
記住我
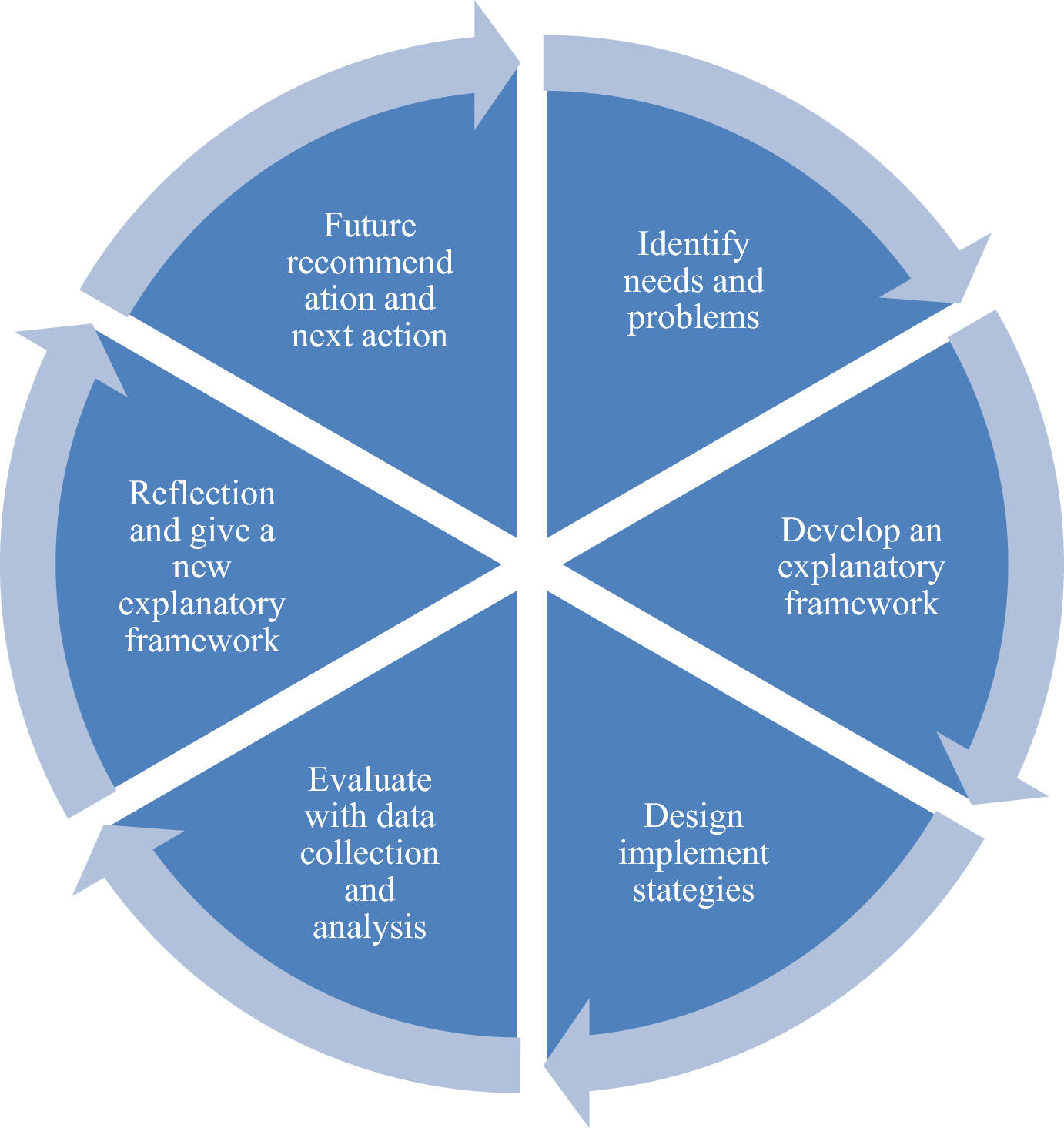








It was clear that further culturally based ethical decisions needed to be made in order to provide ethical, safe and cultural focused care to Juan. This article identifies and evaluates the EEDM process by working through the case using the embodied ethical steps as outlined by Hervey (2007). Along with the movement recommendations from Hervey (2007), I also explored my own movement experiences as I embodied each step in response to my ethical dilemma during the process of writing this article.
Step One: Become FamiliarGiven how violently ethical conflicts can be experienced in the body, (Hervey, 2007), clinicians are drawn away from their embodied experience and shift towards more cognitive approaches to solve ethical dilemmas. Instead of allowing this mind/body disconnect to happen, dance/movement therapists are able to embrace the body using EEDM steps. Hervey (2007) reminds readers that true ethics started as a body-based experience of wrong and right, and in order to find appropriate solutions for ethical dilemmas, one must return to the body for guidance. Embodiment permits us to move past the rational thinking brain (prefrontal cortex) and enter the body. This allows us to develop ethical sensitivity and recognize that there is an ethical dilemma in existence (Hervey, 2007). Step one involves attending to our body’s experience (Csrodas, 1993) by being present and engaged with its perceptual experience. This takes place in the form of movement.
Analytic and somatic movements are two avenues to consider when analyzing bodily movements (Moore, 2014). Moore (2014) introduces analytics as the observation of body movement from an external perspective and somatics as the first-person perspective of internal movement. Csordas (1993) adds that the somatic dimension of movement not only includes attending to one’s internal bodily experiences but also involves attending to the bodies of others, called the somatic modes of attention. Humans are gifted with the ability to interpersonally connect in a way that allows us to feel what others feel when we exercise our use of mirror neurons. Analytic and somatic movement shifts from one’s self and their environment provide evidence that deepens the collection of information and tell us when we have an ethical dilemma on our hands. Again, in this first step of EEDM, it is suggested to postpone any type of action, only to recognize the existence of an ethical dilemma in order to prevent premature and inappropriate action (Hervey, 2007). Instead, Hervey (2007) positions that “vertical containment” of just attending to the body signals and exploring movement in the horizontal plane is ideal for the initial development of an ethical dilemma.
Embodiment of Step OneIn the initial stage of the ethical dilemma presented in this article, my movements became accelerated in the sagittal plane, specifically in my upper limbs, torso, and core. There was a sense of urgency I felt to confide in someone about Juan’s release of private information regarding the spirit attached to his shoulder. I was fascinated by my in-session encounter and wrote in my journals about feelings of excitement and tingling surges running through my body. I also recorded my impression of shaky sensations in my arms, knots in my throat and core, and decreasing pressure in my lower body. Tortora (2006) explains that weight assumes the physical intention of executing an action; the decreasing pressure I experienced in my legs indicated how careful I was to move forward in the dilemma. The vibratory action in my arms implied feelings of anxiousness, and the knots in my throat and core signified some sort of blockage. In my journal I reported feeling a sense of imprisonment; my body felt the restraint of navigating such a cultural dilemma in a hospital setting embedded with Eurocentric forms of healthcare. Though I was excited to learn more about Juan’s experience with the spirit, my movement observations for my core, arms, and legs suggested and confirmed a hesitancy to approach and navigate the disclosure about the spirit. I was motivated and empowered to advocate for him, but I also felt sad and angered by my thoughts of foreseeable outcomes that would be adverse to our therapeutic relationship. Given the cultural context of the dilemma and its tendency to be overlooked in westernized hospital settings, my thoughts held weight. I avoided making any decisions to address Juan’s case, except to obtain support in supervision.
Step Two: Define the DilemmaAfter identifying that an ethical dilemma exists, we are encouraged to define the dilemma and identify potential problem solving opportunities. For this case, the ethical dilemma was respect for culturally based meanings in treatment and how mental health clinicians identify pathology. Juan believed his seeing the spirit was a gift given to him by God; he refused to accept any diagnosis that labeled it otherwise. What Juan described as a spiritual experience is usually understood as a form of psychosis in hospital systems that rely on symptom identification and diagnosis for the treatment of symptoms. Despite encouragement from me, he opposed the idea of talking to his psychiatric nurse about his spiritual experience. I felt stalled between my own spiritual and cultural awareness, Juan’s spirituality, his safety, and having to uphold the policies and procedures of the hospital where I was interning. I understood Juan’s story as a spiritual person, as a clinician, and as a Black woman from the inner city of Chicago; but I wondered if I resonated with his story all too well because we shared the people of color in the American healthcare system narrative. I wanted to make sure he felt heard and included in his treatment. On the other hand, I wanted to avoid compromising his safety in an effort to advocate for him and for increasing cultural awareness at my site. This case with Juan was a culturally embedded ethical dilemma that required my full participation with the embodied ethical steps.
Embodiment of Step TwoMy body and my mind felt uneasy about making a decision; there was a fight between my cultural background and my emergence as a clinician. The idea of both weighed heavy on my shoulders and drained my energy. My upper torso gradually sank downward along the vertical dimension and my entire body wanted to enclose itself and curl like a ball. I encountered feelings of isolation as one of few Black clinicians at my internship site as well as in the academic program at my college. I felt lonely in my ethical dilemma. There are very few articles that talk about a Black clinician’s experience of loneliness during a culturally situated ethical dilemma. Smith (2012), communicated in her thesis about a similar struggle she felt during an ethical dilemma when battling between holding on to her cultural identity as an African American woman versus choosing an identity as a clinician and abiding by ethical codes. I thought with frustration: Why does there have to be a choice? Why cannot my cultural background and my developing identity as a clinician co-exist? Hervey (2007) acknowledged the need to cope with one’s bodily felt experiences when managing complex cases. She concluded that dance/movement therapist found value in moving out the dilemma with full embodiment to support determining the next direction to take. In my attempt to release my body from the enclosed ball and fully embody the dilemma, I encountered hesitation and emotional discomfort. I felt my anger and frustration expand with my movement in the form of increased pressure and restricted affect. My body was reluctant to engage in an emotionally overwhelming, cultural dilemma, but there was a sense of freedom in knowing that I was not giving up.
Step two further required the embodiment of my patient as well as my supervisors and the treatment team to provide an empathic approach to decision-making and deciding the best course of action. In her workshops, Hervey (2007) noted that in this step participants commonly collaborated with one another using creative movement to unlock alternatives to ethical dilemmas. I recall deliberating about the advice of my supervisors, unsure if they realized the substance of my patient’s fear and request for confidentiality given that they did not identify as people of color. For them, it appeared simple: make sure he’s not homicidal or suicidal and inform the nurse practitioner. Juan denied suicidal (SI) and homicidal ideation (HI). But again, one of my supervisors informed me that regardless of his denial of SI and HI, it was imperative that I report his spiritual experience to his nurse due to the fact that she prescribed him medication and that operating as a team in our department was a requirement.
Embodying Juan, my supervisors, and others who played part in the dilemma, such as the psychiatric nurse, helped to increase my understanding of their positioning in the case. My movement consisted of taking on each person’s postures and gestures, and verbalizing notable statements from our encounters. My kinesthetic empathy allowed me to view the case from their perspective. I felt each person’s concern for safety: safety for the patient, the hospital, the college, and each person involved in the dilemma, including myself. To consider safety for everyone and everything taking part in the ethical dilemma, it required diverse methods of examination, risk management, and knowledge. My movement responded with openness to the varying perspectives of stakeholders.
Identifying the OptionsLastly in step two, Hervey found it helpful to encourage participants to imagine the most ludicrous option and move it (Hervey, 2007, p. 103). In this way, options disregarded due to fear and being premeditated as unethical decisions become spontaneous possibilities to solving one’s ethical dilemma (Hervey, 2007). Identifying options will help counselors focus their energy during complex ethical dilemmas. In Table 2, I present options considered for Juan’s case. Ultimately, I wanted to avoid causing harm to him and his beliefs by providing space for autonomy and cultural advocacy. Conversely, I was thoughtful about improperly treating a patient who may in fact benefit from receiving a diagnosis in alignment with his symptoms.
Table 2 Options Considered for Juan’s CaseStep Three and Four: Search, Evaluate, and DetermineHervey (2007) joins steps three and four of Welfel’s (2001) ethical decision-making model into one complete phase to evaluate options and to determine the best solution. It requires dance/movement therapists to utilize professional literature, ethical codes and regulations, and agency policies to provide structure for later deliberating processes (Hervey, 2007). Referencing codes, regulations and policies, as implied by Constable, Kreider, Smith & Taylor (2011), helps novice therapists navigate the uncertainties associated with ethical decision-making. Even for experienced counselors, this step remains a priority for continued growth and development and enhanced ethical judgment (Oramas, 2017). Ethical standards are designed to protect professionals and patients; yet, these standards usually result in more reactive than proactive ethical decision-making (Trahan & Lemberger, 2014). So in addition, seeking guidance from ethics scholarship enables counselors to vicariously learn by trial and error from practiced professionals. Aside from providing clarity, focus, and structure, this step also increases confidence through skill building and acquisition of ethical knowledge, and further limits risky decision-making. Once all relevant information has been obtained regarding options identified in step two, dance/movement therapists are to move out those possibilities. It is essential to utilize this step as an explorative measure with movement to create more available options than to rely on rules to quickly resolve the dilemma (Hervey, 2007).
Codes and ScholarshipThe ethical dilemma of respect for culturally based meanings in treatment and how mental health clinicians identify pathology is related to the American Dance Therapy Association’s (ADTA, 2015) ethical standard of display of integrity within the therapeutic relationship. It states, “Dance/movement therapists encourage the patient’s voice in treatment and respect the patient’s right to make decisions based on personal values” (ADTA, 2015, p. 3). The ADTA (2015) Code of Ethics additionally encourages dance/movement therapists to continuously reexamine their own biases and worldviews to avoid imposing them onto patients, and to consider the impact of oppressive systems on individual patient experiences. According to these ethical codes, Juan had every right to name his spiritual experience as he saw most fitting with his beliefs. Providing space for Juan to do that directly aligned with my obligations as an intern dance/movement therapist. However, the hospital did not ascribe to these standards. Though Juan experienced a sense of safety in my office space, we were a part of a larger operating system that he relied on for treatment.
The American Counseling Association’s (ACA, 2014) ethical code Avoiding Harm and Imposing Values states that counselors work to avoid harm and minimize potential harm to patients. I perceived there could be potential harm in revealing Juan’s undisclosed information to the treatment team. Counselors are trusted with the safety of each patient as they enter our therapeutic spaces, and as humans who have accepted the responsibilities of a counselor as a life calling, we feel competent enough to complete this task. Avoiding harm requires more than providing evidence-based interventions, private and clean spaces for therapy, judgment-free zones, and upholding ethical standards. It requires constant self-awareness and reflection, and honoring cultural differences.
The ADTA (2015) Codes of Ethics are informed by and parallel the ACA (2014) Code of Ethics. It is acknowledged that the ACA Code of Ethics was constructed and shaped by an individualistic, Western society (Birrell & Bruns, 2016) and remains firmly established in a modern society that accordingly places emphasis on rules, independence, and power-over rather than relational engagement and power-with patients in treatment. Ergo, complex situations in treatment settings become central when persons in power are compelled to make ethical decisions regarding the well-being of a patient, even when cultural beliefs conflict (Laws & Chilton, 2013). The patient in this case had a different cultural meaning of issues regarding his psyche than that of the hospital setting where he received treatment.
The Diagnostic and Statistical Manual (DSM) of the American Psychiatric Association (APA) is a manual of classified mental disorders that serves as a guide for interventions and treatment recommendations. In the DSM-5 (APA, 2013), a practical diagnosis for Juan’s case would fall under schizophrenia spectrum and psychotic disorders given his presentation of what the mental health field considers visual, auditory, and somatic hallucinations. Overtime, the DSM-5 has integrated cultural factors into disorders in the form of V-codes, described as supplementary conditions influencing a disorder. V-code 62.89, “Religious or Spiritual Problem”, accounts for loss or questioning of religion or spirituality (APA, 2013, p. 725), however, this code does not encompass religious or spiritual factors as it pertains to this case. The option of diagnosing Juan carried the risk of deterring him from seeking therapy and decreasing his overall well-being. A diagnosis would suggest that his cultural interpretation of his spiritual experience was either false or meaningless. Timimi (2014) and Allmon (2013) are clear that these types of interpretations of culturally based beliefs disempower the patient and could increase negative symptoms.
The second professional value listed in the ACA’s (2014) code of ethics honors and supports, “the worth, dignity, potential, and uniqueness of people within their social and cultural contexts” (p. 3). Since values are the cornerstone of which ethical decisions are carried out, counselors are to refrain from submitting a diagnosis if they know that it will cause harm to the patient in some way (ACA, 2014). It is rational to consider how the stigmatization of an oppressive label from the western culture will cause individual, cultural, and societal adverse consequences for some patients (Ratts & Hutchins, 2009).
Social consequences for the patient must be taken into consideration when making ethical decisions (Zheng, Gray, Zhu & Jiang, 2014). Usually in the decision-making process, the counselor identifies the ethical dilemma, takes the necessary steps to problem-solve outside of the therapy room, and decides on a resolution to the dilemma absent the patient’s voice (Birrell & Bruns, 2016). Yet, the ACA’s (2014) code of ethics states that counselors work collaboratively with patients to promote growth and development during an ethical decision-making process. Shared decision-making (SDM) is a model that was first developed in the 1980′s to improve the experience of patients in treatment settings by encouraging a collaborative process between the patient and health professional (Bradley & Green, 2018). This comes with controversy regarding the risks of granting access to a patient, which allows them to collaborate with doctors regarding their treatment, given their level of competency of medical knowledge may be limited (Christine & Kaldjian, 2013; Herlitz, Munthe, Torner & Forsander, 2016). The same is true to consider when patients are invited to autonomously collaborate in counseling settings.
Embodiment of Steps Three and FourAs I embodied the Effort weight, for this ethical dilemma, I found strong feelings surfacing about my cultural identity and the desire to advocate for marginalized groups. There was increasing pressure in my upper body and I associated this with the idea of fighting oppressive systems at my site, as well as healthcare systems in general. I let that increasing pressure sink downward into my lower body and invited decreasing pressure to my upper body. The anger and frustration of having to engage with such a system did not disappear, however, awareness of my embodied experience encouraged me to take a gentler approach to ethical decision-making.
I had a lot mixed feelings that were reflected in my movement while searching the ethics codes and gathering information. I felt confused and surrounded by information as I turned in circles reaching and pulling. The information seemed full of loose ends and, to a great extent, required interpretation. There was increased tension in my shoulders, and I eventually distanced myself from the imaginary visual of the ethics codes and scholarship. I entered into a remote state of increased bound flow and directing as I gazed at the information from a far. I began to move in my preferred style of popping and locking while visualizing the information regarding the clinical case. I was able to bring in my culture when understanding and interpreting the codes. Although complete clarity of the codes was not realized, I experienced increased confidence and intention for working through the dilemma with this new knowledge.
Step Five: Ethical PrinciplesStep five requires reference to the five ethical principles identified by Kitchener (1984). They are: autonomy, nonmaleficence, beneficence, justice, and fidelity, along with the added principle: veracity. Ethics involves cultural norms, personal morals, and values during the decision-making process, and these will serve counselors in the self-exploration process of relating to the guiding principles (Evans et al., 2012). Ethical principles were conceptualized to provide a foundation of morals to help interpret ethical codes and adjust routine responses to unconventional ethical dilemmas (Chmielewski, 2004).
Each ethical principle has been layed out with common movement qualities that were found by dance/movement therapists when they moved out the principles separately (Table 1; Hervey, 2007). A key part of step five is to be attentive to any embodied responses that are experienced while moving each principle. Principles have the potential to draw out essential details to help us strengthen our understanding of the dilemma and where the conflict is coming from, externally, and internally within ourselves in the form of values (Miller & Davis, 2016).
Another key factor is to acknowledge that these principles were created as a guide to culture-specific standards of behavior, and that ethical principles will be prioritized differently within varying cultures (Gauthier, Pettifor, & Ferrero, 2010). The new age invites new rules of behaviors, and these rules are changing rapidly (Hoose, 1986). It is important to be aware of the cultural body’s response to each principle and how it shapes our experience with them.
AutonomyAutonomy describes mutual respect in a relationship, where both individuals honor one another’s ability to make autonomous decisions (Kitchener, 1984). During complex ethical dilemmas, counselors may feel an urgency to act on impulses, yet feel the tension of respecting the autonomy of the patients, others involved, and that of themselves (Hervey, 2007). Indeed, the act of yielding and pushing through movement, which can be realized in dance/movement therapy, informs our boundaries and asserts greater independence (Schwartz, 2018).
There was constant pushing in my movement to create boundaries while embodying autonomy. I used my arms to separate and push back on the healthcare system to provide space for Juan and myself. It felt like I was taking on the role of advocate: working to gain autonomy for two people of color in a Eurocentric hospital setting. While moving I wondered how much autonomy could I actually encourage Juan to have given his presentation of symptoms and possible limitations of mental health information. Juan had previously omitted important details regarding his symptoms because he did not feel safe. I cautioned myself against allowing too much space as I thought about what other information might be unknown about him. As I moved and created space for myself, I realized I needed separation from both Juan and my internship site to be free in my own autonomy. In a cultural sense, autonomy for me meant expressing and standing strong with my own beliefs. I had responsibilities as an intern clinician to uphold the policies at the hospital, policies that I understood to be Eurocentric cultural norms and did not fully agree with. However, as a novice clinician, how much autonomy could I possess given my own limitation concerning the knowledge of policies and procedures regarding the clinical case? I engaged in a back and forth movement, suggesting the tug between inviting space for autonomy and enclosing space where autonomy may have been less beneficial to resolving the dilemma.
NonmaleficenceNonmaleficence means not causing harm to patients, including intentional actions to harm or carrying out risky actions that have the potential to harm them (Kitchener, 1984). This ethical principle corresponded with careful, cautious, and tentative movement responses (Hervey, 2007).
I attuned to my visceral experience of decreasing pressure and binding flow, as suggested by Hervey (2007), as I moved carefully. There were multiple pieces to consider to avoid harm. I wanted to culturally empower Juan and I wanted to keep him safe; however, safety could have looked like many things from the different perspectives of everyone involved in the dilemma. Safety could look like Juan feeling empowered and gaining trust in the healthcare system because he felt heard and believed by his treatment team. Safety could look like diagnosing Juan and giving him medication from the nurse’s perspective. Safety could look like informing Juan’s treatment team and engaging in ongoing investigation of his symptoms from my supervisors’ perspective. Safety could also look like keeping the information to myself and linking Juan to spiritual healers in nearby communities. I engaged in movements that looked like dipping and dodging as I moved, carefully considering all of these pieces that surfaced. I further examined my own safety in relationship to nonmaleficence. A decision to inform Juan’s treatment team would potentially cause harm to my cultural identity; I would feel like I betrayed my values and my community by going against street codes and abiding by rules of a mistrusted healthcare system. On the other hand, a decision to not inform the treatment team would leave me feeling disconnected as a team member at the hospital and also feeling like I am not doing my job correctly as a clinician; both would cause harm to my professional identity.
BeneficenceBeneficence is the act of reducing human suffering by supporting the welfare of others and enhancing their sense of empowerment (Jennings et al, 2005). This was a principle that I found myself sitting on during the time of my ethical dilemma. There is a two-sided impression of what doing good actually looks like; it could be the literal act of taking action to do good, or it could involve being good in a time of complexity and chaos (Hervey, 2007). Naturally I wanted to advocate for Juan by taking action, and I deemed it necessary for a culturally embedded case. Robson et al., (2000) argues that beneficence carries the obligation for counselors to seek substantial knowledge and perform in the best interest of the patient’s welfare. On the other hand, I felt that beneficence was just being good for my patient by offering a therapeutic space where his cultural interpretation of his experience was true, regardless whether the site was willing to change its process of labeling pathology. My upper torso instantly advanced forward in the sagittal plane without hesitation, my head shook side to side suggesting the word no, my limbs supported me with increased weight. My body gladly considered no other option but to actively engage in this clinical case by advocating for Juan and other underserved people who could benefit from a change in the healthcare system.
JusticeJustice, as an ethical principle, means fairness, treating others as equals, and promoting equality counseling. This ethical principle was most challenging for me to embody. In my body I felt stuck with increased bound flow at thoughts of how inequalities in healthcare systems continue to persist. In my exploration of balancing movements for justice, my body maintained its bound flow in every part except my arms. My bound flow was accompanied by rage and sadness. I attempted to take on the posture of the scales of justice with my hands held outward to the side; they felt empty and light. I brought my hands in front of me, side-by-side, and gazed at the emptiness for a moment. The ethical codes themselves require revamping to address the inequalities that exist within them (Kitchener, 1984; Robson, et al., 2000; Trahan & Lemberger, 2013). ‘It started to become clear that Juan’s case was a step forward in advocating for others like him who want and deserve fair and culturally sensitive treatment. This clinical case study was a component of seeking justice in itself.
FidelityFidelity is an act of faithfulness; it is about remaining loyal and keeping promises to patients (Kitchener, 1986). This was another challenging principle to embody. The moment a counseling relationship is established, there is an obligation on the part of the therapist to honor commitments and promises, and to fulfill the responsibility of trust and accountability (Wade, 2015). While some dance/movement therapists affiliated fidelity with commitment, honesty, and integrity, others associated it with retaining secrets. I considered how this principle could relate to one of my options: doing nothing and disregarding my patient’s spiritual experience in an effort to protect Juan from harm. During my embodied experience, I felt the sensation of being pulled in different directions with an uncomfortable tingling sensation in my stomach. I was confounded, caught in the middle of both my developed and emerging identities. On one end, I felt a pull from my patient to be with him in our marginalized identities. On another end, I felt pulling from my internship site and the counseling field to be an ethical therapist. Lastly, I saw an image of me pulling myself to just be me and to separate from both. I resorted back to autonomy and engaged in boundary setting movements, realizing that being faithful and honest to myself was my first responsibility.
Healthy disconnections are a key factor in the RCT framework. I refused the idea of becoming enmeshed with either the hospital or my patient during process of navigating the dilemma. I desired a healthy balance of connecting and disconnecting, which meant standing in my own identity while engaging with the clinical case. I reflected back to autonomy while moving this dilemma; fidelity helped me see where multiple truths encountered and overlapped one another. The nurse practitioner’s truth may be helping others in an informed way by assigning diagnostic labels in order to effectively treat multiple patients and prescribe medication. The nurse’s truth overlapped Juan’s truth of seeing his mental concerns as something spiritual, but not having many resources to turn to for support. I understood fidelity as a principle to encourage all involved in the case to be true to themselves and not place rules and labels above being human.
VeracityVeracity was added to the most recent addition of the ACA’s (2014) Code of Ethics and is defined as dealing truthfully with individuals during professional interactions. In my embodiment of veracity, I discovered a vertical stance that turned into spiraling movements of my spine with free flow and lightness. I felt authentic and vulnerable in my movement, and I also felt the willingness to share myself and connect with others involved in the ethical dilemma. True veracity requires authenticity to be effective; vulnerability is a bonus. It goes back to fidelity and being aware of placing rules above respect for human differences. The dilemma in this clinical case rose from a lack of acknowledgement of cultural differences and viewing ethical dilemmas through intellectualized codes instead of the truth within the human body.
Step Six: Consult and ShareWhen does spirituality become pathology? How do we ethically honor a patient’s cultural meaning of spirituality in a westernized medical system? These were the questions that had surfaced for me in supervision. Interestingly, I had three White identifying supervisors, and I was one of very few Black clinicians in training at my academic setting and the only Black supervisee at my site. There is an established power differential that comes with a supervisee-supervisor relationship which was compounded by Black-White dyads that constituted each of my supervisory relationships. Clinicians of color in training commonly experience their voices being silenced in clinical and academic settings, especially when topics of culture and race need to be addressed (Estrada, 2005; Hardy, 2015; Hernández, 2003; Jernigan, Green, Helms, & Perez-Gualdron, 2016). This is likely a consequence of practiced cultural conditioning in Western societies as well as a lack of cultural awareness and training that has persisted throughout the counseling field, thus continuing the cycle of supervisors overlooking cultural issues (Estrada, 2005; Vereen, Hill, & McNeal, 2008; Jernigan, et al.,
留言 (0)