
記住我
Globally, breast cancer is the most commonly diagnosed cancer among women.1 In 2018, Australia/New Zealand had the highest incidence rate of breast cancer worldwide, whereas in India, breast cancer was the leading cause of cancer death among women.1 Historically, endocrine monotherapy has been the preferred first-line treatment option for postmenopausal women with estrogen receptor–positive (ER+)/human epidermal growth factor receptor 2–negative (HER2–) advanced breast cancer (ABC).2 The first-in-class cyclin-dependent kinase 4/6 (CDK4/6) inhibitor, palbociclib, in combination with letrozole was initially approved in 2015 in the United States for the treatment of ER+/HER2–ABC.3, 4 Results from the PALOMA clinical trials showed a statistically significant improvement in median progression-free survival (PFS) with palbociclib plus letrozole versus letrozole alone (PALOMA-15: 20.2 vs. 10.2 months; hazard ratio = 0.488 [95% CI, 0.319–0.748], P = 0.0004) or placebo plus letrozole (PALOMA-26, 7: 27.6 vs. 14.5 months; hazard ratio = 0.56 [95% CI, 0.46–0.69], P < 0.0001) in postmenopausal women with ER+/HER2– ABC. The PALOMA-3 trial demonstrated the benefit of palbociclib plus fulvestrant compared with placebo plus fulvestrant (median PFS, 11.2 vs. 4.6 months; hazard ratio = 0.50 [95% CI, 0.40–0.62]; P < 0.00018, 9) in pre-/postmenopausal women with hormone receptor–positive (HR+)/HER2– ABC who had disease progression following endocrine therapy. The most frequently reported adverse event (AE) with palbociclib was neutropenia in all three PALOMA trials.5, 7, 9 Quality of life was also maintained with the addition of palbociclib to either letrozole or fulvestrant treatment.6, 9
As a result of recent advances in targeted therapies, the National Comprehensive Cancer Network category 1, Cancer Australia, and European Society for Medical Oncology international consensus guidelines for ABC now recommend the addition of a CDK4/6 inhibitor to endocrine therapy as a preferred treatment regimen for premenopausal and postmenopausal women with HR+/HER2– ABC.2, 10, 11 However, the safety and efficacy of medications may differ across various patient subgroups based on factors such as race or ethnicity.12
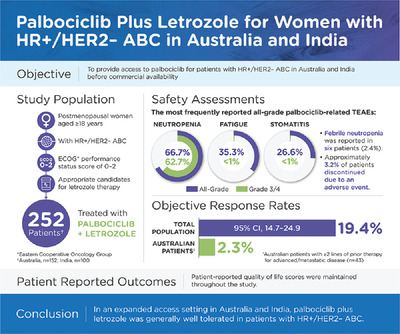
The primary objective of this expanded access program study was to evaluate the safety of palbociclib plus letrozole in patients with HR+/HER2– ABC for whom letrozole therapy was deemed appropriate in Australia and India before palbociclib became commercially available. In addition, antitumor activity of palbociclib was assessed. Patient-reported outcomes (PROs) were also collected for the Australian cohort.
2 METHODS 2.1 Study designThis was an open-label, single-arm, multinational, multicenter (20 sites) clinical trial providing access to palbociclib in Australia and India for patients with HR+/HER2– ABC who were deemed appropriate candidates for letrozole therapy (NCT02679755). The study protocol was approved by the Institutional Review Boards and/or Independent Ethics Committee at each of the participating study sites. The study was conducted in compliance with the Declaration of Helsinki, Good Clinical Practice guidelines, and local country regulations relevant to the use of new therapeutic agents. All patients provided written and informed consent.
Key inclusion criteria included postmenopausal women, defined as per local practice, aged ≥18 years with HR+/HER2– ABC and an Eastern Cooperative Oncology Group (ECOG) performance status score of 0–2 who were deemed appropriate candidates for letrozole therapy. These broad entry criteria led to the enrollment of many patients who were heavily pretreated in the metastatic disease setting in Australia. To ensure appropriate patients were enrolled in the study, the inclusion criteria was amended to specify “in the first-line advanced/metastatic setting.” Key exclusion criteria included prior treatment with any CDK inhibitor, previous participation in a palbociclib clinical trial, and active uncontrolled or symptomatic brain metastases.
Patients received palbociclib orally once daily at 125 mg for 3 weeks followed by 1 week off treatment for each 4-week cycle (3/1 schedule). Commercially available letrozole was administered orally at 2.5 mg once daily on a continuous daily dosing schedule according to product labeling and in compliance with local prescribing information. Patients continued to receive palbociclib and letrozole until disease progression, symptomatic deterioration, unacceptable toxicity, death, or withdrawal of consent, whichever occurred first.
2.2 OutcomesThe primary endpoint was safety. AEs were characterized by type, frequency, severity (as graded by the National Cancer Institute Common Terminology Criteria for Adverse Events version 4.03), and seriousness. All AEs reported after the initiation of palbociclib were considered treatment-emergent AEs (TEAEs). All AEs were coded by System Organ Class and preferred term (PT) using the Medical Dictionary for Regulatory Activities coding, with cluster terms used as noted in the table footnotes. Hematology was performed at screening, on Days 1 and 14 of the first two cycles, and then on Day 1 of each subsequent cycle, and was recorded in the case report form (CRF). Blood chemistry was performed at screening and per routine clinical practice thereafter; blood chemistry data were collected at screening only.
Secondary endpoints included tumor response (based on investigator assessment per local practice) and PRO of health-related quality of life and health status. Tumor assessments were performed at screening and per routine clinical practice according to the patients’ clinical status. The investigators’ assessments were reported on the CRFs. The best tumor response was the best outcome the patient had out of all the tumor assessments during the study as assessed by the local investigator; investigators were not required to use Response Evaluation Criteria In Solid Tumors (RECIST) criteria. Duration of treatment was calculated as the length of time patients remained on palbociclib treatment from the first day of treatment until the last day of treatment in this study, regardless of the reason for discontinuation.
Patient-reported outcomes of health-related quality of life and health status were assessed using the European Quality of Life-5 Dimensions (EQ-5D) instrument in Australian patients only. Patients completed the EQ-5D questionnaire at predose at Cycle 1/Day 1, at every clinical visit thereafter, and at the end of study. Progression-free survival (PFS) and overall survival (OS) were not included in the study objectives; therefore, these data were not collected.
2.3 Statistical analysesApproximately 300 patients from Australia and India were to be enrolled in this study. The as-treated (AT) population or safety analysis set included all patients who received ≥1 dose of palbociclib. The PRO-evaluable population was defined as patients from the AT population who completed the EQ-5D at baseline and ≥1 visit after baseline.
Tumor assessments were performed at screening and per local practice. No uniform assessment schedule was planned for patients across the sites. As an expanded access program study, no inferential analyses were planned, and no hypotheses were tested. The objective response (OR) rate and the corresponding exact 95% two-sided confidence interval (CI) were calculated using standard methods based on the binomial distribution. A descriptive summary of treatment duration (mean, median, range) was generated.
The EQ-5D index was derived by combining one level from each of the five dimensions and converting it to a single summary index or health utility value, a higher score indicating better quality of life/well-being. For patients from Australia, analysis of PROs used descriptive statistics for the actual score and change from baseline for the EQ-5D index and EQ-5D visual analog scale (VAS) scores. The mean (95% CI), median (range), and number of patients completing the scale at each time assessment after baseline were summarized.
3 RESULTS 3.1 PatientsA total of 252 patients were enrolled in the study at 20 sites across Australia and India. In Australia, a total of 152 patients were enrolled beginning in March 2016 to January 2018; in India, 100 patients were enrolled beginning in March 2017 to June 2018. All enrolled patients received palbociclib and letrozole and were included in the AT population for safety analysis (Figure S1).
Patient demographics and baseline disease characteristics are included in Table 1. The median age was 58 years (range, 30–83 years), and 29.4% of patients were aged ≥65 years. Demographic characteristics were generally similar between the Australian and Indian cohorts, with the exception of the proportion of White and Asian patients. In the overall population, 75% of patients had ductal carcinoma, whereas 15.9% had lobular carcinoma. Ductal carcinoma was less common in the Australian cohort relative to the Indian cohort (67.8% vs. 86.0%, respectively). Prior treatment for metastatic disease was more frequent in the Australian cohort compared with patients from India (61.8% vs. 31.0%, including prior chemotherapy [45.9% vs. 32.0%], and prior endocrine therapy [63.2% vs. 54.3%]). More patients in the Australian cohort (n = 17; 18.1%) were heavily pretreated (>3 prior therapies in the metastatic disease setting) compared with patients in the Indian cohort (n = 0; Table S1). At the conclusion of the study, a total of 139 (55.2%) patients discontinued from the study (Australian cohort, n = 105; Indian cohort, n = 34); 107 patients (42.5%) had discontinued because of disease progression, 8 patients (3.2%) discontinued because of AEs, and 113 patients (44.8%) were considered to have “completed” the study after transitioning to commercially available palbociclib once it became commercially available in each country.
TABLE 1. Patient demographic and baseline characteristics Characteristica Palbociclib + Letrozole Australian Cohort (n = 152) Palbociclib + Letrozole Indian Cohort (n = 100) Palbociclib + Letrozole Total Cohort (N = 252) Age, years Median (range) 58 (34–83) 58 (30–79) 58 (30–83) Age group, years 18–44 27 (17.8) 13 (13.0) 40 (15.9) 45–64 80 (52.6) 58 (58.0) 138 (54.8) ≥65 45 (29.6) 29 (29.0) 74 (29.4) Race White 130 (85.5) 0 (0.0) 130 (51.6) Black 1 (0.7) 0 (0.0) 1 (0.4) Asian 12 (7.9) 100 (100.0) 112 (44.4) Other 9 (5.9) 0 (0.0) 9 (3.6) ECOG PS 0 86 (56.6) 38 (38.0) 124 (49.2) 1 60 (39.5) 60 (60.0) 120 (47.6) 2 6 (3.9) 2 (2.0) 8 (3.2) ER+ 152 (100) 100 (100) 252 (100) PR+ 115 (75.7) 88 (88.0) 203 (80.6) Histopathological classification Ductal carcinoma 103 (67.8) 86 (86.0) 189 (75.0) Lobular carcinoma 32 (21.1) 8 (8.0) 40 (15.9) Unknown 5 (3.3) 6 (6.0) 11 (4.4) Other 12 (7.9) 0 (0.0) 12 (4.8) Duration of breast cancer since histopathological diagnosis, years Median (range) 5.8 (0.0–32.0) 0.7 (0.0–17.0) 3.6 (0.0–32.0) Prior surgeries 123 (80.9) 57 (57.0) 180 (71.4) Prior radiation therapies 117 (77.0) 52 (52.0) 169 (67.1) Prior systemic therapies 139 (91.4) 61 (61.0) 200 (79.4) Prior metastatic therapies 94 (61.8) 31 (31.0) 125 (49.6) No. of regimens 1 51 (54.3) 25 (80.6) 76 (60.8) 2 16 (17.0) 6 (19.4) 22 (17.6) 3 10 (10.6) 0 (0.0) 10 (8.0) > 3 17 (18.1) 0 (0.0) 17 (13.6) Prior chemotherapyb 109 (71.7) 50 (50.0) 159 (63.1) Neoadjuvant 14 (12.8) 7 (14.0) 21 (13.2) Adjuvant 78 (71.6) 34 (68.0) 112 (70.4) Advanced/metastatic 50 (45.9) 16 (32.0) 66 (41.5) Prior endocrine therapy† 125 (82.2) 35 (35.0) 160 (63.5) Aromatase inhibitor 101 (80.8) 25 (71.4) 126 (78.8) Fulvestrant 9 (7.2) 0 (0.0) 9 (5.6) Tamoxifen 78 (62.4) 14 (40.0) 92 (57.5) Type of prior endocrine therapy Neoadjuvant 1 (< 1.0) 0 (0.0) 1 (< 1.0) Adjuvant 91 (72.8) 19 (54.3) 110 (68.8) Advanced/metastatic 79 (63.2) 19 (54.3) 98 (61.3) Abbreviations: ECOG PS, Eastern Cooperative Oncology Group performance status; ER, estrogen receptor; PR, progesterone receptor. 3.2 Adverse eventsThe median durations of treatment were 12 months (range, <1.0–35.7) for palbociclib and 12.3 months (range, <1 to 39.5) for letrozole. A total of 60 patients (23.8%) had one palbociclib dose reduction, and 31 patients (12.3%) had two dose reductions. Palbociclib dose interruptions due to AEs were reported in 187 patients (74.2%).
In the Australian cohort, the median durations of treatment for palbociclib and letrozole were 13.6 months (range, <1.0–35.7) and 13.8 months (<1.0–35.9), respectively. In the Indian cohort, the median durations of treatment were 10.7 months (range, <1.0–22.2) and 10.9 months (range, <1.0–22.4), respectively. More patients in the Australian cohort reported ≥1 palbociclib dose reduction than in the Indian cohort (48.7% vs. 17.0%, respectively), reflecting a more heavily pretreated population. In the subgroup of patients in the Australian cohort who received ≥2 lines of prior metastatic therapies (n = 43), the median duration of treatment was approximately 5.9 months (range, <1.0–35.5) for palbociclib and 18 patients (41.9%) had ≥1 palbociclib dose reduction. In this same subgroup, 39 patients (90.7%) had a palbociclib dose interruption due to AEs.
In the overall AT population, all-causality AEs were reported in 244 patients (96.8%); grade 3 or 4 AEs were reported in 193 patients (76.6%), and serious AEs (SAEs) were reported in 63 patients (25%; Table 2). A total of 223 patients (88.5%) experienced palbociclib-related AEs; 172 patients (68.3%) had grade 3 or 4 AEs (Table 3). Palbociclib-related SAEs were reported in 20 patients (7.9%; Table S2).
TABLE 2. Overview of all-causality AEs (AT population) Event Palbociclib + Letrozole (N = 252) Number of AEs 2,293 Patients with AEs 244 (96.8) Patients with SAEs 63 (25.0) Patients with grade 3 or 4 AEs 193 (76.6) Patients with grade 5 AEs 10 (4.0) Permanent patient discontinuations due to AEs 11 (4.4) Permanent patient discontinuations from palbociclib due to AEs 11 (4.4) Permanent patient discontinuations from letrozole due to AEs 11 (4.4) Temporary patient discontinuations from palbociclib due to AEs 188 (74.6) Temporary patient discontinuations from letrozole due to AEs 30 (11.9) Patients with dose reduction of palbociclib due to AEs 91 (36.1)Patients with dose reduction and temporary discontinuations of palbociclib due to AEs
83 (32.9) Abbreviations: AE, adverse event; AT, as-treated; SAE, serious adverse event. Note. All values are presented as n (%). Included data up to 28 days after last dose of study drug. Except for the number of AEs, patients were counted only once per treatment in each row. SAEs were counted according to the investigator's assessment. Severity counts were based on the maximum severity or grade of event. TABLE 3. Palbociclib-related treatment-emergent AEs that occurred in ≥10% of patients (AT population) Adverse event Palbociclib + Letrozole (N = 252) Grade 1 Grade 2 Grade 3 Grade 4 All grades Patients with any AE 27 (10.7) 24 (9.5) 142 (56.3) 29 (11.5) 223 (88.5) Neutropeniaa 0 (0.0) 10 (4.0) 131 (52.0) 27 (10.7) 168 (66.7) Fatigue 66 (26.2) 22 (8.7) 1 (0.4) 0 (0.0) 89 (35.3) Stomatitisb 52 (20.6) 13 (5.2) 2 (0.8) 0 (0.0) 67 (26.6) Alopecia 37 (14.7) 0 (0.0) 0 (0.0) 0 (0.0) 37 (14.7) indentLevel="1"Diarrhea 24 (9.5) 8 (3.2) 4 (1.6) 0 (0.0) 36 (14.3) Nausea 33 (13.1) 3 (1.2) 0 (0.0) 0 (0.0) 36 (14.3) Infectionsc 17 (6.7) 9 (3.6) 8 (3.2) 0 (0.0) 34 (13.5) Anemiad 1 (0.4) 9 (3.6) 17 (6.7) 0 (0.0) 27 (10.7) Thrombocytopeniae 5 (2.0) 11 (4.4) 8 (3.2) 3 (1.2) 27 (10.7) Abbreviations: AE, adverse event; AT, as-treated; MedDRA, Medical Dictionary for Regulatory Activities coding. Note. All values are presented as n (%). Included data up to 28 days after last dose of study drug. Palbociclib-related was defined as AE causality assessed by investigator as “Yes, related” or “Unknown.”In patients who received ≥2 lines of prior therapy for metastatic disease in the Australian cohort, all-causality AEs were reported in all 43 patients; grade 3 or 4 AEs were reported in 37 patients (86.0%), and SAEs in 17 patients (39.5%; Table S3). Forty patients (93.0%) in this subgroup reported a palbociclib-related AE, with grade 3 or 4 AEs reported in 34 patients (79.1%) and SAEs in 7 patients (16.3%); 2 patients (4.7%) permanently discontinued palbociclib because of an AE.
The most frequently reported all-causality TEAEs in the AT population were neutropenia (66.7%), infection (49.6%), fatigue (42.9%), and stomatitis (31.3%; Table S4). The most frequently reported palbociclib-related TEAEs were neutropenia (66.7%), fatigue (35.3%), and stomatitis (26.6%; Table 3). Neutropenia was reported as a palbociclib-related grade 3 or 4 TEAE in 158 patients (62.7%) in the AT population and in 102 (67.1%) and 56 (56%) patients in the Australian and Indian cohorts, respectively. There were no reports of all-causality or palbociclib-related lymphopenia. Among patients in the Australian cohort who received ≥2 lines of therapy in the metastatic setting, neutropenia (74.4%), infections (53.5%), and fatigue (51.2%) were the most frequently reported all-causality TEAEs, whereas neutropenia (74.4%) and fatigue (44.2%) were the most frequently reported palbociclib-related AEs (Supplementary Table S5). Palbociclib-related grade 3 or 4 neutropenia was reported in 31 patients (72.1%).
A total of 91 patients (36.1%) had a dose reduction for palbociclib due to an AE; the most frequently reported AEs associated with dose reduction (in ≥2% of patients) were neutropenia (31.7%) and infections (2.4%). In the Indian cohort, 14 patients (14%) had a dose reduction due to neutropenia compared with 66 patients (43.4%) in the Australian cohort. A total of 188 patients (74.6%) had a dose interruption for palbociclib and/or letrozole due to an AE; the most frequently reported AEs associated with dose interruption (in ≥5% of patients) were neutropenia (60.3%), infections (13.9%), leukopenia (6.0%), and thrombocytopenia (5.2%). Eight patients (3.2%) were permanently discontinued from the study because of AEs, five (2.0%) of whom discontinued because of a palbociclib-related AE (one patient each: headache, liver function test increased, malaise, neutropenia, and pneumonitis [grade 2; considered palbociclib-related by investigator]).
A total of 63 patients experienced all-causality SAEs; the most frequently reported (≥3% of patients) were infections (7.5%) and disease progression (3.2%). Palbociclib-related SAEs were reported in 20 patients (7.9%); the most frequently reported SAEs (≥2% of patients) were febrile neutropenia (2.4%) and infections (2.0%). A total of 10 on-study deaths occurred (up to 28 days after the last dose of study drug). Eight patients died from disease progression, including three patients who died during the study treatment period, one died following an increased liver function test of unknown cause (considered palbociclib-related by the investigator), and one from multiple organ dysfunction syndrome due to an underlying condition.
3.3 Laboratory parametersThe most frequent grade 3 hematology abnormalities observed were reduction in absolute neutrophils (52.8% of patients) and white blood cells (39.7% of patients; Table S6). Grade 4 abnormalities included reduced absolute neutrophils (11.1% of patients), reduced platelets (2.0% of patients), and reduced white blood cells (1.6% of patients). Shifts from baseline grade ≤2 to postbaseline grade 3 and grade 4 for reduced absolute neutrophils were reported for 52.8% and 11.1% of patients, respectively. A shift from baseline grade ≤2 to postbaseline grade 3 anemia was reported for 8.7% of patients. There were no significant reports of lymphopenia.
3.4 Best overall tumor responseThe observed OR rate (based on investigator assessment) was 19.4% (95% CI, 14.7–24.9) for the total population, including three patients with complete response (Table 4). In the India cohort, the OR rate was 29.0% (95% CI, 20.4–38.9), and in the Australia cohort, OR rate was 13.2% (95% CI, 8.2–19.6). Australian patients with ≥2 lines of prior therapy for metastatic disease (n = 43) had an observed OR rate of 2.3%; a best response of partial response was reported in one patient; stable disease was reported in 22 patients (51.2%), and 16 patients (37.2%) had progressive disease.
TABLE 4. Best overall tumor response (AT population) Response Palbociclib + Letrozole Australian Cohort (n = 152) Palbociclib + Letrozole Indian Cohort (n = 100) Palbociclib + Letrozole Total Cohort (N = 252) Complete response 2 (1.3) 1 (1.0) 3 (1.2) Partial response 18 (11.8) 28 (28.0) 46 (18.3) Stable/no response 96 (63.2) 34 (34.0) 130 (51.6) Objective progression 30 (19.7) 20 (20.0) 50 (19.8) Indeterminate response 6 (3.9) 17 (17.0) 23 (9.1) Objective responseb 20 (13.2) 29 (29.0) 49 (19.4) 95% exact CI 8.2–19.6 20.4–38.9 14.7–24.9 Abbreviation: AT, as-treated. Note. All values are presented as n (%). 3.5 Patient-reported health-related quality of lifeA total of 146 patients (96.1%) in the Australia cohort were included in the PRO-evaluable population. The percentage of patients completing ≥1 question on the EQ-5D from Cycle 1 to Cycle 38 ranged from 90.9% to 100.0% (AT population). The percentages of patients on treatment who completed ≥1 question on the survey at 6 months and 1 year were 99% and 100%, respectively. Change from baseline in EQ-5D health utility index score and in EQ-5D VAS score showed that general and overall health status, respectively, were maintained during treatment with palbociclib plus letrozole (Figure 1).

Change from baseline in (A) EQ-5D Health Utility Index Score and (B) EQ-5D Visual Analog Scale Score (PRO-evaluable population). EQ-5D, European Quality of Life-5 Dimensions; PRO, patient-reported outcome; SE, standard error
4 DISCUSSIONThis expanded access program study showed that palbociclib plus letrozole was generally well tolerated in postmenopausal women with HR+/HER2– ABC in Australia and India for whom letrozole therapy was deemed appropriate. The observed OR in the total population was 19.4%. AEs were consistent with the known safety profile of palbociclib plus letrozole. Neutropenia was the most frequently reported palbociclib-related grade 3/4 TEAE. Although neutropenia was nearly universal, fever and infection were uncommon, supporting a different mechanism underlying the development of neutropenia compared with that caused by chemotherapy, with more rapid recovery upon withdrawal of palbociclib. Overall quality of life was maintained with palbociclib treatment. As this was an expanded access protocol, PFS and OS data were not included in the study objectives; thus, these data were not collected.
Of note, patient enrollment in India began 1 year after Australia, and palbociclib became commercially available earlier in India than in Australia. Therefore, Australian patients had a longer duration of treatment with palbociclib than Indian patients (13.6 and 10.7 months, respectively), likely due to Indian patients coming off the study to receive the commercially available drug.
The observed OR rates were 13.2% and 29.0% in the Australian and Indian cohorts, respectively. The lower OR rate for the Australian cohort was likely due to the higher number of patients in this cohort who received prior systemic treatment in the metastatic disease setting compared with the Indian cohort; including 28.3% of patients who received >1 line of therapy for metastatic disease. Moreover, many of the women in the Australian cohort had been treated with endocrine therapy before receiving palbociclib combination therapy in this study (63.2%); 54.3% of women in the Indian cohort had received prior endocrine therapy in the metastatic disease setting. Australian patients who had received ≥2 lines of prior therapy for metastatic disease had an observed OR rate of 2.3%; thus, patients who received more extensive systemic treatment in the advanced/metastatic setting before study enrollment likely contributed to the OR rate in the total Australian cohort. In the Indian cohort, 69.0% of patients had de novo metastatic disease, compared with only 38.2% of patients in the Australian cohort. The difference in the number of previous lines of metastatic th
留言 (0)