
記住我



In this section, we will consider the challenges and issues and the ways forward for research in six areas: definitional issues that set the agenda, the international focus, research quality, theoretical sophistication, participatory research, and the need for multiagency and interdisciplinary working and awareness.
Definitional Issues That Set the Agenda for ResearchOne of the problems noted by researchers has been that there is no single definition of a young carer (e.g., Aldridge 2018). Without a universal definition it is difficult to assess prevalence of young carers and young adult carers consistently across studies. As such, estimates of populations of young carers are at variance with each other. Some use census information which is based on reporting by adults in the household. Others use self-identification methods by young people themselves. This is a problem insofar as researchers have seen a need to develop estimates of prevalence that are comparable across countries. Policy makers will be interested in knowing the extent of a problem and this drives researchers to develop such research. The difficulty of developing a clear definition is widely acknowledged by researchers as caring is a highly subjective and variable experience. We suggest, however, that the difficulty in definition is that caring is not one thing, and that once we disentangle it into its components it is possible to develop a clearer and more useful set of definitions. Below, we will provide what we think is a more nuanced conceptualization.
As already noted, “young carers” and “young adult carers” are social constructions, helpful in one way for drawing attention to an issue faced by many children and young people, but unhelpful in other ways if they reify the idea that this really is a single population of young people, all with the same issues, who are all adversely affected by their experiences in the same way. It is understandable that policy makers want to know what percentage of children and young people are carers but caring is on a continuum and is not a dichotomous experience in which the person is either a carer or not a carer. Also, there are different dimensions to care, for example, the extent of caring (i.e. time spent caring) and the type of care carried out, for example, household tasks or personal care. Striving to produce such an understanding tends to lead to percentages that are either over inclusive of all children who have some caring role or exclusive to those at the more extreme end of caring responsibilities.
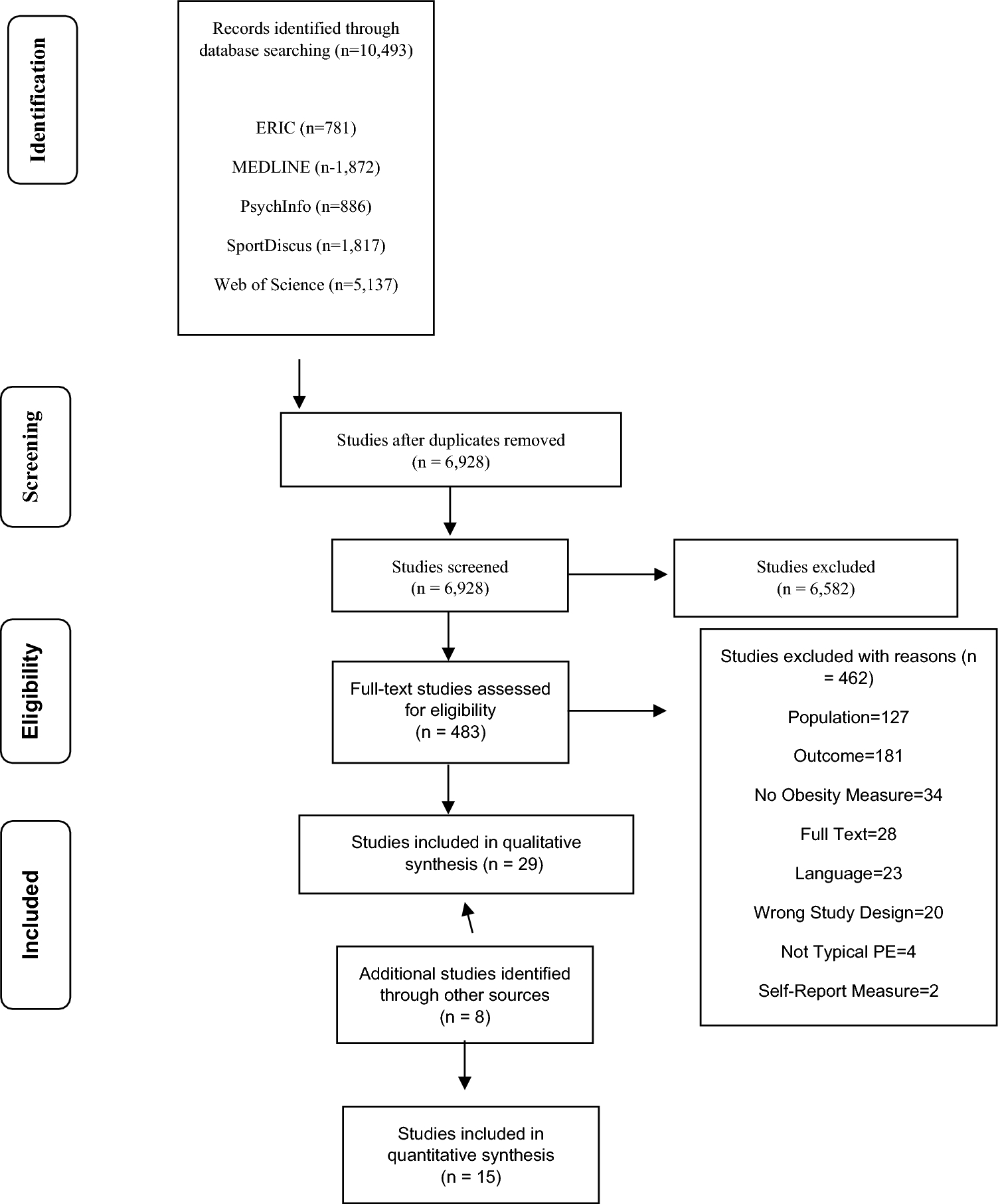
We have had personal experience of this in our own recent research in which we conducted a representative survey of 925 young carers in England (Joseph et al. 2019). Our approach to this was in two stages. First, we ascertained the percentage of children who provide some help, no matter how minimal, to someone in their home who was ill or disabled. We found that this was around 20% of all young people; these could, therefore, be classified as young carers in the very broadest sense. Second, using a standardized assessment tool that asks about caring responsibilities—a revised survey version of the Multidimensional Assessment of Caring Activities (MACA-YC18)—we ascertained the amount of caring that the young person did. We found that around 32% of the young carers were carrying out a “at least a high amount of caring” as defined by the assessment tool (7% of the total sample of all the young people), and 9% of young carers were classified as doing a “very high amount” of caring (3% of all young people). It is this latter smaller group that we would expect are most likely to experience difficulties and be adversely impacted by being carers, but it was the first figure of 20% of all young people that attracted the media attention and that of the various agencies concerned with promoting the welfare of young carers. All of the figures, 20, 7, and 3%, are correct, but it is only through understanding how they each represent different populations that more nuanced policy can be developed.
Becker’s (2000) definition that young carers are those that carry out, often on a regular basis, significant or substantial caring tasks and assume a level of responsibility which would usually be associated with an adults is often used. This is a broad definition, one which has come under criticism in recent years for a number of reasons; most notably that it excludes the impact of caring (Aldridge 2018). While we agree that bringing the focus on the impact of caring into the definition of what it is to be a young carer adds to the policy relevance, we would argue that this is too exclusive a definition. And, of course, children who provide care can still be categorized as “young carers” even in situations where there are few negative (or positive) impacts. One definition is too broad whereas the other we would argue is too narrow. But more importantly, it changes the focus of policy interventions to help with the burden of care to reducing the impact of caring on the carer. Policy needs to be able to address all aspects of caring.
As such, we think scientific enquiry should define caring in the broadest sense to be most inclusive in the first instance of all children who take on some caring role, and to understand the graduations of care along the continuum. We propose that caring can be best conceptualised as three concentric circles. The largest is young people who care about, i.e., those who are helping a relative in at least some minimal way with household activities but not to a greater extent than many of their peers who are not carers. The next is young people who care for, i.e., those who have taken on a level of responsibility that involves household activities but also more specialist and medical roles, but not to an extent that it interferes excessively with their social and educational activity. Finally, young people who themselves need care, i.e., those who have taken on caring activities well beyond the level of their peers who are not carers, involving specialized and medical activities, emotional work, and which prevents the young person engaging in the social and educational activities of his or her peers. Each group has its own distinctive needs. Recognizing this, policy targets can be more nuanced and responsive to the needs in families. In terms of policy and service goals, the implication would be to focus on prevention, assistance, and mitigation, respectively, as discussed by Purcal et al. (2012) in their analytical framework.
First, disabled and ill family members need to be provided with support such that children and young people are not required to provide care. This must always be recognised as a priority even if meeting such targets in full is unrealistic. Second, even if such support were available, because of family bonds and the wish to help, young people will always continue to provide care and they need support themselves to carry out their caring tasks. Resources need to be provided to young people to help them carry out their caring tasks. Finally, there is a need to be able to identify those children and young people under the most burden who are adversely affected and in urgent need of help not to support their caring activities but to support them and their mental health, education, and other ways in which they are impacted. Most often this will be to help with educational and psychological difficulties, but in some contexts there may be physical risks. This more nuanced definition goes some way toward avoiding problematizing the childhood of all young people who care.
Qualitative research with young carers themselves shows that they themselves feel that the best way that services can support them is to better support their cared for relatives (Moore and McArthur 2007). When asked about their own needs, young carers ask for assistance to participate in community life, to attend school, and to have opportunities to take a break from their caring responsibilities (Moore and McArthur 2007). These are intertwined policy objectives that need to be addressed simultaneously; research designed more explicitly to shape the policy agenda in all three ways rather than being responsive to a more simple notion of caring as a simple dichotomy.
As research moves forward, we must recognise the subtle graduations of caring and that no single definition is adequate. The terms young carer and young adult carer are broad descriptors only, as this is not one single population. We think our concentric circles model is a useful conceptual tool that encompasses different definitions and has clear policy implications.
Developing the International Policy FocusYoung carers are a global phenomenon and slowly, one by one, countries are beginning to respond to the challenges they face. There is a need to promote research to support and develop locally-based research and international comparisons. However, related to our discussion above, caring is a social construction that is understood in relation only to expectations of what are appropriate duties for a child or young person to take on. It is clear that we are coming from a frame of reference were it is seen as inappropriate for young people to take on unpaid roles of caring that are associated with trained professionals, but these expectations of normality vary from country to country. Thus, a single universal definition that allows meaningful comparisons across cultures is not possible, in the sense that in one culture a young person could be classified as a carer but not in another. Research which attempts such comparisons must be wary of cultural colonization and exporting the expectations of one culture to another. In this respect, Robson (2004) in writing about the child carers in Zimbabwe states that there needs to be less emphasis on the ideas of childhood as a time of play and innocence and more emphasis on defending their rights to work and be supported in their work.
Young carers do not always self-identify as such, often viewing what they do as part of a normal familial relationship with bonds of reciprocity and love (Smyth et al. 2011); but on the other hand when they do recognise themselves as young carers it can be against a backdrop of expectations about what normal childhood is supposed to be like, thus seeing themselves as somehow deficient (O’Dell et al. 2010). Such a conclusion is borne out by research in a Western context but other research by Skovdal and Andreouli (2011) has shown how in Kenya, there is a different recognition of childhood, in which children are seen as active agents of community life.
Research must approach the topic from within each culture’s frame of reference. As such, many factors can affect the policy response including the presence of country-specific research and local championing organizations. However, where resources are scarce, particularly in so-called developing countries, simply showing that young carers are present will not lead to a response—there are insufficient resources to provide support for that specific group. There is need for discussion on what sort of services and interventions are necessary or appropriate. For example, do we need specific services that are tailor-made for young carers? Or can we use generic services to good effect? And when resources are scarce, how can they best be used to improve the lives of young carers?
One dilemma that arises from the research on young carers is whether children in countries which have no welfare benefits system should be paid for their role as carers so as to obviate their need for finding outside employment? But, if children are paid to continue to act as carers they may become locked in their caring roles and their access to schooling and education will be restricted. This limits their life chances and prevents them from achieving higher goals and better-paid employment. Such young people need appropriate support to break out of the spiral of poverty and caring, and enable them to achieve against the UN Convention on the Rights of the Child and Global Millennium Goals. Most controversially perhaps, it could also be argued that providing support for young carers in any country, rather than providing adequate care for the person they care for, also locks children into an inappropriate caring role and parents into a reliance on their children. Thus, while we think it valuable to use tools and methods that allow for cross-cultural comparisons in research findings, how these findings are interpreted and used by policy makers will not necessarily be the same. Each of our concentric circles has a different policy objective, but which of the circles is given prominence by policy makers and whether the focus is then primarily on prevention, assistance, or mitigation will depend on cultural understandings of childhood, the nature and extent of familial illness, and economic factors.
Ethics of Developing the Quality of MethodologyA broad base of evidence around the nature of caring, its prevalence and potential impacts has been established. As discussed, small scale qualitative research has been carried out with groups of young carers identifying various difficulties. Some survey research has been able to produce figures that give some indication of how widespread problems may be, but on the whole, this work has been with small and selected samples that do not permit generalization and importantly an understanding that the impacts actually arise as a result of caring. One approach to this latter issue has been to ask adults to retrospectively report on their experiences of caregiving (Lackey and Gates 2001) but while this adds weight to the observation that caring has consequences, it is methodologically limited.
Other statistical correlational research is able to show associations between variables. For example, social skills were found to be positively associated with a higher extent of caring activities (Kallander et al. 2018), but due to the cross-sectional nature of the study it is not clear if children take on caring due to their high social skills or if they develop social skills as a result of caring. Similarly, we know that many young carers experience bullying but what we don’t know is whether their victimization is a result of their caring and whether the extent of their victimization exceeds that of young people who are not young carers. To find out we need prospective research and research that compares young carers with other young people.
To do this we also need new research that uses established tools that permit comparisons of findings to be made. In the past, much research has tended to use idiosyncratic measurement tools developed for single study use. However, various tools do exist, such as the Young Carers Perceived Stress Scale (Early et al. 2006), and the Multidimensional Assessment of Caring Activities (MACA-YC18: Joseph et al. 2009b). The latter tool is widely used by carers organisations as it yields scores for a range of caring activities, i.e., domestic activity, household management, emotional care, sibling care, personal care, and financial and practical management. This makes it useful for assessment purposes when used by social workers and health professionals. It has been increasingly used as a survey instrument across different cultures, including the United Kingdom (e.g., Becker and Sempik 2018), Sweden (e.g., Järkestig-Berggren et al. 2018), and Switzerland (e.g., Leu et al. 2019).
Increasingly researchers are in need of tools that allow comparisons to be made between young carers and their peers. As such, a revised survey version of the MACA-YC18 (Joseph et al. 2019) was developed to allow it to be used with all young people regardless of their caring role. The revised tool allows comparisons to be made between the everyday helping carried out by young people and those who are in a caring role. It is important to understand that many young people who are not in a caring role help around the home. Researchers need to understand what young carers do against the backdrop of the culturally expected and everyday level of helping by young people.
Tools to assess the effects of caring have also been developed, such as the Positive and Negative Outcomes of Caring (PANOC: Joseph et al. 2009a), which allows respondents to indicate to what extent they feel adversely affected on the one hand, and to have gained benefits, on the other. We think it is important to understand that caring can promote psychological growth for the young person. This is not to imply that we think caring is necessarily a positive event in the person’s life, but recognizes that in the struggles and challenges faced by the young person, growth can ensue. As such, a focus solely on the destructive aspects of caring is unbalanced and does not provide the scope to understand fully the ways in which policy interventions can be helpful. We think that policy should not be based solely on the idea of mitigation but also on promotion of positive psychological and educational factors. In this way, evaluations should assess not only that problems and difficulties are alleviated but also that positive qualities, such as resilience, strengths, and well-being, are fostered.
We believe greater methodological rigour is needed now to advance the field in the ways described above, but for us this is an ethical issue as well as a methodological one. There is a certain degree of saturation that seems to have been reached in the qualitative literature in describing the range of difficulties and problems encountered by young people who care. As such, we would argue that sufficient work that is essentially descriptive has already been carried out and future work needs to show clearly how it could add a step change to the body of knowledge. Otherwise, we feel research becomes increasingly questionable ethically, particularly in samples that may be upset by the research (Robson 2001), and who give their time without benefit to themselves or their families. The quantitative research is at a more developmental stage, particularly in producing generalizable findings, evidence of causal relationships between variables, and prospective research that can tell us about the impact on future adult life. Larger scale studies with representative samples to determine the extent and nature of the difficulties are needed. Small scale studies with selected groups of young carers simply cannot show conclusively the extent and nature of the problems faced by young carers as one homogeneous group. And as we discussed above in our concentric circle model, young carers are not a homogeneous group. The extent and nature of the problems will likely vary according to the distinctive needs of each group. As such, while we make the same assumption ourselves that many young carers will likely experience damaged educational prospects, poorer mental health, and restricted life opportunities, and so on, questions about the extent of the difficulties faced by young carers demands larger scale quantitative evidence if they are to be taken more seriously by policy makers.
More Theoretically Driven ResearchEvidence for the adverse effects of caring are limited in the ways described above, and recommendations for policy and practice currently often seem to go beyond the data, making assumptions that young carers will suffer from damaged educational prospects, poorer mental health, and restricted life opportunities. As discussed, there needs to be more rigorous quantitative work that allows for generalizability, understanding of causality, and long term effects; but alongside this there also needs to be greater theoretical sophistication.
For example, one of the pressing questions is whether caring has a statistical association with adverse outcomes. As we have seen, research findings on the relationship between the amount of caring activity and measures of well-being and mental health are mixed. However, this is not surprising as we should not expect a straightforward linear relationship between caring and other outcomes. It is known from other areas of similar research such as the stress and coping literature that such a relationship is likely to be moderated and mediated by a number of other factors. To date, research has tended to give too little attention to moderating factors. We must recognise that caring takes place in a sociological context. It is a heavily gendered activity (Aldridge 2018) and influenced by the role of ethnicity, culture, support systems across schools, communities and helping professions (Kavanaugh et al. 2016). How caring activity relates to health and wellbeing is expected to be moderated by such factors, that we might predict strong relationships between caring activity and health and well-being outcomes in some groups but not in others.
As such, we need more theoretically driven approaches. For example, the stress process model used by Kavanaugh (2014) to take into account background factors, the primary stressors of caregiving, but also the secondary stressors such as school performance and parent/child conflict is one example of how research can be developed. Other research by Pakenham and Cox (2015) uses a family ecology framework which takes into account stress-appraisals, coping strategies, and coping resources. Their findings emphasise that higher caregiving responsibilities have direct and indirect adverse effects on youth mental health in the context of parental illness. We might also look to the literature on posttraumatic growth for inspiration on how different personality, social, and coping-related factors are likely to mediate and moderate the relationship between the experience of caring and positive outcomes (e.g., Linley and Joseph 2004).
In particular, we need to understand more about the psychological appraisal factors within the person that mediate their experience of caring. Qualitative research has identified the ways in which young people think about their caring experience, whether they see it as just part of their life, themselves as a caring person, whether they feel they have a choice, and the burden of responsibility they feel (McDonald et al. 2009). It is clear that these very idiosyncratic appraisals of what it means to be a carer, while well documented in the qualitative literature, have failed to translate into the quantitative social survey research as new variables that can help to explain the complex appraisals that young people make that mediate the relationship between their caring role and other outcomes in their life.
In this way, there is a need to apply more sophisticated theoretical frameworks that can understand that caring and its outcomes are not necessarily as straightforward as has been assumed in some past studies, but rather only understood by a closer examination of moderating and mediating factors.
Young People and Those They Care for as Active ResearchersResearch with young people most often involves negotiating access through gatekeepers who will often have reasons to refuse access because of fears of a child protection intervention, invasion of privacy, or for other reasons that are deemed to actually be in the best interests of the young person or the family not to take part (Kennan et al. 2012). As such, we believe an important innovation will be for young carers researchers to step back from taking an expert frame of reference. While we think there is a need for greater sophistication in research from the researchers frame of reference, as described above, we also see opportunities for more participatory action research that engages with the young carers themselves and their families, from their frame of reference, and in their perceived best interests.
One study that offers a ground breaking example of more participatory research is that by Skovdal et al. (2009) in which young carers in Kenya used photography and drawing to provide accounts of their experiences. Their work helped to shift perspective from young carers as victims to competent social actors, and framed within a social psychology of coping. Other work of this nature has involved world café events led by young carers themselves providing insight into the here and now experiences of a group of young carers (McAndrew et al. 2012).
Participatory research with young people remains relatively rare (Raanaas et al. 2018) but finding ways in which research becomes more participatory, action-focused, and participant-led would seem to be especially responsive to what we have learned so far, in finding ways to engage more ethically with young people who care. However, as we know the time available to young carers to take part in other activities is limited, and as such their ability to participate in research will be constrained. In calling for more participatory research which is additionally demanding, we have an ethical duty to young people to provide sufficient resources so as not to add to their burden. Participatory research can be especially appealing to policy makers, more visible to the public creating awareness, and may also be helpful to the development and experience of the young carers themselves. We would encourage researchers and service providers to think about how a participatory research element can be built into existing and new plans.
Multi-agency and Interdisciplinary FocusIt has been argued that the concept of a young carer distracts from inadequate state services and legitimizes abuse of children, and as such, the focus should be on helping parents fulfil their roles, not in supporting children and young people to be carers (Morris 1997). As discussed above, we agree that it is important that the research into young carers is not misused in this way and that full attention must be given to supporting parents, and other adults with illness or disability, as a first priority of policy. But research into the experiences of young people themselves shows that it is not helpful to see this issue dichotomously and that even if parents are fully supported those identified as young carers would continue to have their own needs for support (Thomas et al. 2003). Prevention, assistance, and mitigation/promotion require a range of disciplines and professionals to be involved, i.e., educators, healthcare professionals, community workers, and social workers, all of whom bring different skills and expertise (Warren 2007). When not viewed in this dichotomous way, it is clear that the field demands a multi-disciplinary and multi-agency approach.
A study conducted in Germany (Kaiser and Schulze 2014, 2015) showed that professionals working in education, health or social care only regarded support provided by inter-agency cooperation to be effective for children and adolescents who had caring responsibilities and who had problems with school attendance. However, issues of professional confidentiality and the private (and hence invisible) nature of children’s caring roles undermined inter-agency working and support. Social workers have a central role as they are the most likely to be working with families of ill and disabled people. Educators and teachers must also be involved as they are in direct daily contact with young people. Within school contexts, ensuring that confidential guidance and counselling is available may be helpful given the often covert nature of caring which may prohibit the use of other services (Banks et al. 2002).
The recognition of the need for a multi-agency approach is mirrored in the need for interdisciplinary research. Each scholarly discipline brings with it its own set of assumptions and positionality. For example, sociologists may conduct research which emphasises the gendered nature of caring and the role of public policy in providing solutions to what are seen as culturally created problems. Psychologists may approach the topic from the perspective of the individual studying, for example, processes of coping and resilience, with suggestions for how clinical or counselling psychologists can be more involved.
But the topic of young caring crosses disciplines of sociology, psychology, as well as education, public policy, social work, law, medical ethics and others, and thus demands greater interdisciplinary working and awareness. For example, interest in resilience and coping may be a helpful line of investigation, but only if it is not at the expense of helping parents fulfil their roles. What we are suggesting is that truly interdisciplinary research is able to offer the bird’s eye view on any research and how its significance is positioned within the larger field. Related to this is that the professional groups traditionally involved with young carers tend to adopt an approach grounded in an illness ideology, so policy and practice can become overly driven by a focus on the pathological. While there is a role for this, research also stresses the personal growth, maturity, and identity formation processes pointing to the development of positive psychological and positive educational interventions, which we believe need to become more prominent as we move away in our thinking from an illness ideology that pathologizes young people who care. We need to do more than help young people cope, deal with the stress, and so on; we need to help them flourish.
留言 (0)