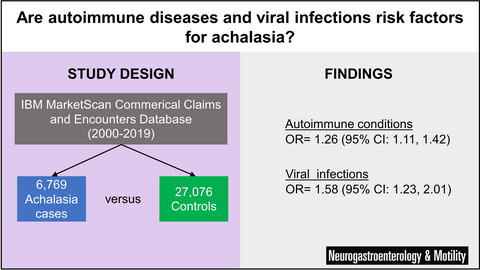
Fructose intolerance is not associated with malabsorption in patients with functional gastrointestinal disorders
Background
Symptoms following fructose ingestion, or fructose intolerance, are common in patients with functional gastrointestinal disorders (FGID) and are generally attributed to intestinal malabsorption. The relationships between absorption, symptoms, and intestinal gas production following fructose ingestion were studied in patients with FGID.
Methods
Thirty FGID patients ingested a single dose of fructose 35 g or water in a randomized, double-blind, crossover study. Blood and breath gas samples were collected, and gastrointestinal symptoms rated. Plasma fructose metabolites and short-chain fatty acids were quantified by targeted liquid chromatography-tandem mass spectrometry. Patients were classified as fructose intolerant or tolerant based on symptoms following fructose ingestion.
Key Results
The median (IQR) areas under the curve of fructose plasma concentrations within the first 2 h (AUC0–2 h) after fructose ingestion were similar for patients with and without fructose intolerance (578 (70) µM·h vs. 564 (240) µM·h, respectively, p = 0.39), as well as for the main fructose metabolites. There were no statistically significant correlations between the AUC0–2 h of fructose or its metabolites concentrations and the AUCs of symptoms, breath hydrogen, and breath methane. However, the AUCs of symptoms correlated significantly and positively with the AUC0–2 h of hydrogen and methane breath concentrations (r = 0.73, r = 0.62, respectively), and the AUCs of hydrogen and methane concentrations were greater in the fructose-intolerant than in the fructose-tolerant patients after fructose ingestion (p ≤ 0.02).
Conclusions & Inferences
Fructose intolerance in FGID is not related to post-ingestion plasma concentrations of fructose and its metabolites. Factors other than malabsorption, such as altered gut microbiota or sensory function, may be important mechanisms.

留言 (0)