
記住我




The pediatric age group is from birth to 16 years. The World Health Organization (WHO) divides this period into 5 groups: neonate (0-30 days), infant (1–2 years), young child (2–6 years), child (6–12 years), and adolescent (12–16 years).[1]
Retinal disorders are one of the important causes of childhood visual impairment (VI) and blindness.[23] These can constitute a large proportion of causes of childhood blindness[2] and is prevalent in both high- and low- income countries.[3] Generally, there appear to be age-specific patterns of pediatric retinal diseases with some degree of overlap. Other than possible birth trauma, the common ones in neonates and infants include retinopathy of prematurity (ROP), TORCH (Toxoplasmosis, Other infections, Rubella, Cytomegalovirus, Herpes simplex) infections, congenital anomalies, retinoblastoma, and retinal dystrophies like Leber Congenital amaurosis (LCA), retinoschisis and achromatopsia. The common retinal disorders in children up to 12 years includes other vascular retinopathies, inflammatory disorders, tumors, non-accidental injuries (previously termed battered baby syndrome), accidental trauma, retinal dystrophies and diabetic retinopathy (secondary to type 1 diabetes). Of all the disorders, there has been an exponential rise in ROP in the last decade and continues to be the most common retinal disease in neonates and infants.[2345]
Blindness causes a massive impact on the development of the child and affects the psychological, educational, and socioeconomic growth. These in turn lead to increased disability-adjusted life years (DALY).
Retinal imaging has enhanced our ability to refine understanding of the anatomy, pathophysiology, diagnosis, and management of retinal disorders. From the development of the first ophthalmoscope in 1851, to our current ability to visualize individual retinal cells using adaptive optics, the journey has been remarkable[6] But most times the design of devices using new technologies has been confined to retinal imaging in adults. Neonates and infants have smaller eyes and different anatomy than adults. Most of these devices need good fixation for image capture. Poor fixation in children due to short attention span leads to image with multiple artifacts. In order to adapt to children, these devices have to be much smarter- miniaturized, portable, noninvasive with auto focus and quick image capture. Introduction and availability of handheld devices is a welcome change in the technological advances, but it is not available in all modalities. In this review, we would elaborate on the various modalities, their indications and challenges for imaging used in pediatric retinal disorders, but mostly limited up to 12 years age group since the adult diagnostic devices could be used conveniently in the adolescents (12-16 years).
ChallengesThere are three main challenges in pediatric imaging: parental consent, child‘s cooperation, and shortage of health workforce. Parents must be convinced that the test is essential in management decision; a quick, painless and non- invasive test is likely to have more acceptance. Neonates may not need general anesthesia, as they are small enough to be cozily swaddled. Parents are unlikely to oppose fundus imaging using a hand-held fundus photography system. However, the use of contact systems along with accessories like speculum and indenters might not be acceptable to some parents. A clear, transparent, persuasive conversation and creating a good rapport with the parents is of utmost importance. Children of one year of age and older are invariably anxious in hospital environment. The attention span is less, and hence every attempt must be made to buy their cooperation including use of colorful fixators or playful methods in quiet and non-crowded environment. Many a times, the older children may require general anesthesia.
Currently, hand-held devices to capture retinal images in a child in supine position are available for fundus photography, but not for other useful modalities such as optical coherence tomography (OCT) and OCT angiography (OCTA). Similarly, flash electroretinography (ERG) and visual evoked potential (VEP) are available as hand-held devices, but not pattern ERG and multifocal ERG (mfERG).
The third challenge is the scarcity of trained human workforce: trained technicians to perform these tests deftly and reliably, and pediatric retina specialists who could interpret the results and gainfully use the results in clinical care. Even in the devices like ocular ultrasonography where fixation is not needed, evaluating each quadrant with precision and confidence is challenging in a crying child. A trained and skilled child-friendly technician thus helps.
Despite these constraints, newer technologies have seen multiple advancements in pediatric retinal imaging in the last decade. The summary of usefulness of these modalities in pediatric retinal diseases is summarized in Table 1. We describe individual diagnostic methods with special mention of their technique and utility in pediatric retinal diseases.
 Table 1:
Table 1: Retinal diagnostic tests in pediatric disorders
UltrasonographyThe first report of ophthalmic ultrasonography (USG) was published in 1957.[7] It is a useful and time-tested modality for imaging the posterior segment. It is inexpensive and noninvasive, and does not require use of sedation or anesthesia. Most of the equipment used in adults is also suitable for use in children. Depending on the indication and characteristics of sound waves, most commonly used ultrasonographic examinations include the following:
A-scan biometry for axial length measurements Diagnostic B-Scan USG along with corresponding A scan ultrasonography Ultrasound biomicroscopy for anterior segment.Technique. A coupling medium is needed for good ultrasound waves transmission from the transducer to the globe.[8] Transducer probes of frequency from 10-30 MHz are used for ophthalmic ultrasound. Coupling gel (propylene glycol) is applied over the eyelids and the scans are performed over the eyelid. Immersion A-scan is performed with open eyelids taking care to avoid excessive pressure on the cornea. Systematic protocol-based approach in scanning the entire globe helps avoid missing small lesions. The accepted sequence is axial scan, followed by transverse scans from superior to inferior and sagittal views, and lateral to medial scans. Adjusting the gain can help in identifying minimal inflammatory debris or membranes in the vitreous cavity.[9]
Indications. Ultrasonography is commonly used in situations where detailed examination of retina is not possible. It may be due to media opacities including but not limited to corneal edema, corneal scars, poorly dilating pupil, cataract, retrolenticular membranes, or vitreous hemorrhage and haze. A-scan biometry is indicated in pediatric retinal diseases such as nanophthalmos and posterior microphthalmos. A routine USG examination could be easier than repeated dilated eye indirect ophthalmoscopy in children with high risk of retinal detachments such as in eyes with uveal colobomas, microphthalmia, high myopia, closed globe injuries, genetic syndromes predisposing to retinal detachment, and in mentally challenged children with vision loss.[10] Two distinct advantages of USG are examination without dilatation and avoidance of annoying light of an indirect ophthalmoscope in an often crying and apprehensive child. USG is useful in detection and monitoring treatment outcome of intraocular tumors [Fig. 1].[11] Table 2 summarizes the indications of USG in pediatric retinal disorders.
 Figure 1:
Figure 1: A 2- year old female, born preterm at 32 weeks, presented with bilateral leucocoria. She was referred with a diagnosis of Stage V retinopathy of prematurity. (a) An immersion ultrasonography of left eye shows a mass lesion in the posterior half of the globe. (b-d) Transverse scans of superior, nasal and temporal half showing a mass lesion with intraretinal calcification. She was diagnosed with retinoblastoma and was treated for the same
 Table 2:
Table 2: Indications of ultrasonography in pediatric retinal diseases
USG provides a comprehensive overview of the anatomy of the globe with reproducible images. But the details of ocular pathology might not be clear on USG. Extension of any lesion into the orbit requires deeper penetration of the ultrasound waves. USG images are inferior to computed tomography (CT) or magnetic resonance imaging (MRI) scan.[11] Nevertheless, USG remains an important adjunctive tool in imaging the eye in children.
Ultrasound biomicroscopy (UBM) was developed in 1989.[12] It uses high frequency transducers, ranging from 50-100 MHz which provide better resolution, about 40 μ, of the cornea, lens, aqueous and ciliary body.[121314] UBM cannot image structures deeper than 4 mm from the surface.[8] It requires the use of a coupling medium like saline or methylcellulose, which is held over the eye in a custom made cup while the transducer is dipped in it. UBM is widely used to image the ciliary area in uveitis, ciliary tumors and trauma. UBM is reported to have a good sensitivity and reproducibility to detect retinoblastoma extension into anterior retina and ciliary body.[15] Other specific uses of UBM are documenting changes in the ciliary body in intermediate uveitis,[16] and anterior hyaloidal fibrovascular proliferation in ROP.[17] The disadvantage is that UBM has to be done under general anesthesia for most pediatric patients unlike the USG.
Fundus Photography (FP)Fundus photography is one of the most common retinal imaging performed in children. These could be either contact or non-contact camera.
Contact retinal camerasRetCam ™ (Clarity Medical System, Pleasanton, CA, USA) remained the most widely used wide-field pediatric contact fundus camera for longer than two decades. It features capabilities of wide-angle fundus view (1300), anterior segment, angle and posterior segment imaging with fives different detachable lenses (D1300, B1200, E800, C300, portrait lens). This foot-pedal operated system needs topical anesthesia, wire speculum (separates the eyelids) and ultrasound gel or 2% hydroxypropyl methylcellulose (HPMC) for coupling between the cornea and the probe. Careful scleral indentation helps capture the retinal pathology in extreme periphery. A montage image provides a panoramic view. RetCam shuttle is a portable system and has been widely used in screening for ROP, both in universal newborn eye screening[18] and tele-screening.[192021] It is also one of the common devices used to document and follow up cases of intraocular tumors in children, including retinoblastoma. The handheld probe has an advantage in imaging children under general anesthesia or in neonates. But the RetCam probe is heavy and unwieldy; artifacts are not uncommon. This system is also expensive for every one to procure. Icon (Phoenix Clinical) is a modified version of the contact based fundus camera with interchangeable and light weight LED based handpiece. It provides a 100 degree field of view and comes with an inbuilt FFA module.
Some of shortcomings of RetCam have been overcome by a compact and portable system developed in India (3Nethra Neo ™, Forus Health, Bangalore, India).[22] This comprises of a handheld camera with inbuilt liquid lens system, and LED based illumination system. It provides a maximum of 120 degree field of view. The other novel featurs include option of adjustment for colour and contrast.[23] This is very useful in enhancing subtle vascular changes. This system presently cannot be used image the anterior segment or angle due to the inbuilt lens system. A technical and fundus image comparison between Retcam and 3Nethra Neo is shown in Table 3 and Fig. 2 respectively.[22] Other cameras introduced in the recent times are PanoCam LT (Visunex Medical Systems) which has the advantage of being a wireless system. It offers a 130 degree field of view.
 Table 3:
Table 3: Technical comparison between Retcam and 3Nethra Neo
 Figure 2:
Figure 2: Wide field fundus photograph of right eye of a preterm neonate showing active neovascularization in zone 1. (a) Picture taken on Retcam with about 130 degrees of field, superior and inferior edges appear cropped. (b) Picture of the same eye taken on “Neo” with about 120 degrees of field in a circular capture
Non contact retinal cameras Smart phone photographyNewer generation smartphones are equipped with a high-quality optical system and a coaxial light source, which can be used to capture high-quality retinal images. The camera‘s coaxial flashlight and a handheld high plus power lens create an indirect ophthalmoscopy-like optical system that is able to record high- resolution digital retinal images. The emitted light of smartphones is safe as retinal irradiance from smartphones is less than that from an indirect ophthalmoscope.[2425] The field of view varies with the dioptre strength of the handheld lens (46°, 53°, and 90° with +20D, +28D, and +40D indirect condensing lenses respectively).[26] The acquired image is inverted, like an indirect ophthalmoscope view. For a single examiner, MIIRetCam or a condensing lens/smartphone/MIIRetCam/black tube device assembly can be used to capture images.[27]
Apparently, there was no significant difference between the images taken by smartphones and fundus cameras in adults.[28] The autofocus capability of smartphone camera helps maintain the image quality. The quick data transfer capability in smartphones can be utilized as an effective telemedicine tool to share and discuss the cases in remote places, e.g., screening for pediatric eye diseases such as ROP and diabetic retinopathy in children and adolescents.[29] Hazy vitreous, small pupil and vasculosa lentis could hamper good quality image acquisition.[26] There is a learning curve in using the smartphone camera to capture the images since it is based on inverted virtual images.
Wide field and Ultra-wide wide field fundus photography (UWF-FP)Optos ™ Panoramic 200Tx imaging system (Optos PLC, Dunfermline, Scotland, UK) is a popular UWF fundus camera based on scanning ophthalmoscope technology and utilizes an ellipsoid mirror to capture a retinal image spanning a maximum of 200 internal degrees. Green and red lasers produce pseudo color, but high-quality retinal images.[3031] The coverage in a single image is much greater than in any other existing retinal cameras. This makes it a lucrative choice for pediatric vascular disorders like ROP, familial exudative vitreoretinopathy (FEVR) and Coat‘s disease, the pathology of which often lies in the peripheral fundus [Fig. 3]. It‘s use in imaging in ROP was reported in 2013.[31] The authors demonstrated the modified ‘flying baby position‘ with one arm supporting the chest/chin and the other hand supporting the head to acquire ultra-wide field images.
 Figure 3:
Figure 3: (a) Ultra-wide field fundus photograph of a 28 weeks GA neonate with APROP (b) Follow up image of the same eye 2 weeks post intravitreal avastin showing regression of plus disease. (c) Ultra-wide field fundus photograph of a 4 year old boy with submacular exudates and peripheral telangiectasia in nasal quadrant, He was diagnosed as Coat‘s retinopathy and focal laser was done to the telangiectatic vessels. Inferior view of the fundus is limited due to artefacts due to eye lashes. (d) Follow up image of the same eye showing regressed macular exudates and telangiectatic vessels post focal laser
Ultra-wide field acquisition of images in one go with a laser based camera makes it comfortable for relatively older children in age group of 3-8 years, who are otherwise uncooperative for fundus examinations. This could potentially decrease the need for examination under anesthesia. With inbuilt fundus fluorescein angiography (FFA) and autofluorescence modules, there are possibilities of use in a wide range of indications including retinal dystrophies, peripheral vascular diseases, retinal detachment, myopia, tumors, inflammatory disorders etc.[3233] It is also useful in training.[34]
The Optos image is not adversely affected by localized media opacities like limited vitreous hemorrhage, cataract and small pupil.[30] Some of the disadvantages of the current system include a larger horizontal than vertical meridian field, pseudo-color (makes interpretation of of ocular tumors difficult), and presence of eye lashes in the field of view (further limits the vertical coverage) [Fig. 3c]. Image capture is marginally difficult in slightly older infants. Additionally, the system is not portable and is expensive.
The Heidelberg Spectralis ultra-widefield imaging module (Heidelberg Engineering) is also one of the non-contact-based camera which uses an attachment to acuire high-contrast images till 102 degrees of field of view. This attachment can be rotated 90 degrees to acquire images in supine position. The additional features of FFA and OCT makes it an important addition in the imaging armametarium.
Telemedicine is an important application of fundus photography for pediatric retinal diseases. Its utility in ROP screening and referral has been reported worldwide[19202122] including India. The “KIDROP” program in India has completed over 150,000 sessions (at the time of this publication) in over 127 neonatal units.[353637] Software based image-enhancing tools, machine learning and auto detection of disease have been integrated into tele-screening programs.[38394041] Newer tools using artificial intelligence (AI) are also being evaluated and hold promise.[42] Tele-ROP has been reported in universal newborn eye screening in India[43] and is already included in India‘s national ROP guidelines.[44]
AutofluorescenceFundus autofluorescence is due to accumulation of fluorescent material, like lipofuscin, in retinal pigment epithelial cells. This property can be captured using longer wavelength light wave or shorter wavelength in blue and green spectrum for better appreciation of fundus changes. Recent modification in capturing images including ultra-wide field, confocal scanning laser ophthalmoscopy, gaze tracking and faster acquisition of images with higher resolution without pupil dilation has helped in overcoming limitations like artifacts, poor fixation and eyes with nystagmus.
Blue FAF (HRA ™, Heidelberg, Germany), uses confocal laser scanning ophthalmoscope (CSLO) based technology instead of normal light wave, with blue filter which allows 488 nm wavelength, more sensitive to lipofuscin compared to infrared wavelength spectrum which gets reflected from melanin pigments.[45] Normal FAF not only represents the anatomic integrity of the RPE but also the normal photoreceptor, outer segment turnover, and vitamin A metabolism.[45]
Indications: Autofluorescence plays an important adjunctive role in pediatric retinal diseases, particularly the ones involving the RPE and photoreceptors.[46] FAF is used in diagnosis and to monitor progression of common dystrophies in children including juvenile retinoschisis, cone dystrophy, retinitis pigmentosa (RP), LCA and primary macular dystrophies like Best disease, Stargardt‘s disease and others [Fig. 4a and b].[474849505152]
 Figure 4:
Figure 4: A 14- year old female presented with bilateral gradual decrease in vision. The best corrected visual acuity was 20/200. (a) Color fundus image shows a central area of RPE atrophic changes with fleck like changes around fovea. (b) Autofluorescence shows central dark hypofluorescence corresponding to the area of RPE atrophy and multiple hyper- and hypo-fluorescent fleck like deposits around fovea, more prominent than the color fundus photo. She was diagnosed with Stargardt‘s disease
Advantages: It is superior to fundus photography, OCT and OCTA in delineating the extent of RPE damage and atrophy.[53] FAF helps visualize disease specific patterns of lipofuscin distribution which are used as a clue to diagnosis, and are often not visible or difficult to visualize on ophthalmoscopy.
Fundus Fluorescein AngiographyFundus Fluorescein Angiography (FFA) to assess the retinal circulation in human eyes was first published in 1961.[54] Since then it has served as a useful tool to assess vascular status, the disease process, and management of retinal vascular disorders. It is a relatively simple but invasive procedure with a high margin of safety in both adults and children.[55] All the same, it is a good practice to review history of allergy, explain the common side effects like yellow discoloration of the urine and skin at the time of taking the consent.
Technique: Retcam3 ™ (Natus, USA) is a commonly used wide- angle pediatric retinal imaging system, which allows FFA with a 130 degrees view handheld camera. Some key steps include insertion of the yellow filter in the camera hand piece, switching the light source to blue light, and switching the software to FFA mode. A patent intravenous cannula is preplaced by the pediatrician and tested (as dye extravasation can be very painful). Sodium fluorescein 20% is injected intravenously as a bolus dose of 0.04 mL/kg (8 mg/kg) rapidly followed by a saline flush; a close monitoring by a pediatrician/anesthetist helps. Images are captured soon after the dye is injected. One must avoid pressing the globe with the weight of the camera hand piece as the dye might not properly enter the eye. It is necessary to alternate the camera between the eyes so as to capture all phases of dye transit in either eye quick enough before the dye leaks into the anterior chamber.
The Optos, that provides 2000 field of view has in-built support for performing FFA and indocyanine green angiography (ICGA). It is difficult to use this system in smaller babies, but is excellent in older children who can sit upright. Alternatively, the modified Heidelberg Spectralis ultra-widefield imaging module (Heidelberg Engineering) has been successfully used in to capture good quality widefield FFA images under general anesthesia in infants. This system is non-contact and hence compression artefacts are absent.[56]
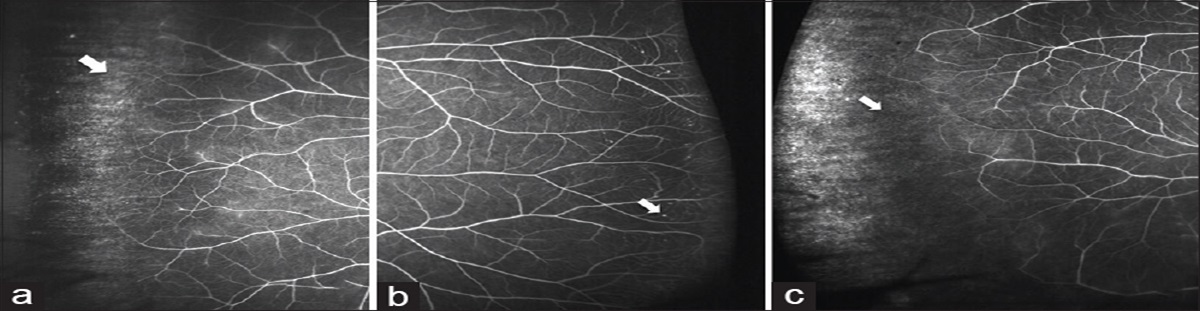
Indications: FFA has been studied extensively in ROP.[575859] It helps clearly demarcate the vascular from avascular retina, identify flat neovascularization not easily discernible to the naked eye, and monitors treatment response [Fig. 5a and b].[60616263] FFA is also useful in other pediatric retinal diseases like retinopathy in type 1 diabetes, FEVR, incontinentia pigmenti, dyskeratosis congenital, muscular dystrophy etc., which have a common presentation of peripheral retinal avascularity, progressive neovascularization and early development of tractional retinal detachment. It has helped identify lesser-known clinical and angiographic findings, where these novel findings have led to an updated FEVR classification and more complete characterization of early stages of FEVR.[64] FFA in these cases also led to the description of newer entities like ROPER which has implications in the management.[65] In Coat‘s disease FFA documents occurrence/progression of characteristic early telangiectasia, capillary non perfusion areas and leakage leading to subretinal exudation – all of which are difficult to detect and assess on indirect ophthalmoscopy.[66] FFA could also be useful to identify subtle retinal new vessels in eyes that present with recurrent vitreous hemorrhage or persistent/progressive vitreoretinal traction, and monitor regression of these new vessels after laser treatment [Fig. 5c].
 Figure 5:
Figure 5: Half zone APROP. (a) Left eye color fundus image shows limited details of vascular retina. (b) Fundus fluorescein angiography (FFA) in the same patient shows vascular retina extent and neovascularization status, not clearly apparent on fundus examination. (c) Wide field FFA shows peripheral avascular retina and neovascular leakage in right eye of 8- year old child presenting with recurrent vitreous hemorrhage
Wide- field ICGA has been performed in preterm babies with active type I ROP and was well tolerated. Choroidal circulation in ROP with peripheral attenuation that corresponds to the regions of avascularity. ICGA has theoretical advantages over FFA like superior imaging in the presence of vitreous hemorrhage. Currently there is limited literature on ICGA in pediatric retinal diseases, but with advances in choroidal imaging, its indications and advantages are likely to expand.
Optical Coherence Tomography (OCT)Despite the ubiquitous use of spectral domain optical coherence tomography (SD OCT) in adult retinal disease management, its adoption into pediatric retina has been limited due to many factors including lack of available instrumentation to easily, rapidly and accurately image infants in the office without anesthesia. Historically, infant SDOCT was performed in the operating room with the baby in the ‘flying baby‘ position under anesthesia and converting the table-top device into a hand-held device.[67] With the introduction of the hand-held OCT device, this tool has become more popular in imaging infants in the office and in the operating room.[68697071] Image optimization is required while imaging pediatric eyes due to a rapidly increasing axial length in the neonatal period,[7273] an evolving refractive status, a steeper cornea and a greater astigmatism in the first six months.[74] Faster OCT systems such as spectral domain (SD) and swept source (SS) (over time-domain system) have shorter acquisition times, and are superior for small children. Adult OCT systems can be easily used for older children who can fixate on the target.
Compared to an adult, the infant‘s fovea differs in that, there is a shallower foveal depression, persistence of the inner retinal layers including the inner plexiform and inner nuclear layers, more attenuated retinal layers, attenuation of photoreceptor layer (PRL) and absence of the PRL sub-layers. Most of this thinning occurs by inner retinal cell migration centrifugally and occurs between 31 and 42 weeks of post menstrual age (PMA).[757677] The photoreceptor layer in infants is initially thin and as the infant grows, there is a progressive centripetal growth of the photoreceptor subcellular structures that extend into the foveal center. There has been good histopathological correlation of the retinal layers with those imaged on SDOCT in developing eyes.[787980]
SD OCT is not a mainstream imaging tool for ROP screening or management yet. However, it can detect clinically unseen or poorly detected retinal features. Vinekar et al. first described macular edema of prematurity (MEOP) as “foveal disruptive” changes on the SD OCT in clinically normal looking foveae in Asian Indian infants,[8182] The MEOP is transient, but may influence the visual acuity and refractive status of infants even at the end of infancy.[82] It helps to prognosticate clinical stage 4A ROP with OCT involvement of the macula.[83] Clinically undetected structures including vitreoretinal interface and epiretinal membranes,[84] retinoschisis,[85] retinal detachment and retinal pigment epithelium changes have reported using OCT.[84] The ability of the OCT to detect neo-vascularization in the posterior retina associated with aggressive posterior ROP (APROP) has helped in OCT guided photoablation of neovascular fronds.[68] It has also been utilized for assessment the macula status after vitrectomy for ROP-related retinal detachments. The vascular abnormality score by OCT (VASO) described by Maldonado et al. delineated the severity of vascular pathology in ROP and is useful in early detection of disease progression and in monitoring the response to therapy.[86]
OCT is an important tool in finer evaluation of the retinal layers in inherited retinal dystrophies, inflammation and infections. Macular edema, epiretinal membranes and extent of photoreceptor loss associated with retinal dystrophies are best reviewed using OCT. It serves to be an important part of workup of children presenting with early onset nystagmus (examined under general anesthesia) and/or unexplained visual loss.[87] OCT along with multifocal ERG is an important tool to identify drug toxicities (eg. hydroxychloroquine) affecting the macula. It has been used in evaluation of optic disc drusen. Choroidal thickness and choroidal vascularity has been studied in retinal dystrophies using OCT.[88] Despite these advantages in pediatric retinal diseases and availability of hand held OCT, its widespread use is still limited in clinical practice.
OCT AngiographyOptical coherence tomography angiography (OCTA) is new non-invasive technique to assess retinal vasculature. The available systems can create automated cross sections of retina at superficial capillary plexus (SCP), deep capillary plexus (DCP), outer retina and choriocapillaris (CC).
Conventional dye-based angiography preclude the detection of deeper extensions of neovascularization which are either not seen or leak. OCTA allows us to evaluate the deep capillary plexus despite overlying lesions. This was first reported in an infant with APROP that documented a deeper extension of flat new vessel suggesting that it was a ‘complex‘ of vascular abnormalities.[89] In addition to foveal avascular zone (FAZ), the OCTA also images the SCP- and DCP- vessel density. Some of these reported changes include an increased vascular density in the SCP and DCP in the central foveae of preterm babies[90]; persistent foveal vasculature in the central FAZ in adults who were born premature,[91] and significantly lower vascular density in the para-central regions in a ROP treated cohort.[92] On OCTA, foveal area is apparently reduced in both treated and spontaneously regressed ROP, but the foveal diameter may not be altered.[93]
OCTA allows separate analysis of these capillary plexuses and choriocapillaris as compared to FFA where such detailed layer-wise image separation is not possible. This is especially useful in assessing the choroidal neovascularization. Choroidal neovascular membrane (CNVM) in pediatric population present in association with retinal dystrophies like Best disease, inflammatory disorders like presumed ocular histoplasmosis syndrome, serpinginous choroiditis, myopia or post trauma choroidal rupture.[94] OCTA is reportedly superior to FFA in identification of these CNVMs.[95] Choriocapillaries rarefaction has been studied using OCTA in retinal dystrophies and are of value especially when RPE transplantation is around the corner.[53]
Improper segmentation and multiple artefacts can limit the use of OCTA in children. Hand-held OCTA devices (when commercially available) will hold exciting prospects in our understanding of multiple pediatric retinal disorders.
Visual ElectrophysiologyChildren often can‘t verbalize their symptoms accurately and a detailed retinal examination at times could be challenging. Objective methods of assessment of retinal and visual pathway like visual electrodiagnostics are useful in such situations. The commonly used visual electrodiagnostic tests, and the target cells are briefed in Table 4. Retinal cells and their electrophysiological responses mature variably in infants with time. These must be interpreted with great caution or repeated when required. The major responses, individual component and their origin and maturation with age have been summarized in Table 5.
 Table 4:
Table 4: Commonly used electrophysiological tests and the cells targeted by them
 Table 5:
Table 5: Commonly used electrodiagnostic tests, waveforms, their origin and their maturation with age
Technique: Children older than 4-5 years can easily be tested like adults. Examination of the younger children is more difficult with corneal contact lens electrodes. At any age, the patient acceptance is good with skin electrodes though the wave amplitudes tend to be lower with increased noise. The sensitivity of retinal cells differs between adult and infants. Therefore, the stimulus strength must be adjusted accordingly. The ERG and VEP can easily and quickly be done under sedation or general anesthesia but the pharmacological agents used in the testing could expose the child to risks and alter the response. A survey conducted by International society for clinical electrophysiology of vision (ISCEV) report that most of the responders prefer to perform ERG in an awake stage.[96] Older children can be easily tested with skin electrodes in awake stage. Toys and attractive targets can be used to attract the attention of smaller children to the testing target. The procedure can be briefed and divided into smaller segments to account for the shorter attention span in infants and younger children.
Good recording requires time, commitment and a baby friendly skilled technician. Multifocal ERG (mfERG) can be recorded in infants as small as 10 months old with smaller number of hexagons with a large central hexagon to address reduced pediatric attention span and a better fixation.[97] Electro oculogram (EOG) requires more co-operation than full field ERG. The reflex eye movement with the subject lying supine on mother‘s lap in a chair rocking within a constant angle have been used to perform EOG in infants.[98] Visually evoked potential play an important role in in the objective assessment and localization of the pathology along retinostriate pathway. This becomes important to reason out the cause of visual loss in subjects with a normal fundus but no or subnormal vision secondary to birth related brain injury. Similarly the pattern sizes used to evoke a response in pattern VEP can give a rough idea on the visual acuity and prognosis in infants and preverbal children.
Indications and interpretation: These tests can help in making or confirming the diagnosis, disease classification, localization, assessment of a response to treatment and prognosis, especially in retinal dystrophies [Fig. 6a-f].
 Figure 6:
Figure 6: A 6- year old girl presented with reduction in vision in both eyes; best corrected vision was 20/60 in both eyes. She was able to read 20 of 23 plates in Isihara color vision chart. (a and b) The fundus was unremarkable; (c and d) very subtle photo receptor irregularity on OCT. (e and f) A full field electroretinogram showed normal scotopic and photopic responses while mfERG showed hypovoltaged subnormal responses from central macula. This confirmed the diagnosis of occult macular dystrophy
The results of visual electrodiagnostic tests should be interpreted with caution because of difficulties in doing a test, possible bias secondary to technical adjustments, age dependent change in wave responses in a growing infant and lack of adequate normative data. For example the cone density varies from 15,000 cones/mm2 at the fovea to 12,500 cones/mm2 at 10° in the infant retina compared to ~ 200,000 cones/mm2 at the fovea and 11,300 cones/mm2 at 10° in the adult retina.[99] Smaller and slower responses in mfERG from the central retina are normal for the infants compared to the adults.[99] A subnormal VEP can be due to macular, panretinal, and optic nerve pathology alone or in any combination. It should always be analyzed in conjunction with pattern or full field ERG.
Advantages and disadvantages: Independent, handheld portable systems work best for infants as they can fit in any position and at various places for testing in awake stage. The table- top electrodiagnosis devices are rather cumbersome for use in infants and small children and would require general anesthesia in operating room. The disadvantages with hand held devices include unavailability of pattern ERG and mfERG for macular functions.
ConclusionAdvances in retinal imaging have permitted ophthalmologists to better diagnose and monitor pediatric patients. Non- invasive modalities with high-resolution has helped identify previously unrecognized details. Each imaging modality adds value in its unique way. The collective use of these modalities opens up exciting prospects in pediatric retinal diseases. There is a further need of portable, less expensive and child-friendly retinal imaging devices, so also skilled workforce for testing and interpretation.
Financial support and sponsorshipSupport provided by Hyderabad Eye Research Foundation (HERF), Hyderabad, India. The funders had no role in the preparation, review or approval of the manuscript.
Conflicts of interestThere are no conflicts of interest.
Financial DisclosuresNone of the authors have any commercial interests related to materials or techniques described in this study to disclose.
Author‘s ContributionAll persons designated as authors qualify for authorship, and all those who qualify are listed. Each author has participated sufficiently in the work to take public responsibility for appropriate portions of the content.
1. Position Paper- WHO archives- World Health Organization.Last accessed 2020 Jun 03 Available from: www.archives.who.int 2. Wadhwani M, Vashist P, Singh SS, Gupta V, Gupta N, Saxena R. Prevalence and causes of childhood blindness in India: A systematic review Indian J Ophthalmol. 2020;68:311–5 3. Gilbert C, Foster A. Childhood blindness in the context of VISION 2020--The right to sight Bull World Health Organ. 2001;79:227–32 4. Agarwal K, Balakrishnan D, Rani PK, Jalali S. Changing patterns of early childhood blinding conditions presenting to a tertiary eye center: The epidemic of retinopathy of prematurity in India Indian J Ophthalmol. 2019;67:816–8 5. Solebo AL, Teoh L, Rahi J. Epidemiology of blindness in children Arch Dis Child. 2017;102:853–7 Erratum in: Arch Dis Child 2017;102:995
留言 (0)