
記住我
Prostate cancer (PCa) represents a major healthcare burden globally. While PCa has been acknowledged as a major disease in the Western countries for decades, it is recently rising in incidence in the Eastern parts of the world, from 14.5% in 2008 to 27.9% in 2020 in the Eastern parts of Asia.1, 2 In Singapore, PCa is now the second most common cancer among males, which is partly driven by an increasing awareness of prostate-specific antigen (PSA) screening.3 As a result, patients are often diagnosed with localized disease, with the majority having low- or intermediate-risk disease as defined by the National Comprehensive Cancer Network (NCCN) risk-stratification criteria. In this group of patients, treatment options include active surveillance (for low-risk patients), radical prostatectomy or radiotherapy (RT), which can be delivered either by external beam radiotherapy (EBRT) or brachytherapy.4-6
For PCa patients who choose to undergo EBRT as their primary treatment, there are now several options for fractionation regimens that have demonstrated equipoise for disease control and survival. Ultra-hypofractionated RT (UHF-RT), which refers to the use of very large doses of 6–8 Gy per fraction, has been shown to confer comparable failure-free survival to conventionally fractionated radiotherapy in the HYPO-RT-PC study.7 In the same vein, several randomized controlled phase III trials comparing moderately hypofractionated (∼3 Gy per fraction) to conventionally fractionated RT have also demonstrated comparable efficacy with no increased incidence of late RT-induced toxicities.8-14 Collectively, these trials were designed on the scientific rationale that like breast cancers, PCa are sensitive to variation in RT dose-fraction size; this is implied by a low α/β ratio—a parameter that is estimated based on dose–response modeling using the linear–quadratic equation. To this point, an updated meta-analysis of 13,384 patients from 14 randomized trials by Vogelius and Bentzen indeed suggested that the α/β ratio for PCa lies between 1.3 and 2.0 Gy.15
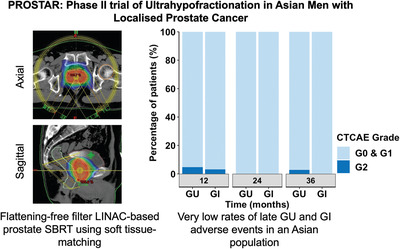
In this background, the utilization of UHF-RT in the treatment of PCa is thus appealing, especially in resource-limited settings. Its efficacy and safety have been reported in a number of large, real-world and prospective datasets.7, 16, 17 Nonetheless, there is a scarcity of data on the use of UHF-RT in Asian cohorts. Existing literature is mostly comprised of small retrospective series in low- and intermediate-risk PCa patients.18, 19 Here, we report the mature treatment efficacy and safety results of our single-institution, prospective phase II trial of UHF-RT, using two fractionation regimens, in Asian men with NCCN-defined low- to intermediate-risk PCa (PROSTAR–PROstate STereotactic Ablative Radiotherapy, NCT02313298, ClinicalTrials.gov).
2 MATERIALS AND METHODS 2.1 Study design and patientsThis was a prospective, single-arm phase II trial conducted at the National Cancer Centre Singapore (NCCS). Patients with histologically confirmed, nonmetastatic prostate adenocarcinoma were eligible. The inclusion criteria were as follows: (1) age ≥21 years; (2) NCCN-defined low-, favorable- or unfavorable intermediate-risk prostate adenocarcinoma (cT1c-T2c, Gleason's score [GS] 5–7, and PSA < 20 ng/ml); (3) the absence of distant metastasis on staging investigations with computed tomography (CT) of the thorax, abdomen, pelvis and/or skeletal scintigraphy and/or 68Gallium-labeled prostate-specific membrane antigen positron emission tomography (68Ga-PSMA-PET). Exclusion criteria include: (1) prior radical surgery (prostatectomy), cryosurgery or high-intensity focused ultrasound (HIFU) treatment; (2) prior pelvic irradiation or prostate brachytherapy; (3) prior history or synchronous malignancy; (4) prior/concurrent cytotoxic chemotherapy or androgen deprivation therapy (ADT) such as luteinising hormone-releasing hormone (LHRH) agonists or antagonists, anti-androgens, and bilateral orchiectomy for PCa; (5) prostate volume exceeding 80 cm3; (6) severe and active co-morbidities (e.g., unstable angina and/or congestive heart failure requiring hospitalization in the last six months). Patients with a prior history of transurethral resection of prostate tissue (TURP) were allowed to participate on trial, provided that the interval between the TURP and UHF-RT was more than eight weeks from the former procedure. Upon completion of patient recruitment on the original study protocol, a decision was undertaken to initiate an expansion study to enrol patients for treatment using a dose-escalated UHF-RT regimen (Cohort B). For Cohort B, NCCN high-risk patients were permitted if patients fulfilled the following criteria: (1) no GS 9–10; (2) absence of seminal vesicle invasion; and (3) PSA < 20 ng/ml. ADT was permitted for Cohort B at the treating physician's discretion. The study protocol was approved by the Singhealth Institutional Review Board (Protocol number: 2015/2444) and registered on ClinicalTrials.gov (NCT02313298). This study was performed in accordance with the Declaration of Helsinki and Good Clinical Practice Guidelines. All patients provided written informed consent prior to trial participation.
2.2 Treatment protocolUHF-RT was delivered by linear accelerator (LINAC)-based RapidArc system (Varian Medical System Inc., Palo Alto, CA). The prescribed dose was 36.25 Gy (Cohort A) and 37.5 Gy (Cohort B) in five fractions over 1.5– 2.5 weeks (every other day). Nonfiducial-based matching was performed with daily cone beam CT imaging (CBCT). The clinical target volume (CTV) included the prostate and proximal 1–1.5 cm of the seminal vesicles depending on the risk. A margin of 3 mm posteriorly and 5 mm in all other directions were added to the CTV to create the planning target volume (PTV). Dose was normalized around the 90% isodose line on average to allow the prescription dose to cover at least 95% of the PTV. The dose–volume histogram (DVH) goals for the rectum and bladder were such that < 1cm3 received 38.06 Gy and 39.0 Gy, respectively. Details of the treatment protocol are reported in the Appendix S1 (see treatment protocol).
2.3 Assessments and follow-upPatients were followed up with clinical assessments and PSA measurements 3-monthly for the first 24 months, 6-monthly between 25 and 60 months, and annually thereafter. Physician-scored genitourinary (GU) and gastrointestinal (GI) adverse events (AEs) were defined based on the Common Terminology Criteria for Adverse Events (CTCAE v4.0) and International Prostate Scoring System (IPSS). Acute and late AEs were defined as events occurring within and after 90-days post-UHF-RT, respectively. PRO-quality-of-life (QoL) outcomes were assessed in Cohort A using the Expanded Prostate Cancer Index Composite (EPIC) instrument at baseline, 12- and 24-month post-UHF-RT.
2.4 Statistical considerationsPrimary endpoint of the study was physician-scored late severe (≥G3) GU and GI AEs at 2 years post-UHF-RT. Sample size was estimated based on the primary endpoint. Assuming a cumulative incidence of 2-year late ≥G3 GU and GI AEs of 4–5%, a sample size of 72 would yield a 95% confidence interval of 0–10%, if the toxicity rate was 4%. Target accrual was set at 80 to account for a potential 10% loss of study participants to follow-up.
Secondary endpoints were physician-scored acute GU and GI AEs, PRO-QoL outcomes, and biochemical relapse-free survival (BRFS). The Kaplan–Meier method was used to estimate BRFS. BRFS was defined by the time from enrolment to PSA relapse by the Phoenix criterion (nadir+2) and/or death due to any cause. Patients who were alive were censored at the time of last follow up. Data cut-off date was July 1, 2021. Descriptive statistics were used to summarize patient demographics and treatment information. The Wilcoxon rank sum test was used to compare median IPSS scores within treatment groups, and the Kruskal–Wallis test was used to compare differences in median EPIC-QoL scores between the respective timepoints. Statistical calculations were performed using RStudio v1.2.1335 (RStudio, Boston, MA). Statistical significance was set at the threshold of p < 0.05.
3 RESULTS 3.1 Clinical characteristics of Cohorts A and BBetween March 2014 to June 2020, 105 patients were enrolled onto the trial (74 onto Cohort A from March 2014 to August 2019, and 27 onto Cohort B from January 2019 to June 2020); four patients from Cohort A were subsequently excluded (one patient exceeded the prostate size criteria and three patients withdrew from the study, Figure 1).

Consort diagram illustrating patient selection in this study
The clinical characteristics of patients in Cohort A and B are summarized in Table 1. Of the 74 patients in Cohort A, 26 (35.1%) had low-risk disease, 38 (51.4%) had favorable intermediate-risk disease, and 10 (13.5%) had unfavorable intermediate-risk disease. 26 (35.1%) patients had GS 6 disease, and 48 (64.9%) patients had GS 7 disease (38 [51.4%] GS 3+4, and 10 [13.5%] GS 4+3). Median PSA was 8.1 (IQR: 6.0–10.1) ng/ml. Of the 27 patients in Cohort B, 13 (48.1%) had favorable intermediate-risk, 7 (25.9%) unfavorable intermediate-risk, and 7 (25.9%) had NCCN high-risk disease.
TABLE 1. Clinical and pathological characteristics of Cohorts A and B Number of patients (%) Characteristics Cohort A (N = 74) Cohort B (N = 27) Median follow up, month (IQR) 45.4 (23.9–63.0) 23.7 (21.1–30.3) Median age, year (IQR) 68.0 (65.0–72.8) 69.0 (63.0–76.5) NCCN risk group Low 26.0 (35.1%) 0.0 (0.0%) Intermediate (Zumsteg–Spratt risk classification) Favorable 38.0 (51.4%) 13.0 (48.1%) Unfavorable 10.0 (13.5%) 7.0 (25.9%) High 0.0 (0.0%) 7.0 (25.9%) cT-category cT1 62.0 (83.8%) 16.0 (59.3%) cT2 12.0 (16.2%) 6.0 (22.2%) cT3a 0.0 (0.0%) 5.0 (18.5%) Gleason score International Society of Urological Pathology (ISUP) 3+31 26.0 (35.1%) 2 (7.4%) 3+42 38.0 (51.4%) 13 (48.1%) 4+33 10.0 (13.5%) 9 (33.3%) 4+44 0.0 (0.0%) 3 (11.1%) Core burden<50%
≥50%
66.0 (89.2%)
7.0 (9.5%)
18.0 (66.7%)
8.0 (29.6%)
Prior TURP Yes 5.0 (6.8%) 0.0 (0.0%) No 69.0 (93.2%) 27.0 (100%) Median pretreatment prostate-specific antigen (PSA), ng/ml (IQR) 8.1 (6.0–10.1) 8.3 (4.8–11.6) MRI imaging featuresProstate size (cm3)
Tumor focality
Unifocal
Multifocal
NA
Extracapsular extension (ECE)
Yes
No
NA
41.1 (32.1–54.5)
30.0 (40.5%)
29.0 (39.2%)
15.0 (20.3%)
0.0 (0.0%)
73.0 (98.6%)
1.0 (1.4%)
32.8 (25.6–42.9)
6.0 (22.2%)
21.0 (77.8%)
0.0 (0.0%)
9.0 (33.3%)
18.0 (66.7%)
0.0 (0.0%)
Androgen deprivation therapy (ADT) Yes 0.0 (0.0%) 7.0 (25.9%) Duration of ADT (days) – 199.0 (183.0–282.0)No
NA
73.0 (98.6%)
1.0 (1.4%)
20.0 (74.1%)
0.0 (0.0%)
3.2 Acute AEs post-UHF-RTFor both Cohorts A and B, we observed that ≥G2 GU AEs were most frequent at 14-days post-UHF-RT (Figure 2A,B). Note that 23.6% (17/72) from Cohort A and 24.0% (6/25) from Cohort B reported ≥G2 GU AEs; 2 (2.7%) and 1 (4.0%) patient experienced G3 GU AEs, respectively. These symptoms resolved by three months post-UHF-RT in both cohorts. The trend in GU AEs by CTCAE corresponded with the IPSS scores post-UHF-RT (Figure 2C,D). IPSS scores were significantly higher at 14-days post-UHF-RT (median: 11.0 vs. 5.0, p < 0.001 [Cohort A]; 12.0 vs. 10.0, p = 0.413 [Cohort B]), independent of the baseline IPSS status (Figure S1). Nonetheless, IPSS scores reverted to baseline by 6 months post-UHF-RT in both cohorts.
 Stacked bar chart illustrating percentage of patients who experienced genitourinary (GU) adverse events (AEs) in each respective cohort based on the Common Terminology Criteria for Adverse Events (CTCAE). (A) GU AEs in Cohort A (N = 74). (B) GU AEs in Cohort B (N = 25). Boxplot illustrating distribution of International Prostate Scoring System (IPSS) scores over a period of 24 months post-ultra-hypofractionated radiotherapy (UHF-RT) in (C) Cohort A (N = 73) and (D) IPSS scores in Cohort B (N = 20). (E) Gastrointestinal (GI) AEs in Cohort A (N = 74). (F) GI AEs in Cohort B (N = 25). Two patients from Cohort B had missing data and were not included in the plot [Colour figure can be viewed at wileyonlinelibrary.com]
Stacked bar chart illustrating percentage of patients who experienced genitourinary (GU) adverse events (AEs) in each respective cohort based on the Common Terminology Criteria for Adverse Events (CTCAE). (A) GU AEs in Cohort A (N = 74). (B) GU AEs in Cohort B (N = 25). Boxplot illustrating distribution of International Prostate Scoring System (IPSS) scores over a period of 24 months post-ultra-hypofractionated radiotherapy (UHF-RT) in (C) Cohort A (N = 73) and (D) IPSS scores in Cohort B (N = 20). (E) Gastrointestinal (GI) AEs in Cohort A (N = 74). (F) GI AEs in Cohort B (N = 25). Two patients from Cohort B had missing data and were not included in the plot [Colour figure can be viewed at wileyonlinelibrary.com]
Figure 2E,F illustrates the GI acute AEs that were reported in our trial. For Cohort A, we observed that ≥G2 GI AEs were most frequent at 14 days post-UHF-RT (Figure 2E). 9.7% (7/72) of patients reported ≥G2 GI AEs, but there was no G3 event. We observed a similar trend for Cohort B, although 36.0% (9/25) of patients reported ≥G2 GI toxicities at the same timepoint (Figure 2F); this was largely attributed to proctitis, rectal bleeding, and urgency symptoms. In both cohorts, the GI symptoms resolved by 3 months post-UHF-RT.
3.3 Late AEs post-UHF-RTNo ≥G3 GU and GI AEs were observed in both cohorts. For Cohort A, we observed a bimodal peak for late ≥G2 GU AEs at the 6–12 months (2.7%–4.7%, Figure 2A) and the 30–48 months (2.9%–6.9%, data not shown) timepoints. Likewise, for Cohort B, we observed a peak incidence of late ≥G2 GU AEs between 9 and 12 months (5.0%–8.3%) post-UHF-RT. Nonetheless, the short duration of follow-up for Cohort B precluded any insights to a possible delayed rise for late GU AEs.
Late ≥G2 GI AEs were infrequent in both cohorts. We observe 3.1% (2/64) and 5.0% (1/20) in Cohorts A and B, respectively, at 12 months post-UHF-RT (Figure 2C,F). No ≥G2 GI AEs were observed at the 24-month timepoint.
3.4 PSA kinetics post-UHF-RT for Cohorts A and BMedian PSA at 24 months post-UHF-RT for Cohort A was 0.80 (IQR: 0.45–1.50) ng/ml. PSA tracking revealed a biexponential decline, with the steepest drop occurring within the first 6 months posttreatment (Figure S2). Interestingly, median nadir PSA for Cohort B (0.62 [IQR: 0.45–0.97] ng/ml) was lower than Cohort A (1.40 [IQR: 0.67–3.02] ng/ml) at 24 months follow-up; seven patients who had received ADT were excluded from this analysis. This is consistent with the higher proportion of patients with a more than 50% decline in PSA levels from pretreatment values in Cohort B than Cohort A at all the timepoints (73.3% vs. 31.5% [1-month]; 78.6% vs. 58.9% [3-month]; 88.8% vs. 77.0% [6-month]; 100.0% vs. 98.1 [18-month]; 100.0% vs. 87.8% [24-month]; Figure 3A).
 (A) Stacked bar chart illustrating change in prostate-specific antigen (PSA) values over a period of 24 months post-ultra-hypofractionated radiotherapy (UHF-RT) as compared to pretreatment PSA values. Patients were stratified into whether their PSA levels at each timepoint had a > 50% change in PSA value compared to pretreatment levels or wileyonlinelibrary.com]
(A) Stacked bar chart illustrating change in prostate-specific antigen (PSA) values over a period of 24 months post-ultra-hypofractionated radiotherapy (UHF-RT) as compared to pretreatment PSA values. Patients were stratified into whether their PSA levels at each timepoint had a > 50% change in PSA value compared to pretreatment levels or wileyonlinelibrary.com]
We report the survival outcomes for Cohort A, given the longer median follow-up duration for this group of patients. We recorded one (1.3%) biochemical relapse that occurred at 48 months of follow-up, and three (4.0%) noncancer-related death events. The estimated 3-year biochemical relapse free-survival for Cohort A was 98.4% (95% CI: 95.0–100.0, Figure 3B).
3.5 QoL outcomes in Cohort ATable 2 shows the median EPIC-QoL scores for GU, GI, and sexual domains measured at pretreatment, 12 and 24 months post-UHF-RT for Cohort A. Overall, we did not observe any significant change in QoL scores over time across the three domains, except for sexual scores. Specifically, there is a deterioration in sexual function at 12 and 24 months for patients in the upper 50th percentile at baseline (median: 55.56 [12 month] and 52.34 [24 month] vs. 63.89 [pretreatment]).
TABLE 2. Median Expanded Prostate Cancer Index Composite (EPIC)-Quality-of-life (QoL) scores for genitourinary (GU), gastrointestinal (GI), and sexual domains measured pretreatment, and at 12 and 24 months post-ultra-hypofractionated radiotherapy (UHF-RT) for Cohort A Overall Upper 50th percentile Lower 50th percentile Baseline 12 Months 24 Months p Value Baseline 12 Months 24 Months Baseline 12 Months 24 Months Median EPIC-QoL score (urinary) Summary 95.8 (11.6) 95.8 (11.5) 95.8 (12.9) 0.766 100 (0.97) 100 (1.0) 100 (0.8) 85.4 (11.1) 82.7 (10.8) 86.8 (14.4) Function 83.3 (7.9) 83.3 (7.5) 83.3 (6.0) 0.656 83.3 (–) 83.3 (-) 83.3 (–) 77.8 (10.2) 73.7 (7.9) 73.7 (5.3) Bother 92.9 (15.2) 92.9 (16.2) 96.4 (19.5) 0.567 100 (1.56) 100 (1.6) 100 (–) 78.6 (13.6) 78.6 (16.6) 83.9 (23.1) Median EPIC-QoL score (Bowel) Summary 97.9 (11.4) 95.8 (11.0) 97.9 (13.1) 0.980 100 (–) 100 (0.8)100 (–)
91.7 (13.0) 89.6 (11.4) 85.4 (14.4) Function 96.4 (9.7) 96.4 (9.0) 96.4 (9.5) 0.862 100 (–) 100 (–) 100 (–) 85.7 (11.4) 87.5 (10.3) 85.7 (10.1) Bother 100 (14.7) 96.4 (14.3) 100 (17.9) 0.644 100 (–)100 (–)
100 (–)
85.7 (17.7) 85.7 (16.1) 83.9 (21.2) Median EPIC-QoL score (Sexual) Summary 48.7 (22.3) 47.8 (18.4) 49.4 (17.3) 0.937 68.3 (12.6) 64.8 (9.9) 61.5 (13.0) 30.8 (11.0) 34.6 (10.0) 34.0 (13.0) Function 44.9 (21.6) 44.4 (19.9) 45.4 (18.5) 0.849 63.9 (11.4) 55.6 (10.9) 52.3 (10.5) 30.1 (13.4) 25.9 (10.4) 30.5 (12.6) Bother 75.0 (29.0) 65.6 (29.7) 78.1 (26.1) 0.885 100 (2.90) 100 (8.7) 100 (5.3) 50.0 (15.9) 43.8 (14.3) 50.0 (15.0) 4 DISCUSSIONHere, we report our single-institution data of 100 men with localized PCa, who were treated using two UHF-RT regimens, and assessed for efficacy and toxicities. Primary endpoint of the study was severe (G3 and above) GU and GI late AEs. Overall, we observed low incidences of late toxicities, which did not exceed our prespecified upper boundary estimate of 10%. We performed longitudinal evaluations of AEs post-UHF-RT. Of note, we saw a bimodal peak with GU AEs at 12 and 48 months post-UHF-RT for Cohort A, ranging between an incidence of 2.7%–6.9%. Likewise, we saw a similar peak at 12 months for patients who received a higher dose (Cohort B), albeit the follow-up period was inadequate to ascertain a delayed bounce for late GU AEs. For late GI AEs, these events were limited (3.1–5.0%), and mostly occurred at the 12-month timepoint. We also observed a characteristic pattern with acute GU and GI AEs. ≥G2 events were more frequent at 23.6%–24.0% and 9.7%–36.0%, respectively, peaking at 14-days posttreatment, and recovering within 1–3 months. Interestingly, we observed a much higher rate of acute GI AEs in patients treated with 37.5 Gy than 36.25 Gy, which could suggest a steep dose–response above a certain threshold for this normal tissue endpoint. Expectedly, only one PSA failure was recorded in Cohort A, which comprised of NCCN low- and intermediate-risk PCa, relative to three noncancer-related deaths. Taken together, our results validate the data of UHF-RT in Western cohorts that it is safe and effective, with no unexpected increase in late AEs and compromise in disease control.
As aforementioned, the outcomes of UHF-RT are well ascertained based on several large Western cohorts, indicating high rates of biochemical control and low rates of toxicities.7, 17 In a pooled cohort study of 2,142 patients from 10 institutions, including 2 multi-institutional phase 2 trials, Kishan and colleagues reported extremely low rates of severe AEs (incidence of acute ≥G3 AEs was only 0.60% for GU and 0.09% for GI). Similarly, low rates of biochemical recurrence were noted in that study; 7-year cumulative incidence of biochemical recurrence was 4.5% and 8.6% for low- and intermediate-risk disease, respectively.17 Nonetheless, while there is an abundance of data among Western patients, in truth, there have only been two prospective studies from Asia, both of which the results are not yet available.20, 21 Our toxicity outcomes in patients who were treated with 36.25 Gy were in fact comparable to the results of the PACE-B trial, which reported an incidence of 10.4% for ≥G2 acute GI and 23.1% for ≥G2 acute GU.16 Likewise, QoL analyses, examined using the same EPIC instrument, were comparable between the present study and the PACE-B trial. These results are also consistent with the data from the Dutch HYPO-RT-PC trial, with the updated long-term QoL analyses confirming that UHF-RT was equally well tolerated as conventionally fractionated RT up to 6 years posttreatment.22
On a separate note, it is noteworthy that a marginal dose-escalation from 36.25 to 37.5 Gy would incur clinically significant differences in PSA response and acute GI AEs between the two cohorts. While we acknowledged the limitations of this unplanned analysis and that clinical characteristics of both cohorts were unmatched, it is nonetheless interesting that we observed a more profound PSA response with 37.5 Gy, as early as a month posttreatment. These data relate to the recent results of a Phase I dose-escalation study by Zelefsky and colleagues, whereby they observed lower biochemical failure rates and proportions of positive biopsies at 2-year posttreatment with dose-escalation.23 Nonetheless, the long-term clinical implications of this early response remain to be determined, and it is plausible that a higher dose is required for patients with high-risk PCa.24
Some limitations of this study deserve mention. First, this was a single-arm design without a comparator conventionally fractionated RT arm. Thus, this limits our ability to conclude if indeed, UHF-RT leads to lower AE rates, given the tighter PTV margins. Next, we had to accept a nonminuscule proportion of missing data due to patient's noncompliance, especially for the later study timepoints in this trial. This is not unexpected for a study, for which we deployed an AE-specific primary endpoint and the bulk of the data collection relates to treatment-related AE and QoL.25 Third, we had included NCCN high-risk patients in Cohort B and seven patients had received concurrent ADT with UHF-RT, and thus, any comparison between both cohorts ought to be cautiously interpreted. Finally, we acknowledged that the follow-up for Cohort B is short, and longer follow-up will provide a more complete insight regarding the occurrence of another peak in GU AEs and the efficacy of UHF-RT in this higher risk-group of patients.
Looking ahead, opportunities to enhance the therapeutic gains of UHF-RT could include dose-escalation in higher risk patients. For example, in the randomized phase III FLAME trial, investigators found that focal boost of a magnetic resonance imaging (MRI)-defined dominant lesion in addition to whole gland prostate RT improved biochemical and disease control compared to whole gland treatment alone.26 Thus, we postulate that given the low frequency of late AEs with UHF-RT (presumably due to the tighter PTV margins and steep dose gradients), focal boost with a UHF schema may be feasible, especially with the introduction of a spacer to increase the anatomical distance between the prostate and the rectum. We await long-term follow up on late AEs from the phase II hypoFLAME trial, which evaluated such an UHF-RT schema, although it is to be noted that rectal spacers were not mandated for all patients recruited in the trial.27 Next, MRI-guided RT delivery is also being currently investigated; here, the advantages are the enhanced soft tissue resolution and the possibility of performing radiomics analyses for correlation with treatment response.28 Nonetheless, such a treatment is lengthy, and requires several steps of RT quality assurance, including real-time tracking, which may be a hindrance to broad implementation in less resourced low- to middle-income countries (LMICs). In the same vein, combinatorial strategies with next-generation anti-androgen therapies or other novel therapeutic agents (especially in higher risk patients) are currently the subject of investigation in a number of ongoing clinical trials.29-31 Finally, the advocacy for UHF-RT in real-world clinical practice can be catalyzed by data sharing of well-curated prospective data from multi-institutions.17, 24 This will help to foster education and training of teams to ensure safe delivery of UHF-RT.
5 CONCLUSIONHerein, we report the first results of our prospective phase II trial confirming the safety of UHF-RT using two fractionation regimens in Asian men with localized PCa. UHF-RT can be considered as a fractionation schema for patients with localized PCa given the seemingly favorable efficacy and safety results of our study, which validate the data of UHF-RT in Western cohorts.
ACKNOWLEDGMENTSWe would like to acknowledge the goodwill of all the patients who participated on the PROSTAR trial. We also like to thank all members of the Chua laboratory for their scientific inputs on the findings of this study. Melvin L. K. Chua is supported by the National Medical Research Council Singapore Clinician Scientist Award (NMRC/CSA-INV/0027/2018), National Research Foundation Proton Competitive Research Program (NRF-CRP17-2017-05), Ministry of Education Tier 3 Academic Research Fund (MOE2016-T3-1-004), the Duke-NUS Oncology Academic Program Goh Foundation Proton Research Programme, NCCS Cancer Fund, and the Kua Hong Pak Head and Neck Cancer Research Programme.
CONFLICT OF INTERESTMelvin L.K. Chua reports personal fees from Astellas, Janssen, Bayer, Pfizer, MSD, personal fees and nonfinancial support from AstraZeneca, personal fees and grants from Ferring, personal fees and nonfinancial support from Varian, nonfinancial support from Decipher Biosciences, nonfinancial support from MedLever, and consults for immunoSCAPE Inc., outside the submitted work. All other authors declare no conflict of interest.
AUTHOR CONTRIBUTIONSStudy conception and design: Jonathan Y. H. Teh, Daniel Y. H. Tan, and Melvin L. K. Chua. Acquisition, analysis, or interpretation of data: All authors. Statistical analyses: Janice S. H. Tan, Laura L. Y. Tan, and Melvin L. K. Chua. Obtained funding: Melvin L. K. Chua. Administrative, technical, or material support: Sheena X. F. Tan, Enya H. W. Ong, and Melvin L. K. Chua. Study supervision: Melvin L. K. Chua. Drafting of manuscript: Janice S. H. Tan, Laura L. Y. Tan, and Melvin L. K. Chua. Approval of final manuscript: All authors.
PATIENT CONSENT STATEMENTAll patients provided written informed consent prior to participation on trial.
ETHICS STATEMENTThe study protocol was approved by the Singhealth Institutional Review Board (Protocol number: 2015/2444) and registered on ClinicalTrials.gov (NCT02313298).
留言 (0)