
記住我

Cervical spondylotic myelopathy (CSM) is one of the most common causes of numbness, muscle weakness, unstable walking and localized pain around the shoulders. It gradually develops when degenerative changes, mainly caused by long-term cervical strain, hyperosteogeny, intervertebral disc herniation and ligament thickening, result in spinal cord compression and dysfunction, leading to a series of clinical symptoms1. Early surgical treatment can avoid the occurrence of spinal cord injury when there is no obvious improvement after conservative treatment for more than 3 months2. For the time being, ACDF and CLF are the two most widely used surgical procedures in treating CSM.
In ACDF, the herniated disc and bony spur is exposed and removed by making an incision from the anterior of the neck and moving aside the muscles, thus preserving adjacent muscular and other soft tissues and relieving the compression in front of spinal cord and nerve root. The disadvantage is that the fusion of surgical segments will accelerate adjacent segments degeneration and reduce the cervical range of motion3. CLF expands the spinal canal and relieves the compression indirectly by removing the lamina and cause the spinal cord to withdraw as a bowstring. However, high incidence of postoperative axial symptoms is one of the disadvantages4, and another one is the limited decompression effect when kyphosis is combined.
It remains controversial whether ACDF or CLF is to be recommended for multilevel CSM5. Up to now, most of the investigations are related to 2-level or 3-level CSM, and 4-level CSM is rarely discussed. This study included only 4-level CSM patients, trying to explore the clinical outcomes of different surgical methods in 4-level CSM.
Materials and Methods Inclusion CriteriaInclusion criteria for this study included: (i) patients diagnosed with C3-7 cervical spondylotic myelopathy with ineffective conservative treatment for more than 3 months; and responsible segments were confirmed by CT and MRI; (ii) patients who underwent ACDF or CLF; (iii) intraoperative blood loss, operation time, visual analogue scale (VAS) of axial pain, Japanese Orthopedic Association (JOA) score, Cobb angle, Cobb angle improvement rate, range of motion (ROM), ROM loss ratio and complications were compared; (iv) follow-up results of the patients were recorded; and (v) a clinical retrospective research.
Exclusion CriteriaExclusion criteria included: (i) fracture, tumor, tuberculosis, spinal cord injury, deformity; (ii) severe lung, heart disease or other surgical contraindications; and (iii) spinal operation history.
Patient PopulationA total of 39 patients with CSM who had undergone ACDF or CLF in the Third Hospital of Hebei Medical University from 2010 to 2018 were included. Of the 39 patients involved, 21 patients were treated with ACDF (group ACDF), and 18 patients received CLF (group CLF) (Figs 1, 2).

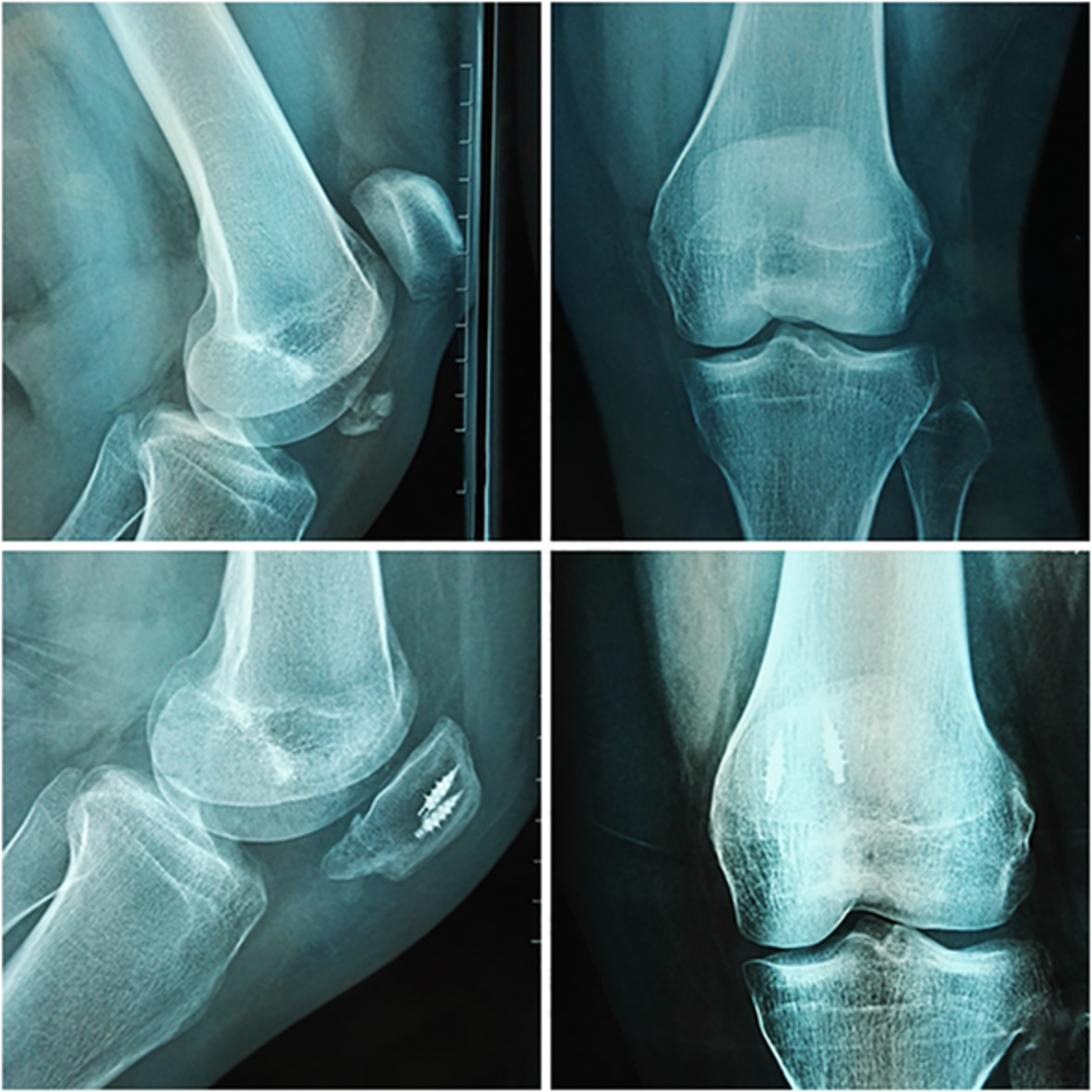
Two cases of ACDF surgery. Notes: Patient 1: (A1–F1). Patient 2: (A2–F2). Preoperative lateral position X-ray radiograph indicate the bone structure of cervical vertebrae (A1, A2); preoperative MRI and CT indicate the compression from disc herniation and osteophyte (B1, C1 and B2, C2); the sufficient decompression of the spinal cord was shown in postoperative MRI (E1, E2) and the X-ray radiographs immediately and 2 years after surgery show the internal fixation position and cervical curvature (D1, D2 and F1, F2).

Two cases of CLF surgery. Notes: Patient 1: (A1–F1). Patient 2: (A2–F2). Preoperative lateral position X-ray radiograph indicate the bone structure of cervical vertebrae (A1, A2); preoperative MRI and CT indicate the compression from disc herniation and osteophyte (B1, C1 and B2, C2); the sufficient decompression of the spinal cord was shown in postoperative MRI (E1, E2) and the X-ray radiographs immediately and 2 years after surgery show the internal fixation position and cervical curvature (D1, D2 and F1, F2).
Surgical ProcedureFor the ADF technique, the patient was in supine position and underwent general anesthesia. Lateral fluoroscopy was used to confirm the correct level. Incision was performed using a right-sided approach at an appropriate cervical level. Following the division of platysma, blunt dissection was performed up to deep prevertebral fascia. After a second fluoroscopy, the hyperplastic osteophyte, degenerative discs and posterior longitudinal ligament were removed. The cages filled with bone fragments were inserted into the C3-6 Intervertebral space. The C3-6 vertebral body was fixed by the titanium plate, and a Zero-Profile spacer was inserted into C6-7. The incision was closed and a cervical collar was placed.
For CLF the patient was initially positioned in a prone position and underwent general anesthesia. The operative level was identified with lateral fluoroscopy. An open midline approach with bilateral muscle strip dissection was used to access the posterior column of the vertebral body. A total of 10 lateral mass screws and two connecting rods were secured to the C3-7 lateral mass. The spinous process and bilateral lamina of C3-7 were removed. A final lateral fluoroscopy confirmed the correct positioning of the screws and rods. The autogenous bone was placed outside the screws. Wound closure consisted of eight to 10 fascial sutures and subcutaneous stitches.
Observation Index and Efficacy EvaluationBaseline and postoperative patient-reported outcomes including age, sex, body mass index, follow-up time, operation time, intraoperative blood loss, perioperative complications were captured.
Radiographic EvaluationThe anterior–posterior and lateral X-ray, cervical CT scan and MRI were taken before and 2 years after the surgery.
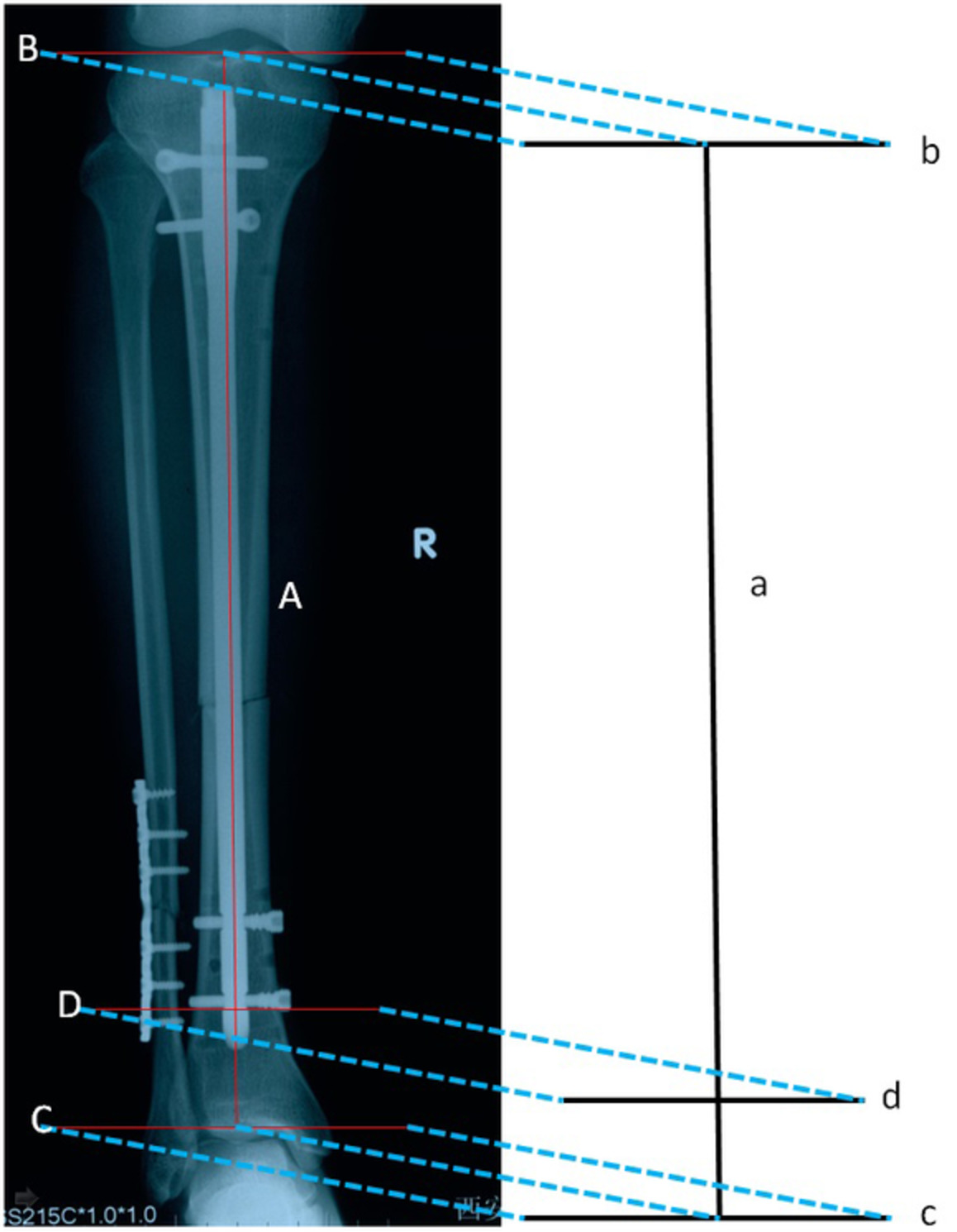
C3-7 Cobb AngleThe C3-7 Cobb angle indicates the angle between two crossed perpendicular lines that are extended parallel to the superior endplate of C3 and inferior endplate of C7 on the standing lateral radiograph of the cervical spine, which was used to quantify the magnitude of spinal deformities.
Cervical Range of Motion (ROM)Cervical ROM is the measurement of the amount of movement of cervical vertebrae, which was calculated as follows: C3-7 Cobb angle in extension, C3-7 Cobb angle in flexion.
ROM Loss RatioThe ROM loss ratio was calculated as: preoperative ROM- postoperative ROM)/preoperative ROM.
Functional EvaluationThe visual analogue scale (VAS) of axial pain and Japanese Orthopedic Association (JOA) score were adopted 1 day prior to surgery and 2 years after surgery.
Visual Analogue ScaleThe VAS is a subjective measure for acute and chronic pain. Scores are recorded by making a handwritten mark on a 10-cm line that represents a continuum between 0 and 10. 0 is defined as “no pain,” 1–3 as “mild pain,” 4–6 as “moderate pain,” 7–9 as “severe pain,” and 10 as “the worst imaginable pain.”
Japanese Orthopedic Association ScoreThe JOA score is a disease-specific and physician-oriented scale which was designed to assess the neurological status of patients. This scale consists of six domain scores (motor dysfunction in the upper extremities, motor dysfunction in the lower extremities, sensory function in the upper extremities, sensory function in the trunk, sensory function in the lower extremities, and bladder function), scaled from 0 to 4, 4, 2, 2, 2, and 3, respectively, with the minimum total score being 0 and the maximum total score being 17. The myelopathy severity was defined as mild if the JOA score is larger than 13, as moderate if the JOA score ranges from 9 to 13 and as severe if the JOA score is less than 9.
Rate of the JOA Score ImprovementThe rate of the JOA score improvement was used to assess the severity of clinical symptoms in patients with cervical compressive myelopathy and calculated as: (postoperative score–preoperative score)/(17–preoperative score) × 100%.
Statistical MethodsThe Student's t test, The Wilcoxon test, Mann–Whitney test, Pearson Chi Square and Fisher's exact test were used when appropriate to test the significance of the differences within and between the groups. Data were analyzed using the SPSS (SPSS Statistics 25.0, IBM Inc., Chicago, IL, USA) software program for Windows. Statistical significance was set at P < 0.05. Results are given as mean values and standard deviation.
Results Baseline and Clinical OutcomesThe baseline characteristics of the patient population were summarized in Table 1. A total of 39 patients (24 men) were involved for analysis, of which 21 (53.80%) underwent ACDF and 18 (46.20%) underwent CLF. The average age at baseline was 55 years. There were no significant differences in sex, age, body mass index, and follow-up time (P > 0.05). Blood loss in the CLF group was significantly higher than that in the ACDF group (692.67 ± 38.68 vs 392.14 ± 128.06, P < 0.05). The operation time in CLF was significantly longer than that in ACDF group (206.60 ± 49.37 vs 172.64 ± 31.96, P < 0.05). No reoperation or revision surgeries were performed during follow-up.
TABLE 1. Patient demographic data Variable ACDF CLF P-value Patients (cases) 21 18 Age (years) 53.94 ± 7.69 57.02 ± 10.48 0.298 * Sex (male, female) 13, 8 11, 7 1.000 † Body mass index (kg/m2) 21.53 ± 2.46 20.89 ± 3.04 0.930 ‡ Follow-up (months) 26.29 ± 1.62 25.39 ± 1.46 0.075 ‡ ACDF, anterior cervical discectomy and fusion; CLF, cervical laminectomy and fusion. Radiographic Evaluation OutcomesThe radiographic outcomes of the patients are shown in Table 2.
TABLE 2. Patient clinical and radiologic outcomes Variable ACDF CLF P-value (n = 21) (n = 18) Blood loss, mL 392.14 ± 128.06 692.67 ± 38.68 <0.001 * Operation time (min) 172.64 ± 31.96 206.60 ± 49.37 0.014 † Preoperative axial VAS 3.43 ± 0.98 3.28 ± 0.89 0.580 * VAS at final follow-up 2.10 ± 0.70 ‡ 1.94 ± 0.73 ‡ 0.510 * Preoperative JOA scores 10 ± 2.14 9.5 ± 1.54 0.416 † JOA scores at final follow-up 14.10 ± 1.45 ‡ 11.72 ± 1.96 ‡ <0.001 * JOA scores improvement rate (%) 60.9 ± 9.57 31.5 ± 15.70 <0.001 † Preoperative Cobb angle (°) 13.72 ± 5.83 12.56 ± 7.78 0.598 † Postoperative Cobb angle (°) 16.70 ± 6.56 ‡ 15.53 ± 8.43 ‡ 0.629 † Cobb angle improvement rate (%) 2.98 ± 1.34 2.97 ± 1.81 0.526 * Preoperative cervical ROM (°) 41.16 ± 9.77 42.84 ± 8.28 0.554 * Postoperative cervical ROM (°) 27.80 ± 1.51 ‡ 28.44 ± 10.67 ‡ 0.530 * Cervical ROM loss ratio (%) 28.03 ± 20.87 32.98 ± 23.08 0.822 * ACDF, anterior cervical discectomy and fusion; CLF, cervical laminectomy and fusion; JOA, Japanese Orthopedic Association; VAS, visual analogue scale; ROM, range of motion. C3-7 Cobb AngleCobb angle improved significantly after operation in the ACDF group (16.70° ± 6.56° vs 13.72° ± 5.83°, P < 0.05). And in the CLF group, the cobb angle was also better compared with preoperative index (15.53° ± 8.43° vs 12.56° ± 7.78°, P < 0.05). No difference was identified between the two groups in Cobb angle (P > 0.05). Regarding Cobb improvement, there was no differences between cohorts (2.98° ± 1.34° vs 2.97° ± 1.81°, P > 0.05).
Cervical Range of Motion (ROM)The ROM reduced significantly after operation in the ACDF group (27.80° ± 1.51° vs 41.16° ± 9.77°, P < 0.05). And in the CLF group, the ROM was also worse than preoperative index (28.44° ± 10.67° vs 42.84° ± 8.28°, P < 0.05).
ROM Loss RatioRegarding ROM loss ratio, there were no differences between cohorts (28.03% ± 20.87% vs 32.98% ± 23.08%, P > 0.05).
Functional Evaluation OutcomesThe functional outcomes of the patients are shown in Table 2.
VASThe axial VAS improved significantly after operation in the ACDF group (2.10 ± 0.70 vs 3.43 ± 0.98, P < 0.05). And the axial VAS also improved significantly after operation in the CLF group (1.94 ± 0.73 vs 3.28 ± 0.89, P < 0.05). No difference was identified between the two groups in preoperative VAS and VAS at final follow-up (all P > 0.05).
JOA ScoreThe JOA score improved significantly after operation in the ACDF group (60.9 ± 9.57 vs 14.10 ± 1.45, P < 0.05). And the JOA score also improved significantly after operation in the CLF group (31.5 ± 15.70 vs 11.72 ± 1.96, P < 0.05). No difference was identified between the two groups in preoperative JOA score and JOA score at final follow-up (all P > 0.05).
Rate of the JOA Score ImprovementCLF patients reported significantly worse JOA score improvement rate as compared to ACDF patients (31.5% ± 15.70% vs 60.9% ± 9.57%, P < 0.05).
ComplicationsThe summary of complications is given in Table 3. In the ACDF group, two patients (9.6%) had postoperative complications, which included dysphagia (one case), pharyngodynia (one case). In the CLF group, two patients (11.1%) developed C5 palsy. No significant difference in the incidence rate of complications was found between group ACDF and group CLF. All the complications were relieved within 1 month.
TABLE 3. Complications Variables ACDF CLF (n = 21) (n = 18) Complications C5 palsy 0 2 (11.1%) Dysphagia 1 (4.8%) 0 CSF leakage 0 0 Hoarseness 0 0 Subsidence 0 0 Infection 0 0 Pharyngodynia 1 (4.8%) 0 Total 2 (9.6%) 2 (11.1%) ACDF, anterior cervical discectomy and fusion; CLF, cervical laminectomy and fusion; CSF, cerebrospinal fluid. Discussion BackgroundACDF has the advantages of decreased invasiveness, direct decompression and so on. Postoperative complications are also common, such as hoarseness, dysphagia, C5 nerve root paralysis, cerebrospinal fluid leakage, implant displacement and collapse6. CLF can relieve the compression from the rear, and the related complications are often C5 nerve root paralysis and axial pain C5 nerve root paralysis and axial pain. Currently, there is still enormous controversies over the treatment for multi-level cervical spondylosis. In this study, the outcome of patients undergoing different C3-7 surgical procedures were compared and analyzed, primarily for the purpose of exploring and deciding on the best surgical approach for 4-level cervical spondylosis.
Orthopedic AbilityThe physiological curvature of the cervical spine mainly functions to reduce and buffer the external shock. The straightening or the reversal of the cervical lordosis will accelerate the degeneration of the cervical spine and cause pains in the neck muscles7. An effective surgical correction of cervical curvature can relieve the tension of paravertebral muscles and delay cervical degeneration. In this study, no significant difference between research groups was found in Cobb angle improvement. Abdullah et al.'s research shows that the loss of spinous process, lamina and interspinous ligament will lead to the deterioration of cervical curvature8. Healy et al.'s study found that increased intervertebral activity after laminectomy may be associated with postoperative pain and cervical deformity9. However, the results of our research were contrary to their conclusions, which may be due to that in CLF operation, we preserved the occipital muscle and cervical hemi acanthus muscle of C2 segment as much as possible, as well as part of lamina of C2, so as to ensure the stability of cervical vertebra and reduce the incidence of kyphosis. In addition, posterior screws combined with rods are superior to the combination of screw and plate in correcting cervical curvature and maintaining spinal sequence.
Surgical Risk AssessmentThe majority of patients with cervical spondylotic myelopathy were over 40 years old. For elderly patients with complex underlying diseases and poor tolerance of surgeries, the size of surgical incision and the length of operation need to be minimized. For this respect, ACDF can provide better surgical outcomes since it involves smaller incision, shorter operation time, less bleeding, and no damage to the important anterior cervical muscle groups. In this research, the amount of blood loss and operation time in the ACDF group were significantly less than those in the CLF group. Before CLF operation, we will comprehensively evaluate the cardiovascular and cerebrovascular health of patients to prevent intraoperative adverse events during the operation. To address the problem of more bleeding with CLF, we routinely use the autologous blood recovery device (which filters the blood and return it back to patient's body during operation), which can, to a certain extent, stabilize the patient's blood pressure and reduce the risk of infection and rejection associated with allogeneic blood infusion. In addition, although there was less bleeding in ACDF, there was no treatment capacity for intraspinal hemorrhage. The time of posterior cervical operation was longer than that in ACDF group. Inconsistent with our findings, Shen et al.10 reported lower bleeding volume in ACDF than in CLF, but the length of operation was the same with both surgical techniques. In our research, the operation time of CLF group was longer than that reported by previous studies. This may be due to our careful lamina dissection in the whole process of laminectomy. In spite of prolonging the surgery, this can prevent the occurrence of spinal cord concussion, thus reducing the stimulation to spinal cord during operation.
Function EvaluationMost axial symptoms are accompanied by muscle tension and stiffness, which are generally attributed to muscle and nerve injuries during posterior surgery. However, there has been research evidence that patients with anterior surgery may also experience long-term axial pain after operation11. In this research, no significant difference in VAS score of axial pain was observed between the ACDF group and the CLF group. Most previous studies considered axial pain to be a frequent complication of posterior cervical surgery. In our study, however, there was no significant difference between ACDF and CLF, which might be due to our retention of attachment point of C2 extensor. Wang et al. pointed out that axial symptoms can be reduced by decreased surgical wound, utmost protection of cervical hemi acanthus muscle and early removal of external fixation12. The 4-segment anterior cervical surgery requires each segment be stretched for decompression and excessive stretch may aggravate the postoperative axial symptoms. In order to reduce the incidence of postoperative axial symptoms, we required patients to exercise the neck muscles earlier after surgery, which can reduce the atrophy of extensor muscles, muscle adhesion, and postoperative stiffness.
The common symptoms of cervical spondylotic myelopathy include increased muscle tension, active tendon reflex and Limb numbness. Efficacy and thoroughness of decompression determines the long-term prognosis of patients. The JOA score of ACDF group in our study was better than that of CLF group. In Houten's study, there was no significant difference in JOA scores between ACDF and CLF13. It is assumed that inconsistent results are caused by the following reasons. First, ACDF reduces compression in the targeted segment directly and causes less damages to muscles and bone structures. Second, in anterior cervical surgery, we normally used a microscope to assist the operation, which increased the surgical field clarity, leading to more adequate and accurate decompression.
ComplicationsC5 nerve root paralysis is usually manifested as deltoid weakness. Research has reported that C5 nerve root palsy was related to excessive spinal cord drift, intervertebral foramen stenosis14, OPLL and laminectomy15. Klement et al.'s study suggested that the width of laminectomy was not related to the risks of C5 paralysis and reducing the width of laminectomy may not reduce the incidence of postoperative paralysis16. Radcliff et al.'s study indicated that the degree of posterior spinal cord displacement was greater in patients with C5 nerve palsy, and the average posterior spinal cord displacement at C5 level was about 4.27 mm17. Kim and Lee raised the open side of the lamina and placed a suture from the base of the spinous process to the cap of the lateral mass screw to reduce the degree of spinal cord backward movement18. In meta-analysis of Wang et al., the incidence of C5 nerve root paralysis was 5.5% in ACDF and 12.2% in CLF19. In our experiment, the total incidence rates of C5 nerve root palsy in CLF group were 11.1%, which was consistent with previous research evidence20. For patients with C5-6 intervertebral foramen stenosis, we will avoid the excessive expansion of the intervertebral space during the operation. For postoperative C5 nerve root paralysis, we used dexamethasone for anti-inflammatory and anti-edema treatment, and in a short period of time, the muscle strength of the deltoid muscle of the patients were well recovered.
Pharyngeal pain and dysphagia are common complications after ACDF. The risk factors for dysphagia were revision surgery, smoking, older age, intraoperative rhBMP-2 use, cardiovascular or endocrine disorders21-23. Dysphagia occured in 83% of patients and were mostly self-limited24. Carucci et al. reported soft tissue swelling and esophageal displacement in 91% of patients25. The incidence of dysphagia in our groups with anterior cervical surgery was 4.8%, which might be due to the increase in area of exposure and in operation time. Meta-analysis showed that the incidence of dysphagia at 1, 3 and 6 months after surgery was significantly reduced in patients using Zero-Profile spacer26. Koreckij et al. significantly reduced the incidence of dysphagia by intraoperative local use of steroids to relieve pharyngeal pain and soft tissue swelling27. In order to reduce the incidence of dysphagia, we took the following measures: (i) auto-retractor rather than manual hook was applied during the operation, since the auto-retractor could produce constant pressure on paravertebral tissue and allow the operator to adjust the range of distraction; (ii) smoking was strictly prohibited during hospitalization; and (iii) The rhBMP-2 was not generally used by patients. If there were risk factors such as osteoporosis, dexamethasone would be used locally on the basis of rhBMP-2 and the dysphagia symptom was relieved within 2 weeks.
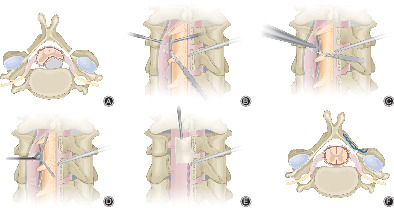
Surgical Technique ACDF Operative exposure: the larger operation space of 4-level ACDF makes that the blood vessels and nerves have a certain degree of activity after dissociation, because of which the blood vessels and nerves can be preserved as far as possible, thus reducing the potential risk of nerve injury, and also protecting the blood supply of adjacent tissues. Restoration of lordosis angle: the screw path can be inclined to the endplate, and when the vertebrae were stretched, a natural angle can be formed between the endplates. In addition, the curvature of the titanium plate should fit to the angle of the lordosis, instead of relying on the titanium plate to restore the angle of the lordosis, or the top and bottom screws are at a risk of loosening. In conclusion, the recovery of curvature depends on the angle of screws, suitable titanium plates and intraoperative position of patients. Decompression: it is not necessary to expose the posterior longitudinal ligament at every segment. For segments with high signal intensity of spinal cord, severe compression, and obvious instability, the posterior longitudinal ligament should be removed. For the segment with less compression, the posterior longitudinal ligament can be preserved, which also can shorten the operation time. Application of microscope: at the C3-4 segment, which is difficult to show clear vision, it is better to use microscope to assist operation (Fig. 3).
Schematic drawing illustrating ACDF and CLF. Notes: ACDF (A, B and C): The C3-6 were fixed with anterior screw-plate system and the C6-7 was inserted a Zero-Profile spacer. CLF (D, E and F): The C3-7 were fixed with posterior screw-rod system.
CLF When the orthopedic rod was inserted, we can restore the lordosis of the cervical spine by adjusting the operating table, rather than by using the screw rod alone to correct the kyphosis. Preventive nerve root decompression: for C4-5 intervertebral foramen, conventional enlargement can reduce the occurrence of C5 nerve root paralysis. The adhesions in epidural space should not be removed excessively. After the adhesions around the dura were removed, the spinal cord moved backward excessively, which may result in a transient injury of C5 nerve root (Fig. 3). Unresolved IssuesACDF cannot remove the compression behind the vertebral body, but Anterior cervical corpectomy decompression and fusion (ACCF) can remove part of the vertebral body and relieve the compression behind the vertebral bod
留言 (0)