4, 11-15. The lumbosacral transitional vertebra (LSTV), which was first observed by Bertolotti in 1917, is the most frequent malformation of the lumbosacral region15. It is defined as either lumbarization of the highest sacral spinal segment (six LVs) or sacralization of the most inferior lumbar spinal segment (four LVs).
Yokoyama et al.4 noted six LVs among normal volunteers, and identified differences in total sagittal parameters between six LVs and five LVs. Benlidayi et al.15 reported that patients with LSTV had less sacral tilt, i.e., a more vertical sacrum. However, they ignored the fact that sometimes an increase in the number of LVs can be accompanied by a decrease in the number of TVs. That is, there are individuals with 11 TVs and six TVs at the same time.
There still remains a paucity of literature regarding global spinal parameters for individuals with variation in the number of vertebrae. Therefore, the purpose of this study is: (i) to explore the prevalence of 11 TVs, four LVs and six LVs among asymptomatic Chinese volunteers; (ii) to present the global spinal parameters from volunteers in eastern China; and (iii) to analyze the changes of global spinal parameters caused by variation of the number of lumbar and thoracic vertebrae.
Materials and Methods Study DesignThis study was performed in accordance with the principles of the Declaration of Helsinki and was approved by our institutional review board (2016 Clinical Research Ethics Review No. 10). A cohort of 427 asymptomatic Chinese adults was recruited between 27 May 2016 and 13 April 2018. The exclusion criteria were as follows: age <18 years; lameness or unequal length of lower limbs; apparent scoliosis (Cobb angle >10° in coronal position); history of trauma of the spine, pelvis, or lower extremity; history of hip or knee arthroplasty and spine, pelvis, or lower limb surgery; complaints of back pain, neck pain, or limb numbness caused by degenerative diseases of the spine, such as disc herniation, spinal canal stenosis, and lumbar spondylolisthesis; strabismus or torticollis affecting balance; history of neuromuscular disorders or congenital abnormalities; or pregnancy or preparation for pregnancy. All individuals were of Chinese ethnicity. Informed consent was obtained from each volunteer prior to enrollment in this trial. The volunteers were given a free full-spine photograph and X-ray report, including the chest, lungs, spine, and abdomen, in return for their participation.
Forty volunteers who had an incomplete number of X-ray images or who met the exclusion criteria after radiography were excluded. Ultimately, 389 asymptomatic subjects were included in the study.
Radiographic AnalysesAnteroposterior and lateral radiographs were acquired for all volunteers with their arms in the fists-on-clavicles position, the head in the neutral position, and the knees and hips fully extended. The radiographs were examined by a spine surgeon and a radiologist who had independently reviewed several hundred whole-spine images prior to this review. The following parameters were measured from each lateral whole-spine standing radiograph: occipital slope (OS), C0–2 Cobb angle (C0–2 Cobb), C2–7 Cobb angle (C2–7 Cobb), C1–7 Cobb angle (C1–7 Cobb), C2–7 sagittal vertical axis (C2–7 SVA), absolute rotation angle C2–C7 (ARA C2–C7), cervical tilt, cranial tilt, T1 slope (TS), neck tilt (NT), thoracic inlet angle (TIA), thoracic kyphosis (TK), C6–T5 Cobb angle (C6–T5 Cobb), T5–12 Cobb angle (T5–T12 Cobb), Ll Slope (LS), L1–5 Cobb angle (L1–5 Cobb), sacral slope (SS), pelvic tilt (PT), pelvic incidence (PI), and C7 sagittal vertical axis (C7 SVA). Examples of the parameters have previously been as described2, 4, 16.
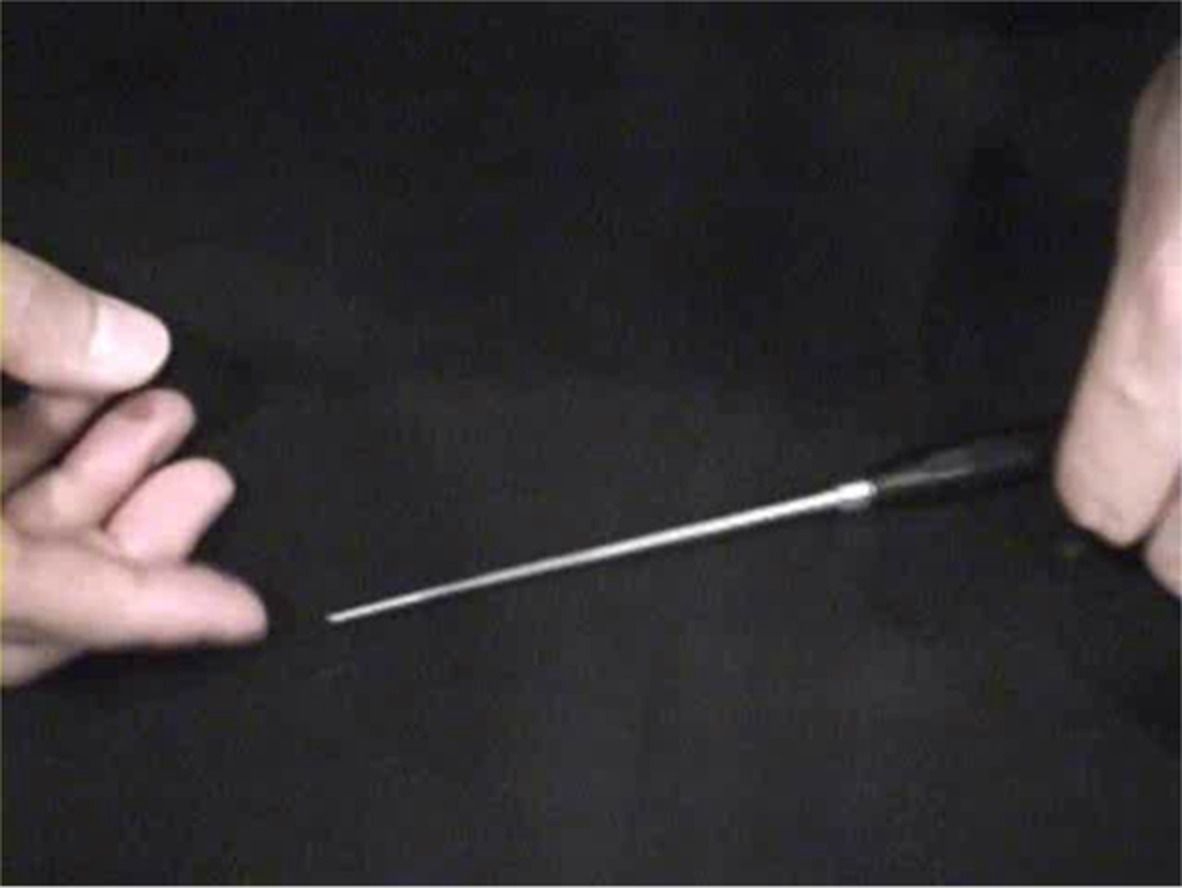
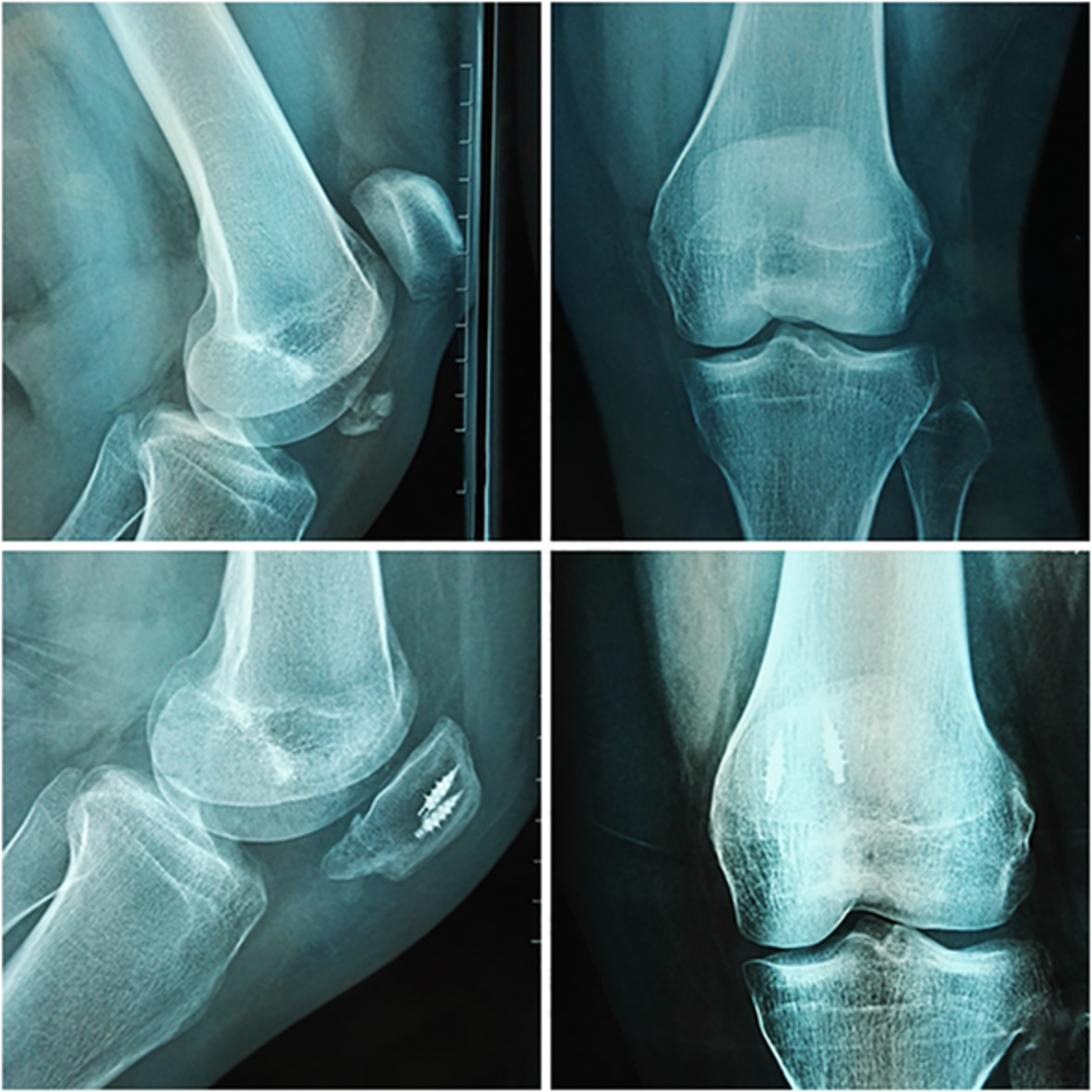
All vertebrae with rib attachments, including bilateral or unilateral ribs, were counted as TVs. A vertebra was considered to be at the LV level only if it was not attached to the ribs17. The key to differentiating whether there were only 11 TVs was to distinguish the first lumbar transverse process from the 12th rib. Generally, the well-developed 12th rib can be viewed in lateral X-ray film. However, if the rib is not fully developed or too small, it is difficult to distinguish it from the first lumbar transverse process in either the lateral or posteroanterior view. It is possible to determine whether it is the 12th rib or the first lumbar transverse process from rib vertebrae angle (RVA) and the angle between the first lumbar transverse process and vertebral body (opening angle), and the presence or absence of “lesser rib fossa” in the posteroanterior view (Fig. 1). Spinal parameter measurements in individuals with 11 TVs were performed using the T11 as an indicator instead of T12.

An example of a unilateral 12th rib to distinguish the poorly developed 12th rib from the first lumbar transverse process. (A) The poorly developed rib could not be viewed in the lateral X-ray image. (B) A smaller example of a unilateral 12th rib to distinguish the poorly developed 12th rib from the first lumbar rib vertebrae angle (RVA) between the rib and the anterior midline of vertebral body in the posteroanterior view. (C) There was a “lesser rib fossa” at the junction of ribs and vertebrae in the posteroanterior view.
Individuals with four LVs were determined to have only four vertebrae and five intervertebral discs between the 12th thoracic vertebra and the sacrum. Spinal parameter measurements in individuals with four LVs were performed using L4 as an indicator instead of L5.
L6 was determined as present if all of the following criteria were fulfilled4, 18: the L6 vertebral body appeared square or rectangular on lateral X-ray images, and obvious, well-formed disc material extending along the entire anteroposterior length of the sacrum was present between L6 and the sacral segment. Spinal parameter measurements in individuals with six LVs were performed using L6 as an indicator instead of L5.
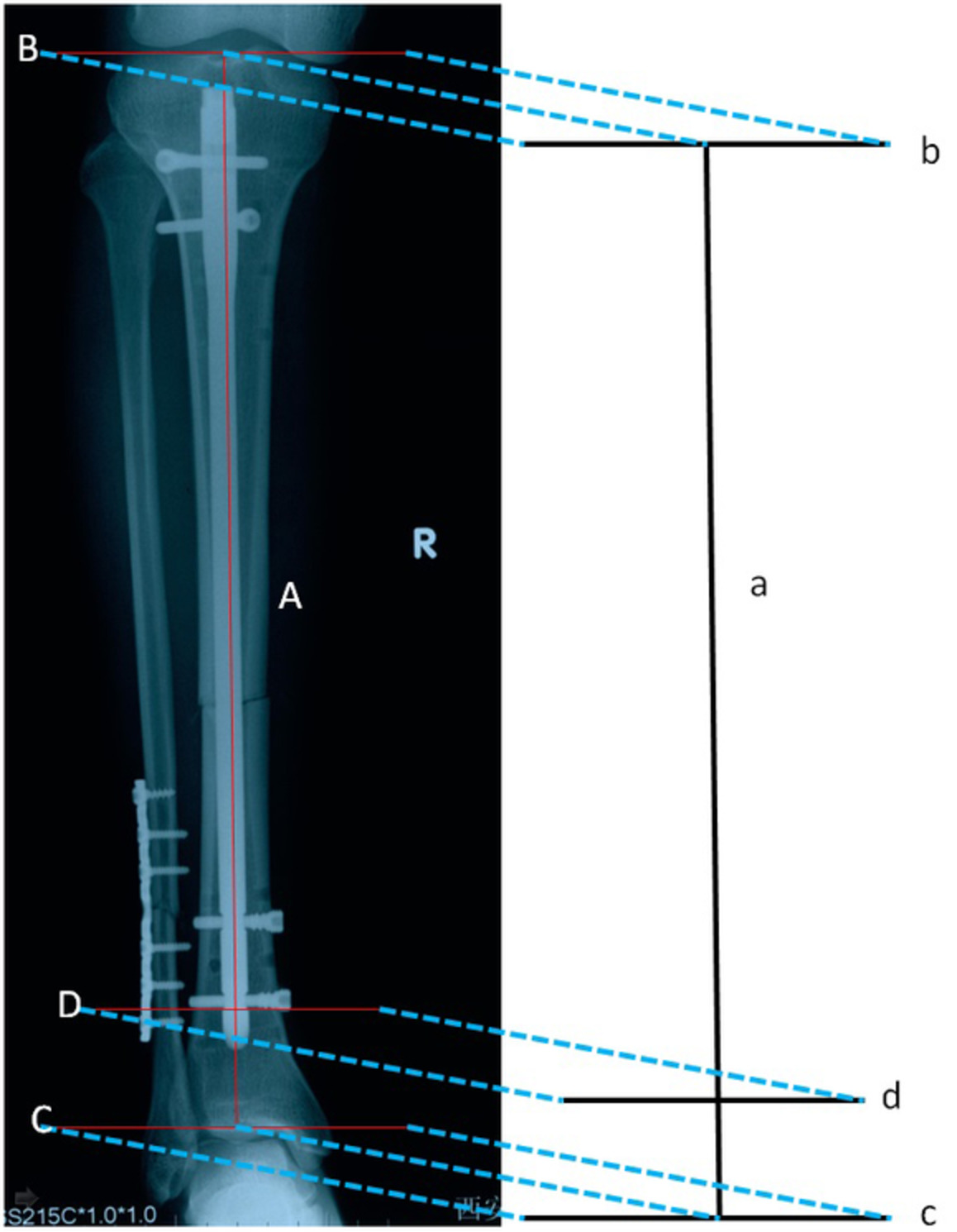
The definition, measurement method and clinical significance of each parameter are shown in Table 1. The measurement method of part of global spinal parameters (positive sign) is shown in Fig. 2.
TABLE 1. Definition, measurement method and clinical significance of the parameters Parameter Description and definition Clinical significance Occipital Slope (°) The angle between McRae's line and the horizontal line Craniocervical parameters(reflecting occipital tilt) C0-2 Cobb angle (°) The angle between McRae's line and the lower endplate of C2 Cervical parameters(reflecting cervical curvature) C2-7 Cobb angle (°) The angle between the C2 lower endplate and the C7 lower endplate C1-7 Cobb angle (°) The angle between the line linking the inferior anterior arch and the inferior posterior arch of the atlas and the C7 lower endplate. C2-7 SVA (mm) The distance between a plumbline dropped from the centroid of C2 and the posterior superior corner of C7 ARA C2–C7 (°) The angle between Jackson's physiologic stress lines drawn at the C2 and C7 posterior body margins Cervical tilt (°) The angle between two lines, both originating from the center of the T1 upper endplate, with one being vertical to the T1 upper endplate and the other passing through the tip of the dens Cervicothoracic parameters;TS = cervical tilting pluscranial tilting(reflecting inclination of the cervical spine) Cranial tilt (°) The angle between two lines, both originating from the center of the T1 upper endplate, with one passing through the dens and the other being a vertical line Tl Slope (°) The angle between a horizontal plane and a line parallel to the T1 upper end plate Thoracic Inlet Parameters;TIA = TS + NT.(To reflect cervical and thoracic junction curvature andpredict physiological alignment of the cervicalspine.) Neck Tilt (°) The angle between two lines both originating from the upper end of the sternum, with one being a vertical line and the other connecting to the center of the T1 upper endplate Thoracic Inlet Angle (°) The angle between a line originating from the center of the T1 upper endplate and perpendicular to the T1 upper endplate and a line from the center of the T1 upper endplate and the upper end of the sternum C6-T5 Cobb angle (°) The angle between the superior endplate of C6 and the inferior endplate of T5 Thoracic parameters(reflecting Thoracicl curvature) T5-12 Cobb angle (°) The angle between the superior endplate of T5 and the inferior endplate of T12 Thoracic Kyphosis (°) The angle between the superior endplate of T1 and the inferior endplate of T12 Ll Slope (°) The angle between a horizontal plane and a line parallel to the L1 upper end plate Lumbar parameters(reflecting Lumbar curvature) L1-5 Cobb angle (°) The angle between the superior endplate of L1 and the inferior endplate of L5 Sacral Slope (°) The angle formed by a line drawn along the endplate of the sacrum and a horizontal reference Spinopelvic alignment.PI=SS + PT.(The important parameters basis ofRoussouly classification; To predictphysiological alignment of thethoracic and lumbar spine.) Pelvic Tilt (°) The angle formed by a line drawn from the midpoint of the sacral endplate to the center of the bicoxofemoral axis and vertical plumbline Pelvic Incidence (°) The angle formed by a line originating from the center of the sacral endplate and perpendicular to the S1 upper endplate and a line drawn between the center of the femoral head and the center of the sacral endplate PI-LL (°) Pelvic Incidence minus L1-5 Cobb angle Achieving a harmonious spinopelvicalignment (PI-LL 10°or less) is instructive for both long and short segment fusion for adult spinal deformity C7 SVA (mm) The horizontal offset from the posterosuperior corner of S1 to the vertebral body of C7 Sagittal balance parameters(Reflecting the sagittal balance of spine; The normal value is between plus and minus 50 mm)
Measurement methods of some spinal parameters.
Statistical AnalysisThe SPSS 19.0 statistical software package (SPSS, Chicago, IL) was used for statistical analyses. For comparison of parameters between the two groups, we applied the independent samples t test, Mann–Whitney U test, or chi square test as appropriate. All data are presented as the means ± standard deviations (SDs), and differences were considered statistically significant at P < 0.05.
Results Study Population and X-ray Images of Each GroupThe 389 volunteers ranged in age from 22 to 70 years, with a mean age of 42.5 years. They included 20 (5.1%) with 11 TVs, eight (2.1%) with four LVs, and 23 (5.9%) with six LVs. Eight individuals had an atypical number of both thoracic11 and lumbar6 vertebrae. No hemivertebra deformities were found in any of the volunteers. The spinal parameters for individuals with 11 TVs, four LVs, six LVs, and typical numbers of vertebrae are presented in Tables 2–5. Based on the above results, the volunteers were divided into five groups: 7C + 11T + 5L group (12 cases), 7C + 11T + 6L group (eight cases), 7C + 12T + 4L group (eight cases), 7C + 12T + 5L group (346 cases), and 7C + 12T + 6L group (15 cases). X-ray images of each group are shown in Fig. 3.
TABLE 2. Comparison of global alignment parameters between 11TVs or 6LVs and normal Parameter 7C + 12T + 5L 11TVs 6LVs Number (%) 346 (89.4%) 20 (5.1%) 23 (5.9%) Male/female 133/213 4/16 12/11 Age (years) 42.6 ± 13.2 41.6 ± 13.0 43.5 ± 13.7 BMI (kg/m2) 22.6 ± 2.8 21.1 ± 2.2* 22.2 ± 2.7 Occipital slope (°) 13.6 ± 7.3 14.3 ± 7.1 16.5 ± 6.8 C0-2 Cobb angle (°) 27.1 ± 8.1 26.3 ± 5.9 28.7 ± 9.2 C2-7 Cobb angle (°) 6.3 ± 10.9 4.33 ± 10.1 5.1 ± 12.0 C1-7 Cobb angle (°) 27.6 ± 11.2 26.1 ± 12.5 27.8 ± 12.3 C2-7 SVA (mm) 16.7 ± 8.5 13.2 ± 6.4 14.9 ± 8.5 ARA C2–C7 (°) 8.2 ± 10.5 7.6 ± 9.6 6.3 ± 12.9 Cervical tilt (°) 8.7 ± 10.8 9.8 ± 8.1 10.2 ± 8.0 Cranial tilt (°) 5.0 ± 4.8 4.6 ± 4.2 4.8 ± 5.4 Tl slope (°) 17.7 ± 6.2 16.0 ± 6.2 16.0 ± 7.1 Neck tilt (°) 52.1 ± 6.8 55.0 ± 8.1 51.6 ± 8.8 Thoracic inlet angle (°) 69.8 ± 8.2 70.9 ± 7.9 67.2 ± 10.1 C6-T5 Cobb angle (°) 9.8 ± 6.5 7.9 ± 5.3 10.0 ± 6.0 T5-12 Cobb angle (°) 21.8 ± 7.8 22.7 ± 8.7 19.6 ± 8.7 Thoracic kyphosis (°) 34.2 ± 9.2 33.3 ± 9.3 31.1 ± 9.7 Ll slope (°) 13.3 ± 5.4 14.5 ± 5.8 11.6 ± 4.9 L1-5 Cobb angle (°) 35.3 ± 9.9 37.5 ± 8.6 41.7 ± 10.3* Sacral slope (°) 38.2 ± 7.7 39.4 ± 6.6 41.6 ± 7.2* Pelvic tilt (°) 9.7 ± 6.2 10.4 ± 6.0 15.4 ± 8.9* Pelvic incidence (°) 47.3 ± 9.2 49.1 ± 10.6 56.6 ± 10.6* PI-LL (°) 11.9 ± 9.1 11.7 ± 9.0 15.0 ± 10.1 C7 SVA (mm) 10.3 ± 18.6 16.7 ± 33.5 14.8 ± 30.9 C, cervical vertebrae; L, lumbar vertebrae; LVs, lumbar vertebrae; T, thoracic vertebrae; TVs, thoracic vertebrae. “7C + 12T + 5L” stands for volunteers with normal number of vertebrae; PI-LL, pelvic Incidence minus L1-5 Cobb angle TABLE 3. Comparison of occipitocervical alignment and cervical balance parameters in different group Parameter 7C + 11T + 5L 7C + 11T + 6L 7C + 12T + 4L 7C + 12T + 6L 7C + 12T + 5L All Number (%) 12 (3.1%) 8 (2.1%) 8 (2.1%) 15 (3.9%) 346 (89.4%) 389 Male/female 1/11 3/5 3/5 9/6 133/213 149/240 Age (year) 39.3 ± 14.4 44.9 ± 10.7 42.9 ± 15.4 42.8 ± 15.4 42.6 ± 13.2 42.5 ± 13.3 BMI (kg/m2) 19.9 ± 2.2* 22.8 ± 1.5 21.8 ± 2.7 21.9 ± 3.1 22.6 ± 2.8 22.5 ± 2.8 Occipital slope (°) 13.8 ± 8.2 15.2 ± 5.5 17.8 ± 8.7 17.2 ± 9.5 13.6 ± 7.3 13.8 ± 7.4 C0-2 Cobb angle (°) 27.6 ± 5.3 24.3 ± 6.6 30.2 ± 10.9 31.0 ± 9.7 27.1 ± 8.1 27.2 ± 8.2 C2-7 Cobb angle (°) 2.0 ± 10.7 7.8 ± 8.8 4.6 ± 15.0 3.6 ± 13.4 6.3 ± 10.9 6.1 ± 11.0 C1-7 Cobb angle (°) 22.7 ± 13.7 31.2 ± 8.7 28.3 ± 15.5 26.0 ± 13.8 27.6 ± 11.2 27.5 ± 11.4 C2-7 SVA (mm) 13.0 ± 5.5 13.7 ± 8.0 16.2 ± 6.0 15.5 ± 8.9 16.7 ± 8.5 16.4 ± 8.4 ARA C2–C7 (°) 3.7 ± 8.9 13.4 ± 7.7 7.0 ± 11.8 2.54 ± 13.7 8.2 ± 10.5 7.9 ± 10.6 TABLE 4. Comparison of cervicothoracic alignment and thoracic parameters in different group Parameter 7C + 11T + 5L 7C + 11T + 6L 7C + 12T + 4L 7C + 12T + 6L 7C + 12T + 5L All Number (%) 12 (3.08%) 8 (2.06%) 8 (2.06%) 15 (3.86%) 346 (89.4%) 389 Male/female 1/11 3/5 3/5 9/6 133/213 149/240 Cervical tilt (°) 8.5 ± 9.2 11.8 ± 6.3 14.3 ± 8.8 9.3 ± 8.9 8.7 ± 10.8 8.9 ± 10.5 Cranial tilt (°) 4.5 ± 3.6 4.7 ± 5.3 3.9 ± 7.0 4.9 ± 5.6 5.0 ± 4.8 4.9 ± 4.8 Tl slope (°) 15.3 ± 6.6 16.9 ± 5.8 19.8 ± 9.6 15.6 ± 7.9 17.7 ± 6.2 17.5 ± 6.3 Neck filt (°) 53.8 ± 6.5 56.8 ± 10.3 56.9 ± 10.7 48.8 ± 6.8 52.1 ± 6.8 52.2 ± 6.9 Thoracic inlet angle (°) 69.3 ± 6.6 73.3 ± 9.6 76.6 ± 11.4* 63.9 ± 9.0* 69.8 ± 8.2 69.7 ± 8.3 C6-T5 Cobb angle (°) 5.7 ± 4.6* 11.3 ± 4.4 9.5 ± 5.7 9.2 ± 6.7 9.8 ± 6.5 9.7 ± 6.5 T5-12 Cobb angle (°) 25.4 ± 7.0 18.6 ± 9.8 23.0 ± 10.7 20.2 ± 8.5 21.8 ± 7.8 21.8 ± 7.9 Thoracic kyphosis (°) 35.0 ± 7.8 30.7 ± 11.1 36.8 ± 9.6 31.3 ± 9.3 34.2 ± 9.2 34.0 ± 9.2 TABLE 5. Comparison of spinopelvic alignment and lumbar parameters in different group Parameter 7C + 11T + 5L 7C + 11T + 6L 7C + 12T + 4L 7C + 12T + 6L 7C + 12T + 5L All Number (%) 12 (3.08%) 8 (2.06%) 8 (2.06%) 15 (3.86%) 346 (89.4%) 389 Male/female 1/11 3/5 3/5 9/6 133/213 149/240 Ll Slope (°) 16.6 ± 5.5 11.4 ± 5.1 13.5 ± 4.2 11.7 ± 4.9 13.3 ± 5.4 13.3 ± 5.4 L1-5 Cobb angle (°) 37.3 ± 6.1 37.7 ± 11.9 32.9 ± 8.5 43.8 ± 9.0* 35.3 ± 9.9 35.6 ± 10.0 Sacral slope (°) 38.1 ± 3.7 41.3 ± 9.5 37.6 ± 6.2 41.8 ± 6.1* 38.2 ± 7.7 38.4 ± 7.6 Pelvic tilt (°) 8.6 ± 6.1 13.0 ± 5.1 4.5 ± 5.4* 16.6 ± 10.4* 9.7 ± 6.2 10.0 ± 6.6
留言 (0)