
記住我

Lumbar disc herniation (LDH) is a major cause of lower back pain and sciatica, resulting in a massive socioeconomic burden worldwide1, 2. Microdiscectomy (MD), which is regarded as an acceptable surgical procedure to treat LDH, is commonly used to treat LDH in western countries3, 4. Percutaneous endoscopic lumbar discectomy (PELD) techniques have become well-developed in the last few decades5-7, with discectomy with the Yeung endoscopic spine system (YESS), transforaminal endoscopic spine system (TESSYS), and full-endoscopic discectomy via the transforaminal approaches being the most popular5-7. Even with advances in these PELD techniques, the working cannula needs to be established with the aid of intervention technique during both YESS and TESSYS techniques, increasing the intraoperative fluoroscopy time. Traditional PELD techniques performed under local anesthesia are often uncomfortable, with terrible intraoperative experience for the patients. In addition, it is difficult to perform discectomy at L5–S1 and above with traditional full-endoscopic discectomy via the transforaminal approaches due to the iliac crest 7-9.
To overcome the shortcomings of these PELD techniques, a newly developed procedure called full-endoscopic visualized foraminoplasty and discectomy (FEVFD) has been developed to treat LDH10, 11. Compared with the above mentioned traditional PELD techniques, FEVFD was performed with excellent endoscopic visualization under general anesthesia, enabling safe and adequate decompression of the nerve root and the spinal canal10. All patients who underwent FEVFD had reasonable intraoperative experience under general anesthesia10. It was demonstrated that FEVFD resulted in significant improvements in pain scores and low complication rates for the treatment of L4-L5 and L5-S1 disc herniation under general anesthesia10.
Traditional PELD techniques and MD have been compared in previous studies; these studies reported that both traditional PELD techniques and MD are safe and effective surgical procedures in treating LDH12-16. However, to the best of our knowledge, there have not been any studies comparing FEVFD with traditional surgical techniques, such as MD. Therefore, patients with LDH treated by either FEVFD or MD were retrospectively analyzed in the present case–control study. The purpose of the present study was to: (i) describe FEVFD and MD for the treatment of single-level LDH; (ii) evaluate the efficacy and feasibility of FEVFD and MD for the treatment of single-level LDH; and (iii) to compare the clinical outcomes of FEVFD and MD for the treatment of single-level LDH.
Materials and methods Inclusion and Exclusion CriteriaThe inclusion criteria were as follows: (i) single-level LDH; (ii) unilateral radiating leg pain, with or without positive Lasegue's sign; (iii) failure of standard conservative treatment for at least 12 weeks; and (iv) herniated disc verified by magnetic resonance imaging (MRI) and computed tomography (CT), in accordance with the clinical symptoms and signs.
The exclusion criteria were as follows: (i) aged >65 or < 18 years; (ii) a history of lumbar surgery; (iii) LDH combined with other spinal disorders requiring surgery, such as spinal canal stenosis or lumbar spondylolisthesis; (iv) LDH at two or more segments; (v) a progressive neurological deficit, such as cauda equina syndrome, needing urgent surgical intervention; and (vi) LDH combined with serious diseases that contraindicate general anesthesia and surgery.
Patient Data and Ethics StatementData from 198 patients who presented with LDH between January 2016 and December 2017 treated using either FEVFD or MD under general anesthesia were retrospectively analyzed. These patients were categorized into either an FEVFD group or an MD group according to the surgical procedure performed. This study was approved by the Ethics Committee of Tongji Medical College, Huazhong University of Science and Technology. Written informed consent was provided by all participants.
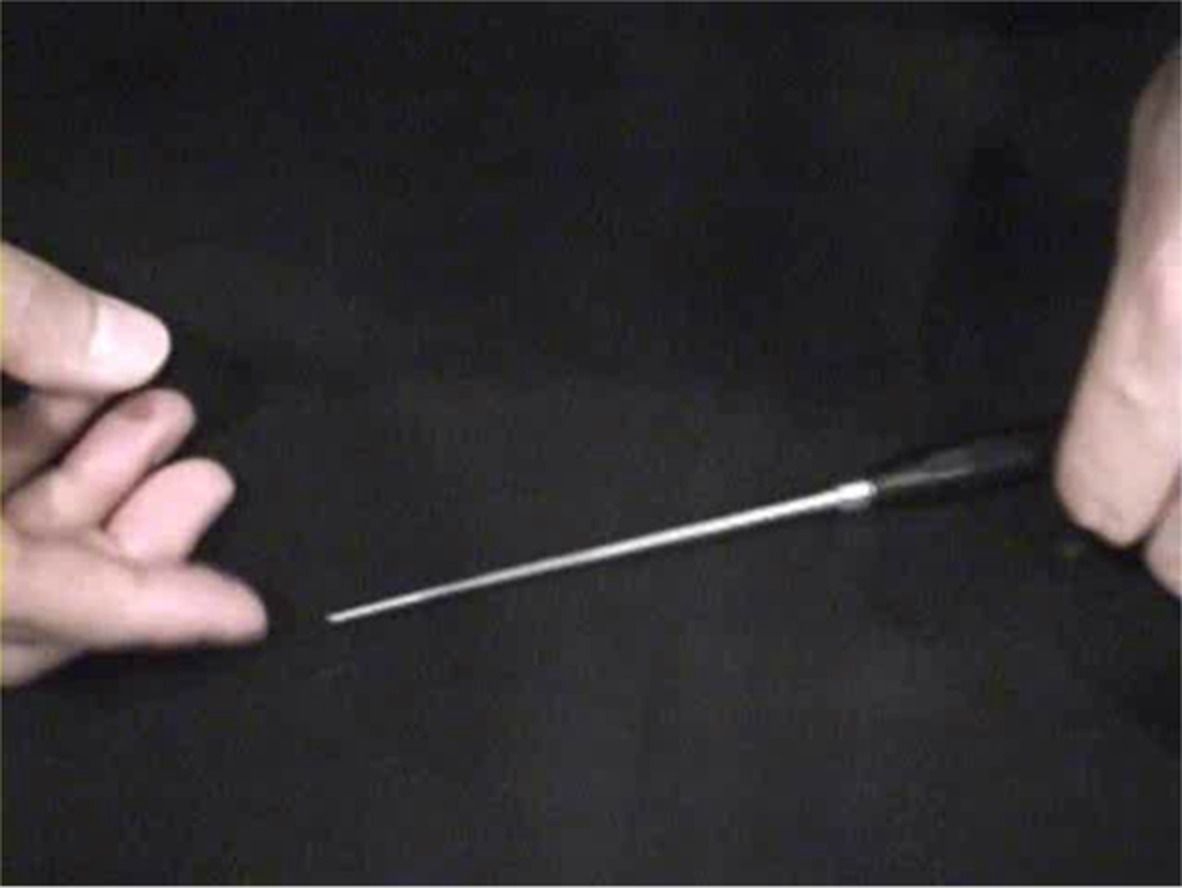
Surgical Technique FEVFDThe surgery was performed under general anesthesia in a prone position. The FEVFD procedure was performed using the surgical technique described by Hua et al.10. The intervertebral gap and foramina were located by posteroanterior and lateral fluoroscopy. The entry point of the assumed approach was 12–14 cm lateral to the spinal middle line above the iliac crest (Fig. 1)10. After inserting the puncture rod toward the intervertebral foramina, the surgical level and location of the puncture rod was confirmed by both posteroanterior and lateral fluoroscopy10. The working cannula and endoscopic surgical system (Spinendos, Munich, Germany) were then inserted toward the intervertebral foramina along the puncture rod10. All subsequent steps, including foraminoplasty, annulus fibrosus fenestration, and discectomy were performed under constant irrigation with excellent endoscopic visualization10. Before ending the operation, we confirmed that there was adequate decompression of the nerve root, the freed nerve root could be identified, and there was no free disc tissue or active bleeding (Fig. 2)10.

Full-endoscopic visualized foraminoplasty and discectomy was performed under general anesthesia in prone position. The entry point of the assumed approach was 12–14 cm lateral to the spinal middle line above the iliac crest.

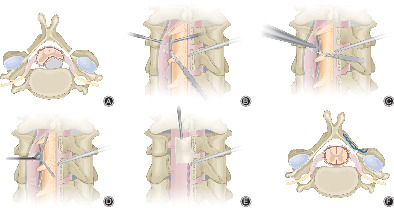
Surgical procedures of full-endoscopic visualized foraminoplasty and discectomy. A and B, Working cannula established along the foramina, and full-endoscopic visualized foraminoplasty performed. C and D, Working cannula directed toward the annulus fibrosus opening. E, F, G and H, Full-endoscopic visualized discectomy performed. I and J, Adequate decompression of the nerve root was ensured.
MDThe surgery was performed under general anesthesia in prone position. Lateral fluoroscopy was used to locate the intervertebral gap. The lamina and ligamentum flavum of the affected level was exposed via a 25 mm posterior midline incision. A minimally invasive lumbar Casper retractor was then applied, and part of the lamina and ligamentum flavum was removed using a Kerrison under direct microscopic (Zeiss, Jena, Germany) visualization. Subsequently, a discectomy was performed under direct microscopic visualization, ensuring complete decompression of the nerve root (Fig. 3).

Surgical procedures of microdiscectomy. A, ligamentum flavum (̂) exposed. B, Nerve root (*) ensured adequate decompression.
Clinical Outcome AssessmentOperative time, fluoroscopy time, postoperative time in bed, hospitalization time, complications, and reoperations were recorded for each patient.
Visual Analog ScalesThe Visual Analog Scale (VAS) for leg and back pain, was used to evaluate the pain level of patients. The VAS scoring system was self-completed by the patient. Patients marked a location on the 10-cm line corresponding to the amount of pain they experienced. 0 indicated no pain and 10 the most severe pain.
Oswestry Disability IndexOswestry Disability Index (ODI) is a principal condition specific outcome measure used to assess patient progression in routine clinical practice. The ODI score system was divided into 10 sections: pain intensity, personal care, lifting, walking, sitting, standing, sleeping, sex life, social life, and traveling. Each section was scored 0–5. If all 10 sections were completed the score was calculated as follows: total score out of total possible score ×100. If one section was missed (or not applicable), the score was calculated as: (total score/(5 × number of questions answered)) × 100%. Scores were as follows: 0%–20% was considered mild dysfunction; 21%–40% was moderate dysfunction; 41%–60% was severe dysfunction; 61%–80% was considered as disability, and 81%–100% was considered as either bedridden for long-term or exaggerating the impact of pain on their life.
36-Item Short-Form Physical Function and Bodily Pain Health SurveyThe MOS 36-Item Short-Form health survey (SF36) includes multi-item scales that assess eight health concepts: physical functioning (PF), bodily pain (BP), role limitations due to physical problems, general health, vitality, social functioning, role limitations due to emotional problems, mental health, and perceptions17-19. The interpretation of the SF-36 has been made much easier with the standardization of mean scores and standard deviations for all SF-36 scales19. It can be illustrated by comparing the SF-36 profile scored using the original 0–100 scoring algorithms based on the summated ratings method and the norm-based scoring algorithms19. SF36-PF and SF36-BP were evaluated preoperatively and postoperatively.
Modified MacNab CriteriaThe modified MacNab criteria was also used to evaluate clinical outcomes. The results were classified as excellent, good, fair or poor: excellent indicated no pain and no restriction of movement, allowing the patient to work normally; good indicated occasional pain, allowing the patient to work normally; fair indicated slight progress; poor indicated no progression 20.
Statistical AnalysisData are presented as mean ± standard deviation. SPSS 22.0 software (IBM Corp., Armonk, NY, USA) was used to perform the statistical analyses, and GraphPad Prism 6 software (Graph Pad Software, Inc., San Diego, CA, USA) was used to generate plots. Normal distribution of the data was assessed using the Kolmogorov–Smirnov test. Nonparametric data were analyzed by the Mann–Whitney U test or the Wilcoxon signed-rank test. A P-value of less than 0.05 was considered statistically significant.
Results General ResultsDemographic data and baseline characteristics of the patients in the two groups are summarized in Table 1. The age, sex, body mass index (BMI), type of disc herniation, and surgical levels of the two groups were not statistically different.
TABLE 1. Baseline characteristics of patients in the two groups FEVFD group MD group P N 102 96 - Age (years) 40.05 ± 12.79 41.62 ± 11.35 0.379 Sex (male) 75 (73.53%) 65 (67.71%) 0.370 BMI (kg/m2) 23.28 ± 3.21 23.47 ± 3.28 0.656 Type of disc herniation 0.522 Central 24 (23.53%) 21 (21.88%) - Paracentral 73 (71.57%) 67 (69.79%) - Far lateral 5 (4.90%) 8 (8.33%) - Surgical segment 0.943 L3-L4 or above 2 (1.96%) 4 (4.17%) - L4-L5 67 (65.69%) 59 (61.46%) - L5-S1 33 (32.35%) 33 (34.37%) - BMI, Body mass index; FEVFD, full-endoscopic visualized foraminoplasty and discectomy; MD, microdiscectomy.The mean operative times, fluoroscopy times, postoperative times in bed, and hospitalization times for each of the two groups are summarized in Table 2. The mean postoperative time in bed, and hospitalization time of the MD group were significantly longer than those of the FEVFD group, while the operative time, and fluoroscopy time of the MD group was significantly shorter than that of the FEVFD group. Representative cases of FEVFD group are presented in Figs 4 and 5, and the representative case of MD group is presented in Fig. 6.
TABLE 2. Comparison of operative time, fluoroscopy time, postoperative bed time and hospitalization time in the two groups FEVFD group MD group P N 102 96 - Operative time (minutes) 73.82 ± 20.73 64.74 ± 17.37 0.003 Fluoroscopy time (seconds) 1.71 ± 0.58 1.30 ± 0.33 <0.001 Postoperative time in bed (hours) 8.51 ± 2.10 9.24 ± 2.01 0.014 Hospitalization time (days) 2.89 ± 0.83 4.94 ± 1.35 <0.001 FEVFD, full-endoscopic visualized foraminoplasty and discectomy; MD, microdiscectomy.
Full-endoscopic visualized foraminoplasty and discectomy under general anesthesia performed on a 25-year-old male patient diagnosed with L4-L5 disc herniation. A and B, preoperative magnetic resonance imaging (MRI) scans. C, preoperative computed tomography (CT) scans. D and E, full-endoscopic visualized foraminoplasty performed with the aid of a direction-variable drill, and the foramina was exposed. F and G, full-endoscopic visualized discectomy was performed. H, a radiofrequency electrode is applied to control bleeding. I and J, the traversing nerve root were exposed, and sufficient decompression of the traversing nerve root was ensured. K and L, MRI scans 3 months after the surgery. Snowflake (*), nerve root, triangle (^), dural sac.

Full-endoscopic visualized foraminoplasty and discectomy under general anesthesia performed on a 49-year-old male patient diagnosed with L4-L5 disc herniation. A and B, preoperative magnetic resonance imaging (MRI) scans. C, preoperative computed tomography (CT) scans. D and E, full-endoscopic visualized foraminoplasty performed with the aid of a direction-variable drill, and the foramina was exposed. F and G, full-endoscopic visualized discectomy was performed. H, a radiofrequency electrode is applied to control bleeding. I and J, the traversing nerve root were exposed, and sufficient decompression of the traversing nerve root was ensured. K and L, MRI scans 3 months after the surgery. Snowflake (*), nerve root, triangle (^), dural sac.

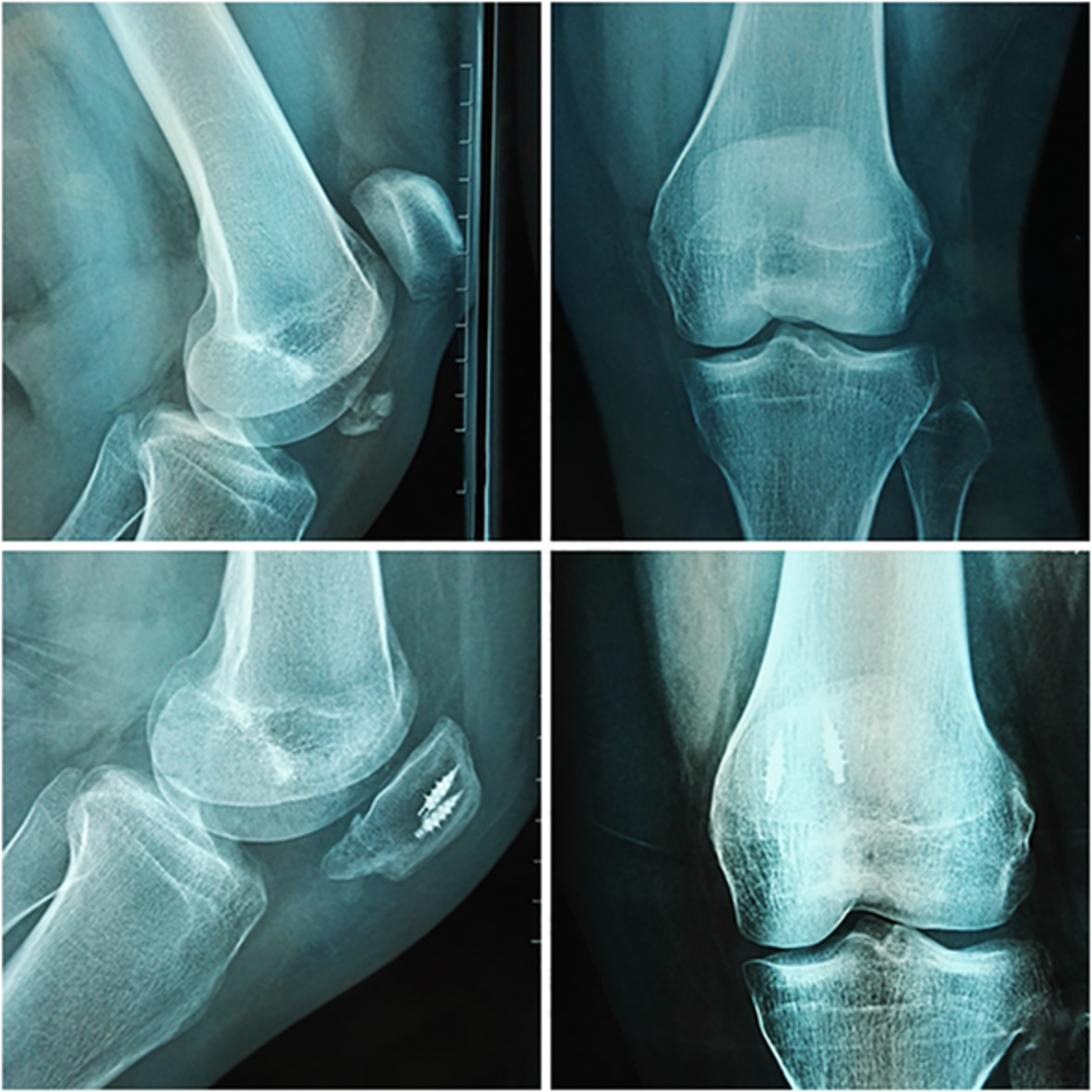
Microdiscectomy under general anesthesia performed on a 26-year-old male patient diagnosed with L5-S1 disc herniation. A and B, preoperative magnetic resonance imaging (MRI) scans. C, preoperative computed tomography (CT) scan. D and E, postoperative MRI scans 1 week after the surgery. F, postoperative CT scan 1 week after the surgery. G and H, postoperative MRI scans 12 months after the surgery. postoperative CT scan 15 months after the surgery.
Functional Evaluation VASThe mean preoperative and postoperative scores for the VAS for leg and back pain, for the FEVFD group were not significantly different from the scores for the MD group. However, the mean VAS scores for leg and back pain at each follow-up decreased significantly following surgery for both groups.
ODIThe mean preoperative and postoperative ODI scores for the FEVFD group were not significantly different from the scores for the MD group. However, the mean ODI score at each follow-up decreased significantly following surgery for both groups.
SF36-PF and SF36-BPThe mean preoperative and postoperative scores for SF36-PF and SF36-BP for the FEVFD group were not significantly different from the scores for the MD group. Conversely, the SF36-PF and SF36-BP scores at each follow-up increased significantly following surgery for both groups (Table 3, Fig. 7).
TABLE 3. Comparison of VAS scores, ODI scores, SF36-PF scores and SF36-BP scores in the two groups Variables FEVFD group MD group P N 102 96 - VAS score for leg pain pre-op 7.31 ± 1.35 7.48 ± 1.20 0.516 3 months post-op 1.85 ± 0.75* 1.78 ± 0.73* 0.491 6 months post-op 1.64 ± 0.48* 1.57 ± 0.50* 0.356 12 months post-op 1.52 ± 0.54* 1.44 ± 0.54* 0.267 24 months post-op 0.96 ± 0.48* 0.93 ± 0.46* 0.625 VAS score for back pain pre-op 3.75 ± 0.89 3.61 ± 0.74 0.370 3 months post-op 1.88 ± 0.62* 1.97 ± 0.72* 0.398 6 months post-op 1.72 ± 0.62* 1.64 ± 0.62* 0.351 12 months post-op 1.54 ± 0.54* 1.49 ± 0.54* 0.494 24 months post-op 1.08 ± 0.66* 1.02 ± 0.60* 0.502 ODI score pre-op 46.38 ± 9.38 47.38 ± 9.29 0.367 3 months post-op 16.20 ± 5.15* 16.48 ± 5.02* 0.762 6 months post-op 15.45 ± 4.28* 15.69 ± 4.10* 0.788 12 months post-op 14.87 ± 4.03* 15.07 ± 3.86* 0.806 24 months post-op 12.46 ± 4.51* 12.99 ± 4.29* 0.323 SF36-PF score pre-op 49.70 ± 13.87 50.36 ± 14.20 0.547 3 months post-op 85.49 ± 8.91* 85.94 ± 9.01* 0.648 6 months post-op 91.47 ± 4.70* 91.51 ± 4.87* 0.940 12 months post-op 94.61 ± 4.08* 94.84 ± 4.13* 0.682 24 months post-op 96.37 ± 3.99* 96.77 ± 4.04* 0.410 SF36-BP score pre-op 44.28 ± 22.74 43.80 ± 23.36 0.837 3 months post-op 85.37 ± 11.94* 85.85 ± 11.82* 0.566 6 months post-op 89.39 ± 6.25* 89.98 ± 6.18* 0.276 12 months post-op 92.43 ± 6.72* 92.64 ± 6.85* 0.767 24 months post-op 94.65 ± 6.78* 95.00 ± 6.82*
留言 (0)