
記住我




Medical education has vastly changed in the past few decades. The National Medical Council has brought in a competency-based curriculum for undergraduate medical students.[12] The aim is to make the medical graduates more competent and so that they may deliver better health care independently. Numerous efforts have been made in the past, following the United States standards, to have similar results in the post-graduate medical care[3] Indian, nay South Asian residency programs still operate on a gurukul model: the trainee learns from the teacher by observing and learning skills for a period of two to three years.[4] Feedbacks which have been collected earlier previously collected from the residents, about the validity of residency training programs in India have highlighted that there was enormous diversity amongst them.[567] A survey commissioned by the Dr. Rajendra Prasad Centre for Ophthalmic Sciences, All India Institute of Medical Sciences in 2003 had looked at the status of sub-specialty training in ophthalmology.[8] The respondents were the heads of departments/institutions in India.
The All India Ophthalmology Society had commissioned the ‘Residency Evaluation and Adherence Design Study‘ (READS) to gauge what young ophthalmologists, who had spent a few years in practice, felt about the viability of their residency training in their respective careers.[910] It also compared the residency training across the decades, between the last two decades of the 20th century and the first decade of the 21st century.[11] An evaluation of the ophthalmology departments of medical colleges in the past (performed more than a decade ago), had come with recommendations for better quality residency training.[1213] It had led to recommendations from expert groups defining the ideal program, as well as editorials in the Indian Journal of Ophthalmology.[141516]
Ophthalmology residency teachers perform the key role of transmitting knowledge and skills to young residents through didactic teaching, bed side clinics, case presentations, supervision in operating rooms and also oversee their research projects. They have the prime responsibility of ensuring that young residents learn ophthalmology competently.
Except for the study in 2003,[8] the ophthalmology teachers or residency trainers‘ perspectives have never been considered. The aim of this pan-India study was to get a feedback from the ground level enforcers on what an ideal residency program should be, in terms of clinical exposure, surgical skill transfer, academics, and research.
MethodsThe cross-sectional study was conceived and commissioned by the Academic & Research Committee of the All India Ophthalmological Society. The study was in the form of a survey launched during the All India Ophthalmology society‘s annual meeting in February 2019. The basic questionnaire used had been validated in the READS study.[9] Six questions pertaining to non-clinical training were added and a pilot study was done to check the validity. They were questions regarding the teaching of ethics, medico-legal matters, financial skills, law & statutory regulations, communication skills, and stress management. A survey monkey link was shared via email with the study population. After the pilot study, the survey link was edited, so that the respondent would be able to complete it within 15 minutes.
The survey was circulated to the ophthalmologists who were faculty members in a medical college or corporate or municipal hospitals or in non-governmental organizations (NGO), that had a residency program. Only accredited teachers were invited to participate in the study. The senior residents were excluded from the study. The survey was electronic, but printed versions were used for senior teachers who were more comfortable with the print media as compared to the electronic media. Reminders were sent to the potential respondents via WhatsApp and SMS, which were later followed by communication through the telephone. Each potential respondent was reminded on three occasions. Heads of institutes, association of medical college teachers and office bearers of AIOS and various state societies were enlisted to help reach out to respondents.
Ethics approval was sought and obtained from the institutional ethics committee of DY Patil Medical College, Pimpri, Pune.
The respondents were asked to complete demographic data which included the type of institution, the state (province) in which they worked and their professional designation. They were asked to comment on what they thought was the ideal way to impart clinical and surgical skills.
The data were collected and collated in an Excel worksheet and the Statistical Package for Social Sciences (SSPS version 16), IBM, Bangalore, India was used for data analysis. Median, mean and standard deviation of responses were considered.
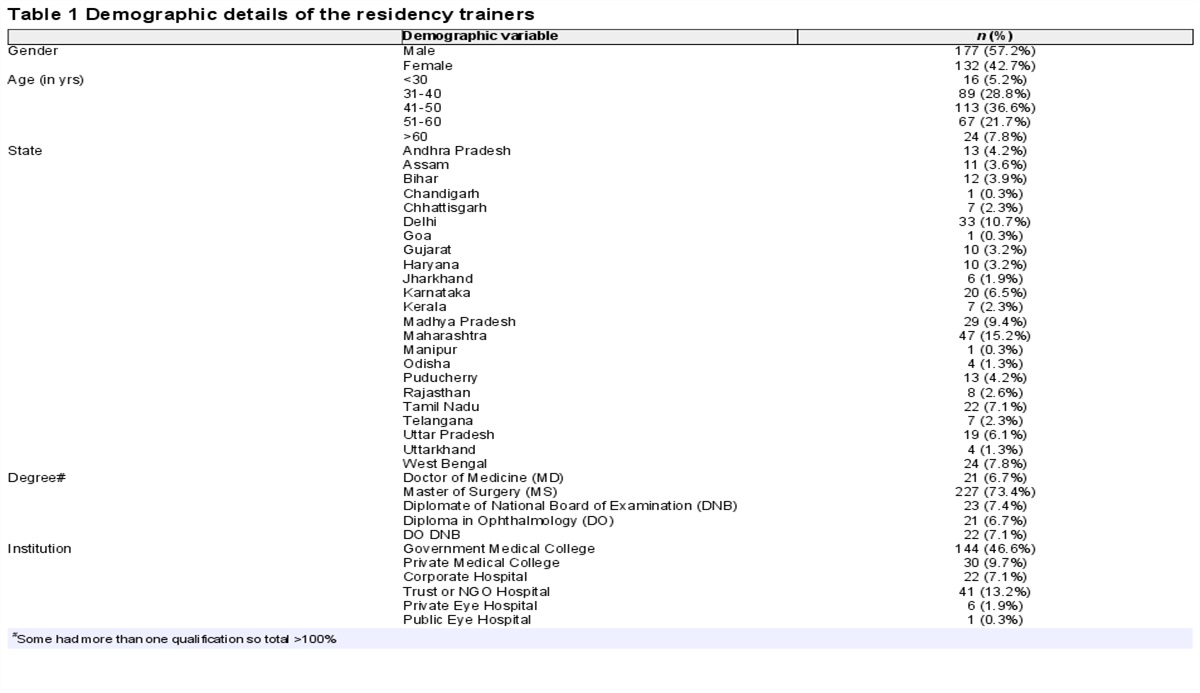
ResultsThree hundred and twenty-five ophthalmology residency trainers, amongst the 682 contacted, responded to the study questionnaire, - a response rate of 47.6%. There were 309 responses which were complete and valid. Among the respondent teachers, 132/309 (42.7%) were females and their age ranged from 26-68 years (Mean 45.3 + 9.5 years). Their demographic details are given in Table 1. Sixteen (5.2%) were ≤30 years of age, 89 (28.8%) aged 31-40 years, 113 (36.6%) aged 41-50 years, 67 (21.7%) aged 51-60 years and 24 (7.8%) were >60 years of age. The respondents were teaching in 23 states of the Indian union. Table 1 also demonstrates the type of institution and the academic degrees of the teachers. Two respondent teachers had an FRCS degree while another two had a Ph. D degree. Some had more than one qualification.
 Table 1:
Table 1: Demographic details of the residency trainers
The residency trainer‘s expectations about how much their wards should be competent in clinical skills in the out-patient department are given in Table 2. If the parent institution did not have all the facilities for investigation and treatment, 277 (89.6%) reported that the residents should be allowed to observe and learn at another medical college, NGO hospital, private practice or institute of excellence to garner the necessary competency; only 3 (1%) were naysayers, while 29 (10%) were ambivalent.
 Table 2:
Table 2: Each resident should be taught/made to learn the following clinical skill in what detail: Rate from 0-10; 0: no exposure at all, 10: ideal/extremely proficient
The number of surgeries a resident should ideally observe, during residency training, for him/her to be adequately exposed to that skill set are reported in Table 3.
 Table 3:
Table 3: Surgeries to be ideally observed by the resident
The number of surgeries each resident should ideally perform independently, during residency training, for him/her to be adequately competent in that skill set, are reported in Table 4.
 Table 4:
Table 4: Surgeries to be performed by the resident: How may surgeries should a resident get to perform during residency training. (please write number of surgeries, in entire 2 or 3 years. Please write 0 if you feel this surgery need not be given independently to a resident)
Table 5 reports the teacher‘s perspective about how much should a resident be taught every month by the following academic modes: lectures, seminars, case presentations, journal clubs and wet labs each month.
 Table 5:
Table 5: The frequency of academic activity in a month
The trainers were asked if their wards needed to be taught some life skills to become more competent professionals. Table 6 shows how the trainers responded about teaching of medical ethics, medico-legal matters, financial skills, law & statutory regulations, communication skills and stress management to their wards.
 Table 6:
Table 6: Should the resident be taught/exposed to the following non-medical skills during the residency?
One hundred and ninety-five (63.1%) respondent teachers opined that even diploma candidates should undergo the research dissertation or thesis. Forty-five (14.6%) were against it, the commonest reason being lack of adequate time to undertake that endeavor, while 69 (22.3%) were ambivalent about it.
The topic for thesis or dissertation was decided by 255 (82.5%) teachers after discussion with their students and taking their wishes into consideration, while 32 (10.4%) reported that they (teachers) or their institution would make the choice, while 22 (7.1%) left it to their students. Ethics committee approval was always sought and obtained by 290/309 (93.9%), 15 (4.9%) sometimes did it, while 4 (1.3%) reported they did not seek ethics approval. On being asked to rate on a scale of 0-10, how well versed with research methodology their students were at the end of the thesis process, the average score was 7.0 (std dev 2.2, range 0-10).
The research work of the dissertation was presented by their student in a conference according to 254/309 (82.2%) of the teachers. According to 26 (8.4%) it was the supervising faculty, while 12 (3.9%) reported both the student and the supervisor presented at some meetings. Four (1.3%) reported their student‘s work had never been presented, 2 (0.6%) reported the presentation was by another faculty; while 11 (3.6%) said it was not applicable, as they had never had a student till now, had their first student or only a diploma student. The presentation format in conferences was oral for 98 (31.7%), poster for 26 (8.4%) and both for 185 (59.9%) dissertations.
The dissertation work of their students had never been published in an indexed journal according to 112 (36.2%) teachers, 66 (21.4%) reported it had been published only once, while 122 (39.5%) reported that it was frequently published.
DiscussionThe results of this study show that the teachers expected their wards/residents to learn clinical skills completely––the median was 10 for all components of comprehensive examination like slit lamp examination, direct & indirect ophthalmoscopy, applanation tonometry, +78/+90D fundus evaluation, keratometry and gonioscopy. Only for orthoptic evaluation, Hess charting, stereo acuity and pediatric visual acuity estimation, the median was 8 or 7. These were all components of pediatric ophthalmology and strabismus whose training was perhaps not enough to meet the needs of India‘s 400 million children.[17] In fact, residents trained in the last century reported better training in strabismus management.[11] Automated perimetry, A and B scan ultrasonography were also marked as 10, which means that they should learn enough to become ideally proficient. Retina related investigations were rated 8 or 9, just below ideal proficiency. This is in line with feedback from residents who reported better training in glaucoma and retina related skills.[111819] Amongst the LASER procedures, the teachers expected their residents to be extremely proficient in posterior capsulotomy, but were willing to settle for less in retinal LASER procedures. This contrasts with what young ophthalmologists had reported.[9] While some reported that they had been taught the skill to proficiency, others had reported no exposure at all.[911] Even some teachers, albeit a small minority, were willing to settle for less than proficiency among their residents.
Unlike clinical skills, there was an enormous variation amongst what the residency trainers thought their wards should observe and perform in the operation theatres to obtain proficiency. Some expectations were unrealistic (observing and performing a few hundred cataract surgeries) given the limited surgical volumes and numerous residents that many training programs have, but most expected their wards to learn cataract, glaucoma, lacrimal sac, pterygium and chalazion surgery (medians > 2). After cataract, pterygium and chalazion the maximum median score was for dealing with ocular emergencies, foreign body removal, scleral and corneal tear repair and managing chemical burns. The trainers rightly believed that residents should be adequately equipped to deal with ocular emergencies.
The trainers seemed to prefer leaving keratoplasty, retinal detachment, strabismus and refractive surgery training for fellowship post-residency, the median was zero for performing independent surgeries. Only vitrectomy, encompassing anterior vitrectomy, was considered essential for an ophthalmology resident‘s armamentarium. But this thinking is not reflected in the actual number of surgeries performed by the residents as per READS study.[911] The enormous variation observed in the READS study for clinical and surgical training may be because the trainers themselves were not in unison what and how much to teach. The residents and their trainers have a limited time for skill transfer and academics, as there are demands of patient care, statutory requirements, dissertation and examinations. The 21st-century patients are more aware of their rights and most training programs, rightly consider patient safety of paramount importance. Wet labs and simulators can help augment surgical training.[202122]
A variation was observed amongst the University department‘s residency programs in the United Kingdom too.[23] Eliciting patients consent for taking up a surgical case for training was a challenge in the UK.[24] In India, a presumed consent is taken from the patient that their surgery may be used for training under supervision. The presence of limited opportunities to learn and master surgery has been reported not just from India, but also from Nigeria and China.[252627] Many developed countries have tried to obviate this by using simulation and wet labs.[202122]
The trainers expected the residents to attend a lecture, seminar, case presentation, journal club and wet lab at least once every week (median 4 for each month). Seminars and case presentations were rated slightly more than journal clubs, this was similar to feedback from young ophthalmologists in the READ Study.[10]
Seeking ethics committee permission for the proposed dissertation was the norm, but it was not universal. Nearly half had their students‘ dissertation published, most had it presented orally or as a poster. Most allowed their students to do the presentation. Publications were less common. On a scale of 0-10, the mean was 7, about whether residents learn research methodology during the dissertation process, similar to what was reported by young ophthalmologists about their training.[10]
Teachers overwhelmingly acknowledged that residents should be taught about ethics, statutory regulations, law, medico legal matters and communication skills. They perceived that teaching only clinical and surgical skills would not make their wards competent professionals. They were ambivalent about financial skills (perhaps because most were in a salaried job) and stress management. But training programs of the future would have to include some, if not all, of these skills to help shape a new generation of ophthalmologists.
There is a significant gap between the expected ideal by the trainers and actual learning that a resident receives as reported in the READ study.[911] A vast majority of teachers expected their wards to become competent professionals. There was near unanimity about the content of clinical skills training, non-medical skills and academics, but there was a significant variation on extent of surgical training that should be imparted to the residents. A lack of unanimity and clarity amongst the teachers may also be a contributing factor to the wide variation observed. Retina, pediatric ophthalmology, cornea and refractive surgery can be later learned in fellowship.
ConclusionOur study has unraveled an existing gap between the expectations by the teachers and residents and the reality in ophthalmology residency training. The challenge is to bridge the gap. A shift to competency-based education, as it had happened in the United States may help.[3] There should be benchmarks, not just for theoretical knowledge imbibed, but also for the hands-on clinical and surgical skills learnt during residency. Statutory norms may be laid down for the basic competency a young ophthalmologist acquires during his/her residency program. The All India Ophthalmology Society and various health Universities can take initiative to this effect.
Financial support and sponsorshipAcademic and Research Committee, All India Ophthalmology Society (2019-20).
Conflicts of interestThere are no conflicts of interest.
AcknowledgementsAcademic & Research Committee, All India Ophthalmology Society (2019-20).
Shrivallabh Sane for the statistical analysis. Optometrists Mahima Bhushanwar and Muskan Shaikh for data collection.
Dr. Ajit Babu Majji, Dr. Arup Chakraborty, Prof. O K Radhakrishnan, Dr. Prashant Bawankule, Prof. Rohit Saxena, Dr. Krishna Prasad, Dr. Amit Porwal, Dr. Satyajit Sinha and Prof. Bageshri Gogate for their inputs. Mrs. Radhika Warty for English language editing.
1. Last accessed on 2020 Mar 29 Available from: www.mohfw.gov.in 2. Last accessed on 2020 Mar 29 Available from: www.mciindia.org 3. Golnik KC, Lee AG, Wilson MC. A national program director survey of the shift to competency-based education in ophthalmology Ophthalmology. 2008;115:1426–30 4. Mendis L, Adkoli BV, Adhikari RK, Muzaherul Haq M, Qureshi AF. Postgraduate medical education in South Asia BMJ. 2004;328:779–81 5. Gogate P, Deshpande M, Dharmadhikari S. Which is the best method to learn ophthalmology? Resident doctors‘ perspective of ophthalmology training Indian J Ophthalmol. 2008;56:409–12 6. Ajay K, Krishnaprasad R. Feedback of final year ophthalmology postgraduates about their residency ophthalmology training in South India Indian J Ophthalmol. 2014;62:814–7 7. Ajay K, Krishnaprasad R, Divya DS. Ophthalmic surgical training in Karnataka and Southern India: Present status and future interests from a survey of final-year residents Indian J Ophthalmol. 2015;63:306–11 8. Murthy GV, Gupta SK, Bachani D, Sanga L, John N, Tewari HK. Status of specialty training in ophthalmology in India Indian J Ophthalmol. 2005;53:135–42 9. Gogate PM, Biswas P, Natarajan S, Ramamurthy D, Bhattacharya D, Golnik K. Residency evaluation and adherence design study: Young ophthalmologists‘ perception of their residency programs I: Clinical & surgical skills Indian J Ophthalmol. 2017;65:452–60 10. Gogate PM, Biswas P, Natarajan S, Nayak BK, Gopal S, Shah Y, et al Residency evaluation and adherence design study: Young ophthalmologists‘ perception of their residency programs II: Academics & Research dissertation Indian J Ophthalmol. 2017;65:8–12 11. Biswas P, Gogate PM, Maskati QB, Natarajan S, Verma L, Bansal P. Residency evaluation & adherence design study III: Ophthalmology residency training in India: Improving with time? Indian J Ophthalmol. 2018;66:785–92 12. Thomas R, Dogra M. An evaluation of medical college departments of ophthalmology in India and change following provision of modern instrumentation and training Indian J Ophthalmol. 2008;56:9–16 13. Grover AK. Postgraduate ophthalmic education in India: Are we on the right track? Indian J Ophthalmol. 2008;56:3–4 14. Honavar SG. Ophthalmology residency training in India: Quo vadis? Indian J Ophthalmol. 2017;65:427–8 15. Gupta A. Ophthalmology postgraduate training in India: Stirring up a hornet‘s nest Indian J Ophthalmol. 2017;65:433–4 16. Grover AK, Honavar SG, Azad R, Verma L. A national curriculum for ophthalmology residency training Indian J Ophthalmol. 2018;66:752–83 17. Gogate P, Biswas P, Vijayalakshmi P. Pediatric ophthalmology training in India Indian J Ophthalmol. 2018;66:478–9 18. Gogate P, Biswas P, George R. Is ophthalmology residency training in India geared to tackle the glaucoma challenge? J Glaucoma. 2018;27:e53–4 19. Gogate P, Biswas P, Das T, Nirmalan P, Natarajan S. Ophthalmology residency training in India: Comparing feedback about how the training equips ophthalmologists to combat retinal diseases. READS report#6 Indian J Ophthalmol. 2019;67:1816–9 20. Ramani S, Pradeep TG, Sundaresh DD. Effect of wet-laboratory training on resident performed manual small-incision cataract surgery Indian J Ophthalmol. 2018;66:793–7 21. Gogate PM. Wet lab for cataract surgery training Indian J Ophthalmol. 2018;66:798 22. Gillan SN, Saleh GM. Ophthalmic surgical simulation: A new era JAMA Ophthalmol. 2013;131:1623–4 23. Alexander P, Matheson D, Baxter J, Tint NL. United Kingdom national cataract training survey J Cataract Refract Surg. 2012;38:533–8 24. Steeples L, Mercieca K, Smyth K. Consent for cataract surgery training: A national trainers‘ survey Eye (Lond). 2012;26:666–70 25. Ayanniyi AA, Taoheed AA. Fulfilling human resources development goal in West Africa: Can the training of ophthalmologist diplomates be improved? West Afr J Med. 2009;28:177–81 26. Eze BI, Nwadinigwe CU, Achor J, Aguwa EN, Mbah A, Ozoemena F. Trainee resident participation in health research in a resource-constrained setting in south-eastern Nigeria: Perspectives, issues and challenges. A cross-sectional survey of three residency training centres BMC Med Educ. 2012;12:40 27. Young AL, Jhanji V, Liang Y, Congdon N, Chow S, Wang F, et al A survey of perceived training differences between ophthalmology residents in Hong Kong and China BMC Med Educ. 2015;15:158
留言 (0)