
記住我

Cervical ossification of the posterior longitudinal ligament (OPLL) is defined as a degenerative disease with the characteristics of calcification of the posterior longitudinal ligament in the cervical spine, which may result in cervical myelopathy due to the compression of spinal cord or nerve roots. As reported, it is more susceptible for Asian and middle-aged populations1-3. Patients usually develop various degrees of neurological symptoms, such as paresthesia of limbs and trunk, motor paralysis, and bladder and rectal dysfunction, and their OPLL may progress gradually. Long-term follow-ups have shown that the ossification progressed laterally for 42% patients and longitudinally for up to 86% patients4. Therefore, surgical intervention would be considered in their course inevitably, especially for those with progressive myelopathy.
However, the ideal operative strategy for OPLL has always been a controversial issue. Posterior approach, such aslaminectomy and laminoplasty, can enlarge the spinal canal volume with indirect decompression of the compressed spinal cord and drift the spinal cord dorsally. On the one hand, it is commonly recommended for patients with multilevel OPLL (more than three levels) and excellent cervical curvature (negative K-line). On the other hand, the viewpoint has been universally acknowledged that anterior approach surgery outperformed posterior approach with respect to the postoperative neural function, particularly for patients with canal-occupying ratio greater than 50%–60% and with kyphotic cervical curvatures. However, the anterior approach, such as anterior cervical discectomy and fusion (ACDF) and anterior cervical corpectomy and fusion (ACCF), is challenging with a more complex procedure and a higher risk of complications5-9.
OPLL more than three levels cannot be managed well by traditional anterior decompression surgery. Recently, our team has proposed a new surgical technique named anterior controllable antedisplacement and fusion (ACAF) which overcome such difficulties. In this technique, anterior vertebral bodies were partly resected and the remaining vertebrae-OPLL complex (VOC) was hoisted via a plate-screw system. By this method, we not only achieved more satisfactory outcomes, but also extended the indication of the anterior approach retaining the OPLL and vertebrae10. As our previous reports, ACAF provided adequate decompression of the spinal cord and better outcomes compared with conventional ACCF in the treatment of severe cervical OPLL and cervical stenosis11-14. We assume that this is partly due to the fact that ACAF has a wider range of decompression than conventional anterior approach, resulting in adequate decompression of the spinal cord and nerve roots.
In recent anatomic research, the safety of ACAF surgery in terms of the occurrence of vertebral artery injury during the slotting procedure was verified15. However, its safety and availability of neuroldecompression have never been verified by the anatomic method. The entrance zone of the intervertebral foramina is the narrowest part, however, the nerve root crossing this tunnel is the largest part16, 17. Thus, neurothlipsisusually occurs and causes cervical radiculopathy. The spinal cord decompression is hardly neglected during traditional anterior approach, but decompression of the entrance zone of the intervertebral foramina and takeoff points of nerve roots may be inadequate. For example, the takeoff points may be decompressed inadequately in ACDF as the takeoff points are usually located cranially when compared with the corresponding intervertebral foramen, and the entrance zone of the intervertebral foramina cannot be managed adequately in ACCF, especially for the unskilled surgeons. These deficiencies can be avoided by the ACAF technique theoretically, however, only radiographic evaluation has been employed in previous research. Thus, anatomic evidence should be elucidated well.
The spinal nerve is located at the lateral and posterior sides of uncovertebral joint, and removal of the hyperplastic uncovertebral joint plays an important role in decompression of the nerve root. Several techniques have been introduced to deal with the uncovertebral joint during traditional anterior methods. For example, Jho et al.18-20 proposed anterior cervical foraminotomy through completely resecting the uncovertebral joint, and others21, 22 modified it by preserving the lateral margin of the uncovertebral joint to avoid vertebral artery injury. In ACAF surgery, uncovertebral joints are usually resected safely and get a similar decompression effect compared with these techniques. In fact, tip of uncovertebral joint is recommended as the landmark for slotting in ACAF. Even in such cases with severe foraminal stenosis, wedging slotting15 would be preferred to make sure of adequate decompression on the cervical nerve roots. Thus, it is also crucial for surgeons to understand the anatomical relationship between the slotting and the spinal nerve and cervical intervertebral foramina thoroughly during ACAF surgery.
Above all, we started this study through the cadaveric and radiologic methods. The purpose of this study was to: (i) provide cadaveric evidence to verify that the adequate decompression effect could be achieved in ACAF surgery; (ii) demonstrate that ACAF surgery could offer a novel revision strategy for traditional ACCF; and (iii) describe the morphology and intradural pathways of rootlets in the cervical spine.
Materials and Methods Cadaveric SampleFor this study, three fresh cadaveric spines (two males and one female, death within 3 months), ages at death ranged from 37 to 49 years (mean 42 years) were examined. To study the physiologic relation between the bone and nerve tissues, all specimens with severe deformities and traumas were excluded. The cadaveric specimens of the cervical spine from the atlas to the first thoracic vertebra were obtained.
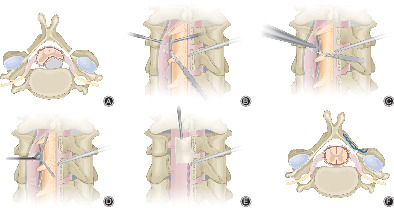
Anatomic EvaluationAll of the cadaveric specimens underwent vertical slotting in the medial of uncinated process(UP) tip bilaterally on the basis of ACAF surgical procedure (Fig. 1A)10. The C4, C5, C6 vertebrae were removed after bilateral osteotomies. Then the dural sac corresponding to the vertebrae was removed anteriorly to acquire the spinal cord and nerve rootlets as shown in Fig. 1B,C.

Anatomic schematic figure of the relationship between ACAF and spinal cord, nerve root and cervical intervertebral foramina. (A) Anterior view of specimen after cervical discectomies. a. the conventional slotting line in ACAF surgery. (B) Anterior view of specimen after removing the C4, C5, C6 vertebrae and corresponding dural sac. The shadow areas indicated the paths of respective ventral rootlet from the origin of ventral rootlet to intervertebral foramina. (C) Oblique view of specimen after removing the C4, C5, C6 vertebrae and corresponding dural sac. The arrows indicated the locations of entrance zones of respective intervertebral foramina. (D) Placing the titanium mesh after anterior cervical corpectomy according to the slot width in ACAF surgery procedure.
Four anatomic parameters were evaluated after removing the C4, C5, C6 vertebrae and corresponding dural sac as follows (Fig. 2):

Schematic figure of anatomic parameters. (A) width of groove. (B) distance between the bilateral origins of ventral rootlets. (C) length of ventral rootlet from the origin to the intervertebral foramina. (D) descending angle of ventral rootlet.
Width of Groove and Distance between the Bilateral Origins of Ventral Rootlets (DVR)Width of groove was measured as the distance between bilateral lateral walls of groove. DVR was measured as the distance between bilateral medial edges of origins of ventral rootlets. They were used to evaluate the decompression effect of ACAF technique on the origin of ventral rootlet.
Length of Ventral Rootlet from the Origin to the Intervertebral Foramina (LVR) and Descending Angle of Ventral RootletLVR was measured as the distance between the origin of ventral rootlet and corresponding the intervertebral foramina. Descending angle of the ventral rootlet was measured as the angle between the vertical line and the line running parallel to the ventral rootlet. They were used to evaluate the decompression range of ACAF technique on the running part of ventral rootlet and recognize the morphology and pathway of spinal nerve in the spinal canal.
Clinical SampleThis study was approved by the institutional review board of our hospital, and all included patients signed the informed consent. The inclusion criteria were as follows: (i) diagnosed with cervical OPLL by X-ray and computed tomography (CT); (ii) diagnosed with cervical stenosis by X-ray and magnetic resonance imaging (MRI); (iii) presented with neurologic dysfunction and accepted surgery of ACAF or ACCF; and (iv) compression segments extended two or more. The exclusion criteria were as follows: (i) history of injury; (ii) cervical congenital deformity; and (iii) nerve root compressed by the superior articular process, the ligamentum flavum or the periradicularfibrous tissues posteriorly.
Clinical data of 47 consecutive patients treated for cervical OPLL and cervical stenosis from March 2017 to March 2018 were retrospectively reviewed. Among them, 21 patients underwent ACAF surgery and ACCF surgery was performed on 26 patients. The operations were performed by the same professional spine surgeon.
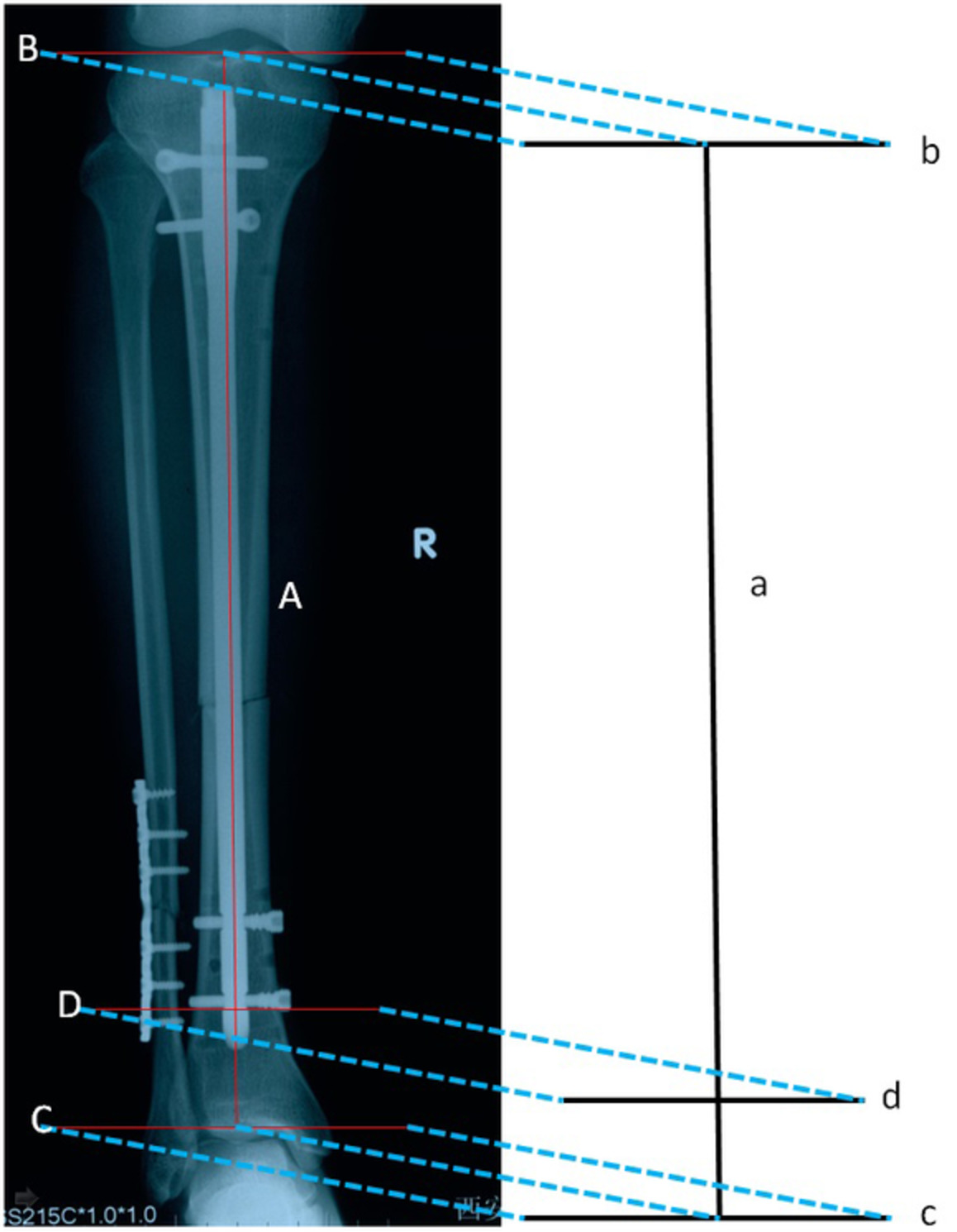
Radiographic EvaluationCT scans and MRIs were obtained on the third day after operation in all postoperative patients. All radiographs were independently analyzed by three experienced spine surgeons on both sides of cervical vertebras in operative levels through MIMICS software. Three postoperative radiographic parameters were evaluated (Fig. 3).

Schematic figures of radiographic parameters. (A) Postoperative radiographic parameter in CT: a. decompression width in ACAF. The arrows indicated the bilateral entrance zones of intervertebral foramina. (B) Postoperative radiographic parameter in MRI: b. segmental transverse diameter of spinal cord in ACAF.
Decompression Width and Transverse Diameter of Spinal CordDecompression width was measured as the distance between the bilateral lateral walls of groove on cross-sectional CT image. Transverse diameter of spinal cord was calculated on cross-sectional MRI image. They were used to compare the decompression effect of ACAF and ACCF surgery on the takeoff point of the nerve root.
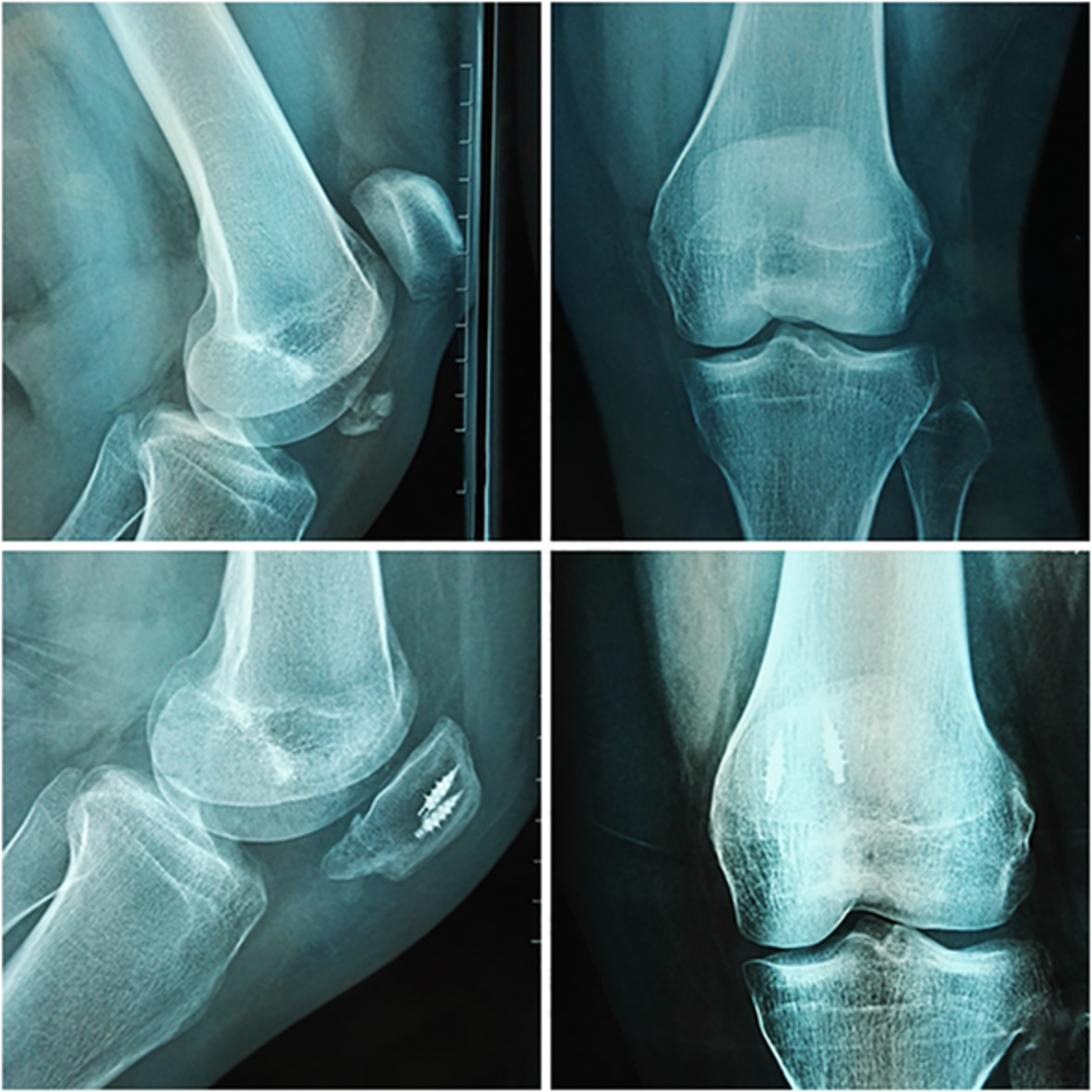
Satisfaction Rate of Decompression at the Entrance Zone of Intervertebral ForaminaThis was investigated on a cross-sectional CT image. The satisfaction standard of decompression at the entrance zone of intervertebral foramina was defined based on the condition of the posterior UP base and medial cortex of cervical pedicle. It was positive when the posterior UP base or medial cortex of cervical pedicle was removed, and was negative when posterior UP base and medial cortex of cervical pedicle were left in situ (Fig. 4). The satisfaction rate was defined as the positive number divided by the total number. It was used to evaluate the decompression effect of ACAF on the cervical intervertebral foramina and running part of the nerve root.

Radiographic satisfaction standard of decompression at the entrance zone of intervertebral foramina. (A) Positive: A1: bilateral posterior UP bases and part of the right medial cortex of pedicle were resected in ACAF surgery. A2: bilateral posterior UP bases were resected in ACCF surgery. (B) Negative: B1: the left posterior UP base was resected, but the right posterior UP base was not resected adequately in ACAF surgery. B2: bilateral posterior UP bases and medial cortex of cervical pedicles were remained in ACCF surgery. The arrows indicated the bilateral entrance zones of intervertebral foramina.
Statistical AnalysisThe measured parameters are expressed as the mean ± SD. The chi square test was used to compare categorical variables. Unpaired t test was used to compare continuous data between ACAF and ACCF group. t Paired t test was used to compare parameters between the left and right side. It was also performed for the comparison of the decompression width and the transverse diameter of spinal cord in each group. Statistical analysis was performed using SPSS21.0 (IBM, Armonk, NY, USA). P value <0.05 was considered as statistically significant.
Results Anatomic Outcomes Width of Groove and DVRThe groove created in ACAF surgery obviously included the bilateral origins of ventral rootlets in each level.(Width of groove: 20.4 ± 0.5 mm in C4 vertebra, 21.7 ± 0.5 mm in C5 vertebra, 23.0 ± 1.1 mm in C6 vertebra. DVR: 6.9 ± 0.2 mm in C5 ventral rootles, 7.5 ± 0.2 in C6 ventral rootlets, 7.2 ± 0.1 mm in C7 ventral rootlets, 7.5 ± 0.2 mm in C8 ventral rootlets)(Table 1).
TABLE 1. Anatomic parameters in the samples underwent ACAF surgery Anatomic parameter C4 C5 C6 C7 C8 Width of groove (mm) 20.4 ± 0.5 21.7 ± 0.5 23.0 ± 1.1 DVR (mm) 6.9 ± 0.2 7.5 ± 0.2 7.2 ± 0.1 7.5 ± 0.2 LVR (mm) (left) 13.1 ± 0.3 16.4 ± 0.4 17.7 ± 0.4 16.4 ± 0.3 LVR (mm) (right) 13.2 ± 0.2 16.4 ± 0.3 17.7 ± 0.4 16.4 ± 0.4 Descending Angle (°) (left) 33.7 ± 0.4 24.5 ± 0.5 20.4 ± 0.2 14.8 ± 0.2 Descending Angle (°) (right) 33.7 ± 0.4 24.6 ± 0.5 20.4 ± 0.2 14.9 ± 0.3 Data are expressed as the mean ± standard deviation. DVR, distance between the bilateral origins of ventral rootlets; LVR, length of ventral rootlet from the origin of ventral rootlet to the intervertebral foramina. LVR and Descending Angle of Ventral RootletThe length of the C5-C8 ventral rootlets showed increasing and the descending angles of ventral rootlets demonstrated decreasing gradually from the rostral to the caudal direction.(LVR: 13.1 ± 0.3 mm in the left of C5, 13.2 ± 0.2 mm in the right of C5, 16.4 ± 0.4 mm in the left of C6, 16.4 ± 0.3 mm in the right of C6, 17.7 ± 0.4 mm in the left of C7, 17.7 ± 0.4 mm in the right of C7, 16.4 ± 0.3 in the left of C8, 16.4 ± 0.4 mm in the right of C8. Descending angle: 33.7 ± 0.4° in the left of C5, 33.7 ± 0.4° in the right of C5, 24.5 ± 0.5° in the left of C6, 24.6 ± 0.5° in the right of C6, 20.4 ± 0.2° in the left of C7, 20.4 ± 0.2° in the right of C7, 14.8 ± 0.2° in the left of C8, 14.9 ± 0.3° in the right of C8). No differences were identified between left and right in terms of the LVR and the descending angle of ventral rootlet (Table 1).
Morphology and Intraduralpathways of the RootletsThe rootlets tended to be vertical from the rostral to the caudal direction as their takeoff points from the central thecal sac became higher and farther away from their corresponding intervertebral foramina gradually. The origin of the C5 ventral rootlet was located at the C4 vertebrae level. The C6 ventral rootlet originated at the C4-C5 disc level. The C7 and C8 ventral rootlets originated at the inferior border of C5 vertebrae and superior border of C6 vertebrae, respectively (Fig. 1B).
Clinical General ResultsThe ACAF group consisted of 21 patients (13 males and eight females, mean 60.7 ± 7.2 years in the range of 45 to 78). The ACCF group was composed of 26 patients (15 males and 11 females, mean 57.6 ± 6.3 years in the range of 42 to 73). There was no significant difference in the comparison of sex and age between ACAF and ACCF groups.
Radiographic Outcomes Decompression Width and Transverse Diameter of Spinal CordThe decompression width was significantly greater in the ACAF group in all levels (19.2 ± 1.2 mm vs 14.7 ± 1.2 mm in C3, P < 0.001, 21.3 ± 2.2 mm vs 15.4 ± 0.9 mm in C4, P < 0.001, 21.5 ± 2.1 mm vs 15.7 ± 1.0 mm in C5, P < 0.001, 21.9 ± 1.6 mm vs 15.9 ± 0.8 mm in C6, P < 0.001) (Table 3. The pair t test demonstrated that the decompression width was significantly greater than the transverse diameter of spinal cord in ACAF group (19.2 ± 1.2 mm vs 14.3 ± 1.8 mm in C3, P < 0.001, 21.3 ± 2.2 mm vs 15.1 ± 1.7 mm in C4, P < 0.001, 21.5 ± 2.1 mm vs 14.5 ± 1.9 mm in C5, P < 0.001, 21.9 ± 1.6 mm vs 14.2 ± 2.5 mm in C6, P < 0.001) (Table 4). Comparatively, there existed no difference in the ACCF group besides the C5 level (15.7 ± 1.0 mm vs 14.4 ± 2.0 mm in C5, P = 0.017) (Table 3).
Satisfaction Rate of Decompression at the Entrance Zone of Intervertebral ForaminaThe satisfactory rate of decompression at the entrance zone of intervertebral foramina was significantly greater in the ACAF group (100% vs 55.6% in the left of C3/4, P = 0.013, 94.4% vs 63.2% in the left of C4/5, P = 0.026, 94.4% vs 57.9% in the right of C4/5, P = 0.012, 100% vs 50.0% in the left of C6/7, P = 0.006), except for the right side of C3/4 and C6/7, and both sides of C5/6 on account of their small sample size. And the satisfactory rate tended to be better in the left side in the ACAF group (Table 2).
TABLE 2. Comparison of radiographic parameters between ACAF and ACCF groups Group Decompression width (mm) Satisfaction rate of decompression at the entrance zone of intervertebral foramina (%) C3 C4 C5 C6 C3/4(L/R) C4/5(L/R) C5/6(L/R) C6/7(L/R) ACAF 19.2 ± 1.2 21.3 ± 2.2 21.5 ± 2.1 21.9 ± 1.6 100/90.9 94.4/94.4 90.0/85.0 100/83.3 ACCF 14.7 ± 1.2 15.4 ± 0.9 15.7 ± 1.0 15.9 ± 0.8 55.6/55.6 63.2/57.9 68.4/68.4 50.0/50.0 t 8.106 10.7 11.01 9.635 6.111/3.3 4.976/6.279 2.783/1.509 7.500/2.540 P <0.001* <0.001* <0.001* <0.001* 0.013*/0.069 0.026*/0.012* 0.095/0.219 0.006*/0.111 Continuous datas are expressed as the mean ± standard deviation. TABLE 3. Comparison of decompression width and transverse diameter of spinal cord in both groups Radiographic Parameter ACAF ACCF C3 C4 C5 C6 C3 C4 C5 C6 Decompression width (mm) 19.2 ± 1.2 21.3 ± 2.2 21.5 ± 2.1 21.9 ± 1.6 14.7 ± 1.2 15.4 ± 0.9 15.7 ± 1.0 15.9 ± 0.8 Transverse Diameter of Spinal Cord (mm) 14.3 ± 1.8 15.1 ± 1.7 14.5 ± 1.9 14.2 ± 2.5 14.5 ± 1.3 14.8 ± 1.8 14.4 ± 2.0 14.9 ± 2.1 t 7.427 9.746 11.575 8.959 0.508 1.423 2.512 1.216 P <0.001* <0.001* <0.001* <0.001* 0.618 0.166 0.017* 0.255 Datas are expressed as the mean ± standard deviation. Case ReportA 63-year-old male diagnosed with cervical OPLL complained of gait disturbance and zonesthesia for 17 years. He received a C6 corpectomy in 2007, and the symptoms were not relieved after the primary surgery. In 2018, the remaining OPLL at C5-C6 and the adjacent degeneration (C4/5) was found during follow up, then ACAF was chosen for the revision surgery (Fig. 5). After removing the plate and screws, the anterior part of titanium mesh was ground off. Then discectomy in C4/5 and partly anterior resection of C5 vertebrae were performed. We then completed the vertical slotting on bilateral sides of C5 and outside the original titanium mesh. Subsequently, the wedge osteotomy was performed at the inferior border of the titanium mesh and the superior border of C7 vertebrae in accordance with our preoperative design. The C5 and titanium mesh were moved forward, and the bilateral entrance zones of intervertebral foramen were decompressed. As a result of the revision surgery, the spinal cord and nerve root received adequate decompression and his postoperative symptoms gradually relieved, while his JOA score increased from 9 preoperatively to 15 postoperatively.

A revision case of cervical OPLL with failed ACCF surgery. (A) Lateral X-ray showing the primary ACCF surgery with a C6 corpectomy. (B) sagittal CT of the cervical spine showing the ossification mass remained at C5-C6 (indicated by the arrows). (C) Sagittal MRI showing spinal cord compressed at C4/5 and C5/6. (D) Cross-sectional CT showing the remaining ossification mass located at bilateral posterior UP. The arrows indicated the stenosis of entrance zone of intervertebral foramen. (E) The morphology of the spinal cord on cross-sectional MRI was crescent. (F) Lateral X-ray showing a revision surgery with discectomy of C4/5 and antedisplacement of C5 and original titanium mesh. (G) Sagittal CT and (I) MRI demonstrating the sufficient decompression of spinal canal. (H) Coronal CT showing the slotting at bilateral sides of the original titanium mesh. (J) Cross-sectional CT showing the sufficient decompression at bilateral entrance zones of intervertebral foramen. (indicated by the arrows) (K) The morphology of the spinal cord on cross-sectional MRI was cylinder.
DiscussionThere is still some controversy on the treatment of OPLL. The anterior approach can achieve better clinical outcomes and long-term benefits by directly removing the anterior pathogenic structures5, 23-25. However, the procedure is more complex and associated with a higher risk of complications26, 27. When it comes to multilevel or severe OPLL, the anterior approach becomes riskier and more challenging, and the posterior approach becomes an alternative option6, 7, 9. Though a relatively simple technique with demanding and low complication rates, the posterior approach tends to be unsatisfactory due to the indirect decompression and spinal cord shifting dorsally, especially for severe OPLL or kyphotic cervical spine5, 9, 28. Previously, we proposed a novel technique named ACAF surgery for the treatment of severe OPLL, which showed lower surgery-relative complication rates and better clinical outcomes than the conventional anterior approach10-13. We contributed the good clinical outcomes to the adequate decompression of spinal cord and nerve root in ACAF surgery. This anatomic and radiographic investigation supported the hypothesis, and the revealed relationship among the slotting and cervical spinal cord, nerve root, and cervical intervertebral foramina provide a reference for the surgical procedures.
Decompression Effect of ACAFThe boundaries of the intervertebral foramen were the adjacent pedicles inferiorly and superiorly, by the medical aspect of the facet joint and the adjacent part of the articular column posteriorly, and by the posterolateral aspect of the uncovertebral joint, the intervertebral disc, and the inferior part of the suprajacentvertebrae anteriorly.16 The intervertebral foramina were divided into two anatomic zones: entrance zone and exit zone. The shape of the intervertebral foramina approximated a funnel, with their entrance zone being the narrowest part, and the shape of the nerve roots were conical, with their takeoff points from the central thecal sac being the largest part.16, 17 The ventral rootlet and dorsal rootlet merge into the spinal nerve at the entrance zone of intervertebral foramen. Thus, the entrance zone of intervertebral foramina and the takeoff points of nerve roots are the key sites which could influence the decompression effect. The takeoff points of the ventral rootlets are usually located higher than the corresponding intervertebral foramen, the decompression may be inadequate by discectomy alone. The corpectomy is sufficient in terms of decompression at the takeoff points of ventral rootlets, but it cannot always decompress the entrance zone of the intervertebral foramina adequately, especially for the unskilled surgeons. In ACAF surgery, the vertical slotting was performed in the medial of UP tip. Thus, most of the structure of posterior UP base were resected. Furthermore, we resected the intervertebral disc and inferior part of the suprajacentvertebrae in front of the intervertebral foramina to expand the narrowest part of intervertebral foramina, which is able to complete the decompression of the junctions of ventral rootlets and dorsal rootlets.
As our anatomical results show, the width of groove in ACAF surgery included the origins of bilateral ventral rootlets and the massive rootlets running laterally and caudally in the spinal canal. We found that the width of groove and length of ventral rootlet from the origin to the intervertebral foramina gradually increased as they became caudal. This suggests that the width of grooves in each segment in ACAF technique are inconsistent. We need to use the UP as an anatomical landmark to achieve a gradually increasing decompression width from the rostral to the caudal direction, so as to achieve complete decompression of the gradually extending nerve roots in each segment, and provide them with more space to pass through the intervertebral foramina. The effectiveness of decompression on the spinal nerve in the ACAF technique is also confirmed from the radiographic results, that show the satisfaction rate of decompression at the entrance zone of intervertebral foramina was significantly higher in the ACAF group, and the decompression width was significantly greater than the transverse diameter of spinal cord in ACAF group.
Since the spinal nerve originates from the spinal cord, it is located at the lateral and posterior sides of uncovertebral joint as well as the posterior side of vertebral artery, and runs laterally and caudally. Therefore, removal of the hyperplasticuncovertebral joint plays an important role in decompression of the nerve root. Jho18-20 proposed the anterior cervical foraminotomy for the treatment of cervical radiculopathy and myelopathy through completely resecting the UP with a drill. Since then, others had reported some modified techniques to generally avoid drilling the lateral margin of the UP to lessen the risk of vertebral artery injury21, 22, 29, 30. For stability, Pakzaban31 described the ultrasonic total uncinectomy (UTU) technique, who utilized an ultrasonic bone dissector to safely achieve complete resection of the UP during anterior cervical discectomy and decompress the entire length of the cervical nerve root up to the vertebral artery. The management of UPs in ACAF surgery could get a similar safety and decompression effect with these techniques. Our previous cadaveric study indicated that the distance between the UP tip and transverse foramen was larger than 2 mm, which verified the safety of ACAF surgery in the risk of vertebral artery injury15. ACAF was capable of accomplishing the complete anterior decompression on cervical nerve roots. Otherwise, wedging slotting15 would be preferred for patients with severe foraminal stenosis. The boundary of wedging slotting can extend to the pedicle, in some cases, the medial cortices of the pedicles will be removed to make sure the adequate decompression on the cervical nerve roots. As a consequence, ACAF is qualified for dealing with the anterior central, paracentral and lateral compression with cervical myelopathy and radiculopathy.
Revision StrategyAccording to the anatomic study, there was extra space on both sides after placing the titanium mesh in the groove created in ACAF surgery (Fig. 1D), which indicated a wider decompression slotting in ACAF surgery. It was directly verified by this radiographic result that the decompression width in ACAF was significantly greater than ACCF, consistent with our previous clinical study (17.9 ± 1.0 vs 15.1 ± 0.8 mm, P < 0.01)11. Moreover, ACAF could decompress the spinal nerve and the entrance zone of intervertebral foramina well, which makes it possible to revise the primary ACCF by the ACAF technique. Based on the typical case (Fig. 5), good radiographic and clinical outcomes had been reported in the revisio
留言 (0)