
記住我

What are the novel findings of this work?
In women with rectosigmoid deep endometriosis (DE), transvaginal sonography (TVS) is reliable for assessing lesion length but less reliable for lesion thickness and transverse diameter measurements.
What are the clinical implications of this work?
TVS enables accurate assessment of rectosigmoid DE lesion length, which is decisive for diagnosis, surgical planning and risk assessment. Thus, it can improve counseling of women with rectosigmoid DE.
INTRODUCTIONWhen surgical treatment is chosen for women with rectosigmoid deep endometriosis (DE), a multidisciplinary approach involving gynecological and general surgeons is often warranted1-3. Serious complications can occur as a result of rectosigmoid surgery, including anastomotic leakage and development of a rectovaginal fistula3-5. As a consequence, there is an ongoing debate on the optimal surgical method for removal of rectosigmoid DE1, 6, 7. Over the past years, there seems to have been a shift from more extensive surgery, including segmental resection (SR), towards more limited approaches, including discoid resection (DR) or shaving techniques, favoring a more tailored approach for each woman and according to the extent of disease3, 8. Transvaginal sonography (TVS) is a well-established first-line imaging tool for diagnosis and mapping of DE, with high sensitivity and specificity9, 10. Preoperative assessment of rectosigmoid DE lesion size using TVS is among the decisive factors to consider when counseling women on planning a surgical procedure and weighing the risk of complications1, 11, 12.
The International Deep Endometriosis Analysis (IDEA) group developed a systematic approach for describing TVS findings in women with DE in order to improve clinical practice and research13. Furthermore, an updated version of the Enzian classification (#Enzian) for endometriosis has been published recently, enabling clinicians to use a universal classification system for describing rectosigmoid DE on TVS and at surgery14. Optimal preoperative assessment of the extent of rectosigmoid DE, including the need for a temporary ileostomy, is crucial when planning surgery11. Detailed knowledge of the degree of DE could also prevent problems related to residual disease and repeat surgery in women with chronic pain and DE15, 16. Besides SR and DR, rectal shaving removes fibrosis on the bowel, but, unlike DR and SR, it does not involve a full-thickness resection. In simple terms, lesions < 30 mm in length can be treated with DR, while SR is recommended for larger lesions1, 17. Some groups have suggested that DR carries a lower risk of complications compared to SR, but functional results may not differ3, 18, 19. Measurement of all three diameters of rectosigmoid DE lesions, namely the craniocaudal–midsagittal, anteroposterior and transverse diameters (hereafter referred to as length, thickness and transverse diameter, respectively), is pivotal and recommended by the IDEA group13. From a surgical point of view, lesion length is the most important of these three diameters in determining surgical technique17. In a single-center study, Di Giovanni et al.20 reported that there was no statistically significant difference in measurements of the three diameters of rectosigmoid DE lesions when comparing preoperative TVS and surgical bowel specimen measurements. The aim of this study was to investigate all three diameters of rectosigmoid DE lesions in a multicenter setting using the IDEA group's definition13, comparing preoperative TVS with postsurgical measurement (PSM) of fresh bowel specimens.
METHODSWomen scheduled for elective surgery with DR or SR due to symptomatic rectosigmoid DE were recruited consecutively, between April 2017 and December 2019, from three tertiary referral centers for endometriosis, namely Hospital St John of God Vienna, Vienna, Austria; Oslo University Hospital, Oslo, Norway; and Nepean Hospital, Sydney, Australia. In all three centers, the gynecological surgeons perform preoperative TVS when planning surgery and counseling women. Exclusion criteria were previous bowel surgery, age < 18 years, virgin and menopause11. Women who underwent bowel shaving were excluded, as they did not undergo full-thickness resection, and a postsurgical specimen for measurement of the three dimensions of the lesion was consequently unavailable. Before the start of the study, we decided that rectosigmoid DE lesion length was the most important diameter for surgical planning17. All women included in the study underwent TVS followed by SR or DR for rectosigmoid DE. Measurements obtained by TVS were compared to measurements derived from the surgical specimen. The study was approved by the local ethics committee of Hospital St John of God in Vienna, Austria; the Regional Ethics Committee for Medical Research in Norway; and the Nepean Blue Mountains Local Health District Human Research Ethics Committee in Australia.
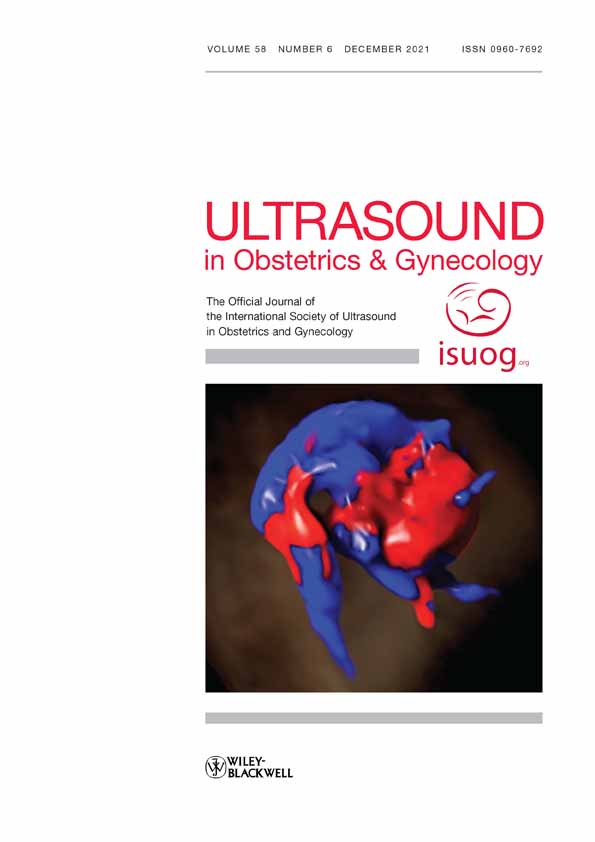
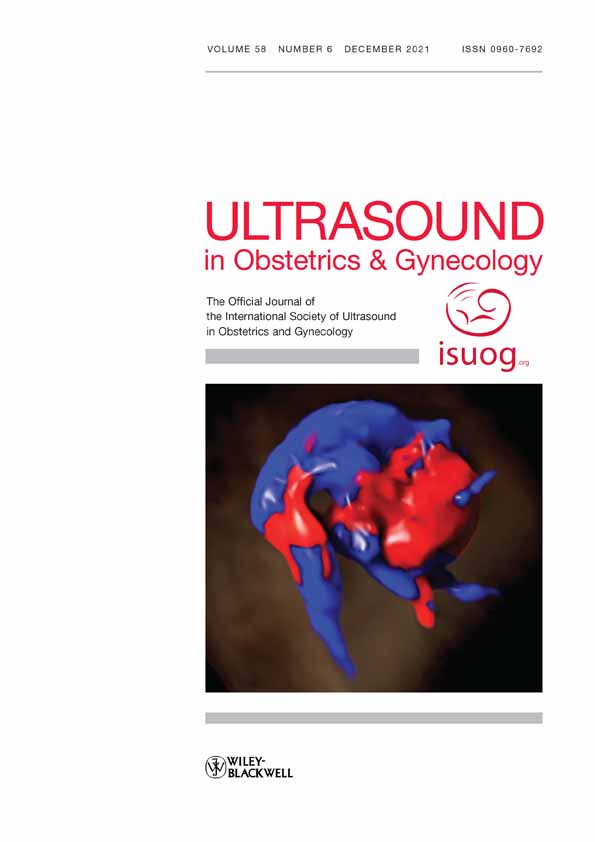
Transvaginal sonographyTVS examinations were performed in a systematic manner for DE of the anterior and posterior pelvic compartments13. Rectosigmoid DE lesions appear on TVS as hypoechoic thickenings or nodules, usually affecting the muscularis layer of the bowel wall13, 21. Length, thickness and transverse diameter measurements of the lesion were recorded, as described by the IDEA group13. The length and anteroposterior thickness ofthe lesion were obtained in a still midsagittal plane (Figure 1a,b). The transverse diameter measurement was recorded in a still image after having turned the TVS probe in the transverse plane at the level of the maximum thickness of the lesion in the midsagittal plane (Figure 1c,d). In cases of multifocal lesions that were attached to each other, the total length of the bowel lesion involved was measured. The thickness and transverse diameter measurements of multifocal lesions were obtained at the thickest part of the lesion. No preoperative bowel preparation was utilized, as this is not routine practice in any of the three study centers. Ultrasound examinations were performed by G.H., M.K.A., G.C. or M.Le. All four examiners are gynecological surgeons who routinely carry out TVS in tertiary referral centers. A Voluson E8/10 ultrasound machine with a 5–7-MHz transvaginal probe with three-dimensional facility (GE Healthcare, Zipf, Austria) (G.H., G.C., M.Le.) or a Samsung WS80A ultrasound machine with a 5–9-MHz transvaginal probe with three-dimensional facility (Samsung Healthcare, Seoul, Republic of Korea) (M.K.A.) was utilized.

(a,b) Transvaginal ultrasound image (a) and schematic diagram (b) in the midsagittal plane, showing a rectosigmoid deep endometriosis lesion, with caliper placement for lesion length (A) and thickness (B) measurements, according to the International Deep Endometriosis Analysis (IDEA) group consensus. (c,d) Transvaginal ultrasound image (c) and schematic diagram (d) in a transverse plane, showing a rectosigmoid deep endometriosis lesion, with caliper placement for transverse diameter (C) measurement, according to the IDEA consensus.
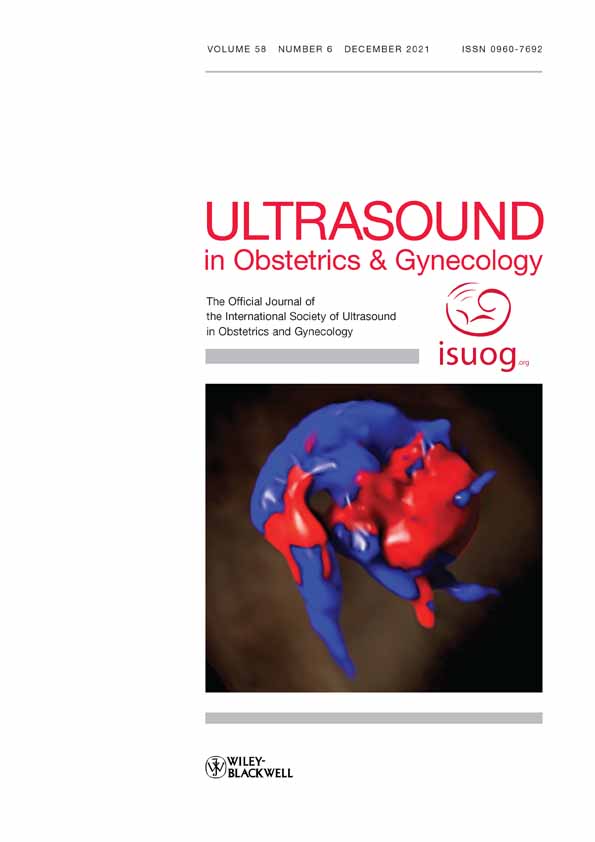
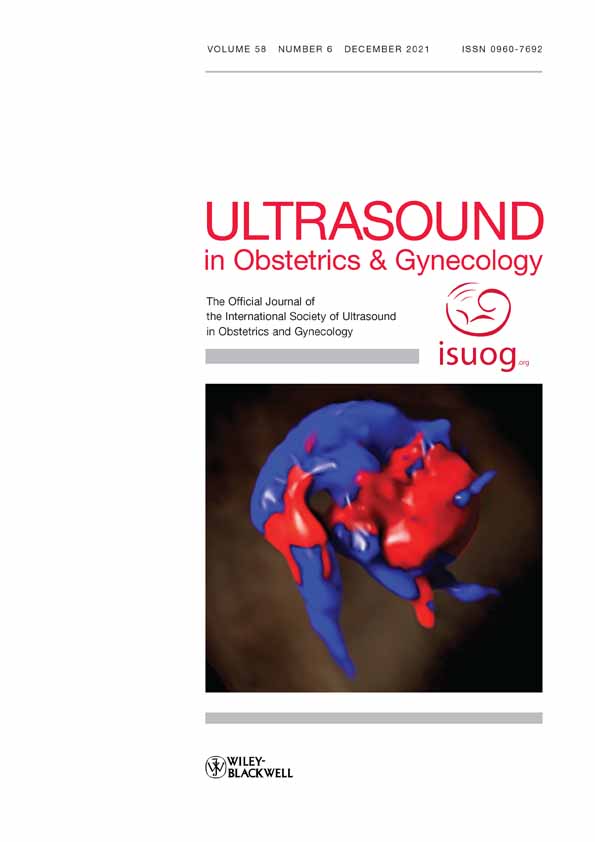
Surgical procedure and postsurgical measurementSurgery was performed in each institution by a multidisciplinary team consisting of gynecologists, general surgeons and urologists2, 3. The surgical procedures for DR and SR have been described previously in detail3. The final decision regarding the preferred surgical technique was made intraoperatively in collaboration with the gynecologist and general surgeon. However, in general, in cases with a rectosigmoid DE nodule with length < 30 mm on preoperative TVS, full-thickness DR was the preference22. Conversely, in women with a rectosigmoid DE nodule with length > 30 mm on preoperative TVS, full-thickness SR was the preference. PSM of freshly extracted specimens was performed using a ruler (Figure 2). Initially, the specimen was cut in the midsagittal plane to obtain lesion length and thickness, and then in the transverse plane for transverse diameter measurement. The three diameters were recorded. Histopathological confirmation was obtained and was defined as endometrial glands and stroma in the resected bowel specimen23. Severity of DE was classified during surgery according to the revised Enzian score24. The revised American Society of Reproductive Medicine (rASRM) score, which was not developed specifically for DE25, was also registered.

Postsurgical specimens of rectosigmoid deep endometriosis lesions after segmental resection (a) and discoid resection (b).
Statistical analysisThe degree of agreement between TVS and PSM was examined for lesion length, thickness and transverse diameter measurements using Bland–Altman plots and limits of agreement (LoA) of the differences26, 27, Pearson's correlation coefficient28 and intraclass correlation coefficient (ICC)29. Data were log-transformed before performing analysis of agreement because the distributions of length, thickness and transverse diameter measurements were skewed. The key estimates, such as mean and lower and upper limits of 95% CI, were transformed back to the original scale, using antilog. Bootstrap method was used for correlation analysis to obtain bootstrapped 95% CI, which was based on 2000 replications of the dataset. The ICC was based on absolute agreement with a two-way random-effects model for test–retest reliability29. Values < 0.50 indicate poor reliability, values of 0.50–0.75 indicate moderate reliability, values of 0.75–0.90 indicate good reliability and values > 0.90 indicate excellent reliability29. Average differences in measurements of length, thickness and transverse diameter between TVS and PSM were tested for statistical significance using a paired-sample t-test and the significance level was set at 0.05. The clinically acceptable average difference between the methods and LoA were set to ± 10 mm for all three dimensions. Regression analysis was performed to investigate factors that could influence differences in measurements. Analyses were performed using IBM SPSS Statistics for Windows, version 26.0 (IBM Corp., Armonk, NY, USA).
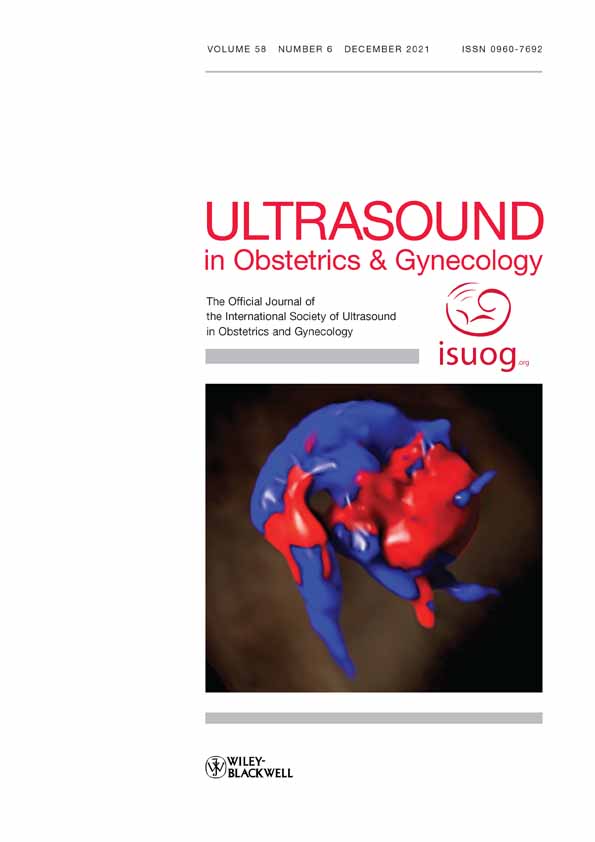
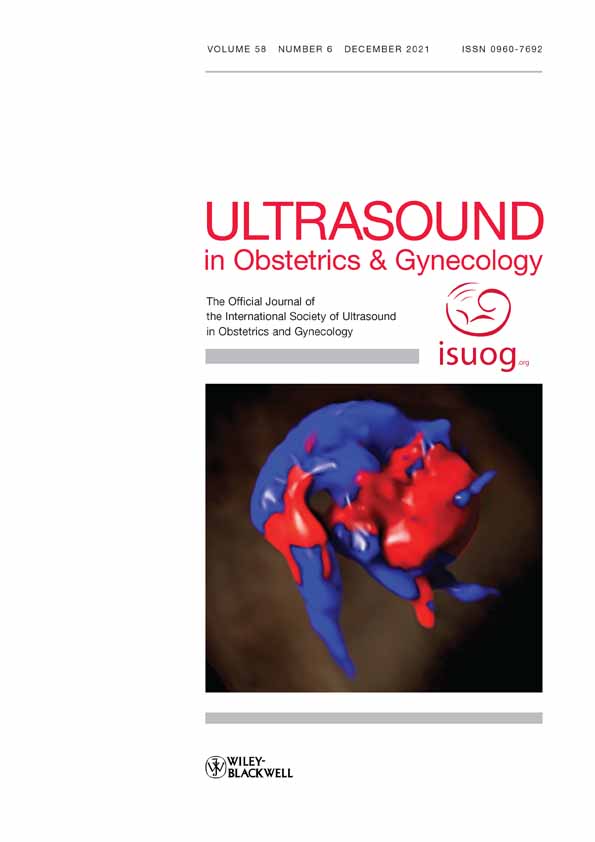
RESULTSFrom April 2017 to December 2019, 207 consecutive women were eligible for inclusion (Hospital St John of God Vienna, Vienna, Austria; n = 112; Oslo University Hospital, Oslo, Norway; n = 75; Nepean Hospital, Sydney, Australia; n = 20). Forty-one women were excluded, leaving 166 women for analysis (Figure 3). Demographic details and surgical procedures are displayed in Table 1. A total of 123 SRs and 46 DRs were performed. In three women, both procedures were performed. Fourteen women underwent a planned temporary ileostomy. Three women underwent a postoperative temporary ileostomy due to anastomotic leakage.

Flowchart summarizing inclusion of women undergoing surgery for rectosigmoid deep endometriosis.
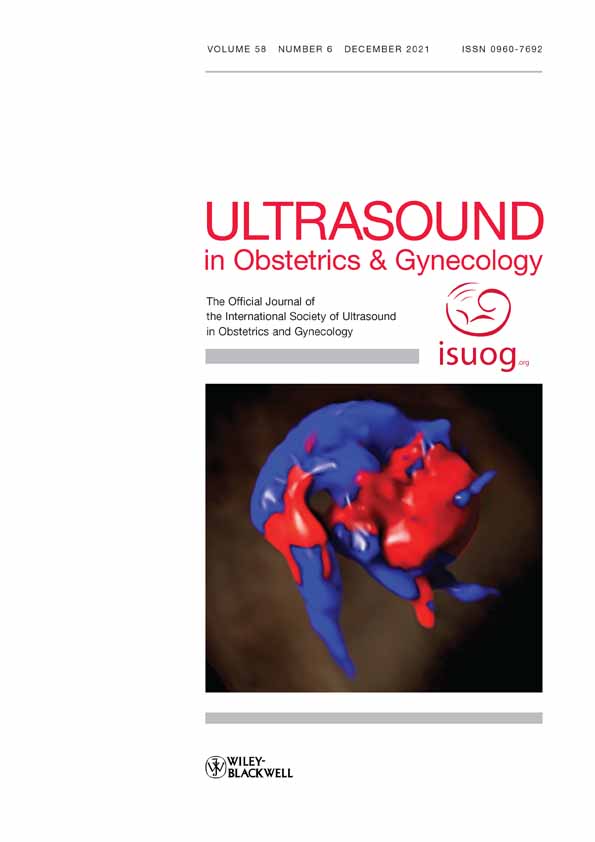
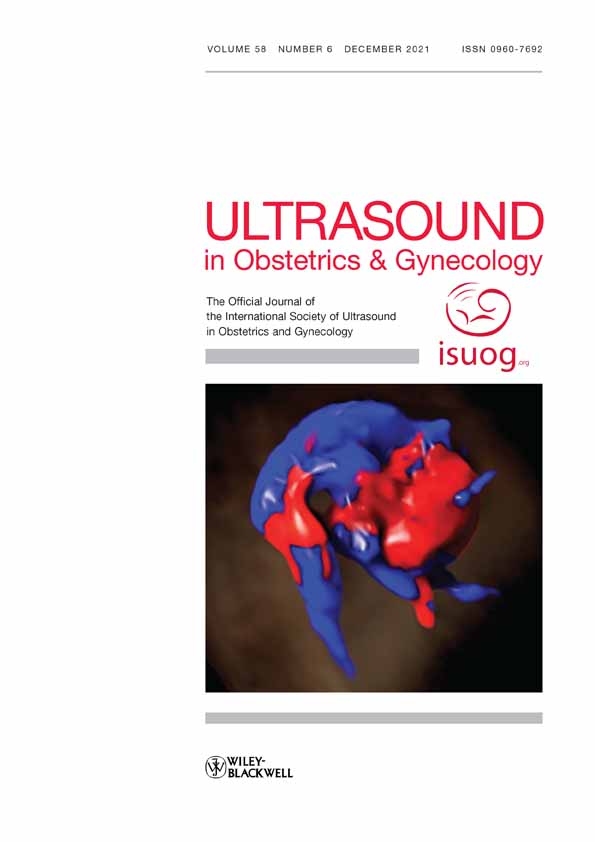
The mean lesion length, thickness and transverse diameter measurements based on TVS and PSM are displayed in Table 1. The mean difference in measurements between TVS and PSM was 0.90 mm (95% CI, 0.85–0.95 mm; P < 0.0001) for lesion length, 1.03 mm (95% CI, 0.98–1.09 mm; P = 0.20) for lesion thickness and 0.84 mm (95% CI, 0.79–0.89 mm; P < 0.0001) for transverse diameter (all calculations based on antilog-transformed data). From a clinical perspective, the differences were small for measurements of all three lesion dimensions and were below the a-priori set clinically acceptable difference of ± 10 mm. A Bland–Altman plot on a logarithmic scale showed good agreement and no systematic differences between TVS and PSM for lesion length measurements (Figure 4a). There was perfect agreement between TVS and PSM for measurements of lesion length in 10 (6%) women, while TVS demonstrated lower measurements than did PSM in 101 (61%) women and higher measurements in 55 (33%) women. However, the Bland–Altman plots for lesion thickness and transverse diameter measurements showed a greater spread of differences between the measurement methods (Figure 4b,c).
Table 1. Demographic characteristics and symptoms in 166 women with rectosigmoid deep endometriosis (DE) scheduled for surgery Characteristic Value Age (years) 35.7 ± 6.2 BMI (kg/m2) 24.7 ± 4.3 Rectosigmoid lesion dimensions Transvaginal sonographic measurement Length (mm) 29.6 ± 13.6 Thickness (mm) 11.4 ± 4.2 Transverse diameter (mm) 14.7 ± 5.6 Postsurgical measurement of fresh specimen Length (mm) 33.9 ± 18.5 Thickness (mm) 11.0 ± 4.1 Transverse diameter (mm) 17.9 ± 7.0 Symptoms Dysmenorrhea 163 (98.2) Dyschezia 141 (84.9) Dyspareunia* 114/164 (69.5) Diarrhea 70 (42.2) Constipation 63 (38.0) Dysuria 22 (13.3) Rectal bleeding 21 (12.7) Previous surgery for endometriosis None 83 (50.0) One 60 (36.1) More than one 23 (13.9) Type of surgical procedure† Discoid resection 46 (27.7) Segmental resection 123 (74.1) rASRM stage I 0 (0) II 33 (19.9) III 39 (23.5) IV 94 (56.6) Enzian classification of rectosigmoid DE C1 (rectosigmoid lesions < 1 cm) 0 (0.0) C2 (rectosigmoid lesions 1–3 cm) 60 (36.1) C3 (rectosigmoid lesions > 3 cm) 106 (63.9) Data are given as mean ± SD, n (%) or n/N (%). * Data missing for two women and three women had abstained from intercourse for many years due to pain. † Both procedures were performed in three women. BMI, body mass index; rASRM, revised American Society of Reproductive Medicine. Bland–Altman plots showing agreement between transvaginal sonography (TVS) and postsurgical measurement (PSM) for rectosigmoid deep endometriosis lesion length (a), thickness (b) and transverse diameter (c) measurements. All plots are on a logarithmic scale (ln). The mean (
Bland–Altman plots showing agreement between transvaginal sonography (TVS) and postsurgical measurement (PSM) for rectosigmoid deep endometriosis lesion length (a), thickness (b) and transverse diameter (c) measurements. All plots are on a logarithmic scale (ln). The mean ( ) and 95% limits of agreement (LoA) (
) and 95% limits of agreement (LoA) ( ) with 95% CI (
) with 95% CI ( ) are displayed. The plots show that TVS measurements were on average lower than PSMs for lesion length and transverse diameter, while they were higher for lesion thickness. There was a wider spread of differences between the two methods for lesion thickness and transverse diameter measurements than for lesion length measurements. The 95% LoA for all three lesion dimensions were within a clinically acceptable range.
) are displayed. The plots show that TVS measurements were on average lower than PSMs for lesion length and transverse diameter, while they were higher for lesion thickness. There was a wider spread of differences between the two methods for lesion thickness and transverse diameter measurements than for lesion length measurements. The 95% LoA for all three lesion dimensions were within a clinically acceptable range.
The 95% LoA were 0.44 (95% CI, 0.41–0.49) mm to 1.82 (95% CI, 1.67–1.99) mm for lesion length, 0.53 (95% CI, 0.48–0.58) mm to 2.01 (95% CI, 1.84–2.20) mm for lesion thickness and 0.37 (95% CI, 0.33–0.41) mm to 1.90 (95% CI, 1.70–2.12) mm for transverse diameter measurements (all calculations based on antilog-transformed data). The LoA were within the clinically acceptable difference of ± 10 mm for all dimensions. There was good reliability and correlation between TVS and PSM for measurements of lesion length, with ICC of 0.82 (95% CI, 0.75–0.87) and Pearson's correlation coefficient of 0.72 (95% CI, 0.62–0.80). There was moderate-to-good reliability and correlation for lesion thickness measurements, with ICC of 0.76 (95% CI, 0.67–0.82) and Pearson's correlation coefficient of 0.61 (95% CI, 0.51–0.70), and poor-to-moderate reliability and correlation for transverse diameter measurements, with ICC of 0.58 (95% CI, 0.39–0.71) and Pearson's correlation coefficient of 0.46 (95% CI, 0.33–0.58). Regression analysis did not identify any variables that could explain the differences in measurements between the methods.
DISCUSSIONThe present study is the first multicenter study conducted in a tertiary referral setting in which detailed analysis of pre- and postoperative rectosigmoid DE lesion measurements, based on the IDEA consensus statement, was performed. We found that TVS had good reliability for measuring the length of rectosigmoid DE lesions, moderate-to-good reliability for measuring lesion thickness and poor-to-moderate reliability for measuring transverse diameter, as compared with PSM of fresh bowel specimens. The results highlight the value of using TVS for measuring lesion length and examining women with rectosigmoid DE systematically prior to surgery11, 13.
However, this study has some limitations. First, variation in how the bowel was cut prior to PSM could explain the moderate-to-good reliability for lesion thickness measurements and poor-to-moderate reliability for transverse diameter measurements. Any errors in measuring lesion length and thickness would have an additive effect on transverse diameter measurements. Difficulty in identifying infiltration depth on TVS30 could have contributed to increased variability for lesion thickness and transverse diameter measurements. We assumed that the true measurements of the three lesion dimensions were obtained by PSM. PSM was performed using a manual ruler, which is a limitation. A histological control was not possible, as the specimen was already cut and as formaldehyde fixation leads to specimen shrinkage, which would distort the bowel specimen. TVS and PSM were performed by the same observer since the gynecological surgeons also perform sonography in our tertiary referral center settings. However, there was variability in measurement differences between the methods for all three lesion dimensions, which provides evidence against the presence of bias due to lack of blinding. In addition, we did not use bowel preparation prior to TVS in this study. However, there is no consensus on the use of bowel preparation to enhance TVS evaluation of rectosigmoid DE lesions31-33. Bowel preparation is more invasive and requires more resources, particularly outside a study setting. This study reflects clinical practice, as TVS with prior bowel preparation is not routine in any of the three tertiary referral centers. Lesion shape, such as regular, comet sign or Indian head-dress sign, as suggested by the IDEA consensus13, was not described, as this was beyond the scope of this study. Thus, a limitation is that we did not subclassify lesion shape to investigate whether TVS measurements of regular shaped lesions corresponded better to PSM than did TVS measurements of lesions with prominent spikes. It would be interesting to study this further. However, in the surgical management of rectosigmoid DE, lesion-to-anal-verge distance and lesion size, rather than lesion shape, are seen as important factors in planning surgery1, 17, 34. Furthermore, measuring the three dimensions of rectosigmoid DE lesions may be confounded by inter- and intraobserver variability. A kappa index calculation was not performed between the four observers in this study, as it was a multicenter study recruiting women from three different countries, which represents a limitation. Egekvist et al.35 found intra- and interobserver variability for TVS measurements of lesion length, with a coefficient of repeatability of 11–14 mm, compared with 3–6 mm for lesion thickness and 5–9 mm for transverse diameter measurements. However, the IDEA consensus was not used. Contrarily, Bean et al.36 recently reported good interobserver variability (ICC, 0.88 (95% CI, 0.72–0.95)) and excellent intraobserver variability (ICC, 0.93 (95% CI, 0.82–0.97) and ICC, 0.96 (95% CI, 0.90–0.98)) of bowel lesion measurements on TVS. In a single-center study, Di Giovanni et al.20 found no statistically significant difference in the measurements of any of the three dimensions of rectosigmoid DE lesions when comparing TVS and PSM. The IDEA consensus was not used in their study. The strength of this study is that we performed an additional analysis investigating agreement and between-method differences26, 37. Furthermore, the international multicenter study design increases the generalizability of the results to other tertiary referral units around the world.
In conclusion, our results show that TVS is a reliable tool for measuring rectosigmoid DE lesion length. Systematic preoperative TVS mapping, including lesion-length measurement, is vital before embarking on advanced surgical treatment and is likely to improve the counseling process of women and optimize surgical planning.
ACKNOWLEDGMENTSWe thank the Norwegian Endometriosis Association for their input and support of this study. We thank Johann Baptist Dormagen at the Division of Radiology and Nuclear Medicine, Oslo University Hospital, Oslo, Norway, for his comments on and input in the write-up of the article.
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
REFERENCES
1 Working group of ESGE, ESHRE and WES, Keckstein J, Becker CM, Canis M, Feki A, Grimbizis GF, Hummelshoj L, Nisolle M, Roman H, Saridogan E, Tanos V, Tomassetti C, Ulrich UA, Vermeulen N, De Wilde RL. Recommendations for the surgical treatment of endometriosis. Part 2: deep endometriosis. Hum Reprod Open 2020; 2020: hoaa002. 2Hudelist G, Tammaa A, Aas-Eng MK, Kirchner L, Fritzer N, Nemeth Z, Lamche M. Outcome of sonography-based minimally invasive surgery for deep infiltrating endometriosis of the ureter and urinary bladder: a retrospective cohort study. Acta Obstet Gynecol Scand 2018; 97: 277– 284. 3Hudelist G, Aas-Eng MK, Birsan T, Berger F, Sevelda U, Kirchner L, Salama M, Dauser B. Pain and fertility outcomes of nerve-sparing, full-thickness disk or segmental bowel resection for deep infiltrating endometriosis-A prospective cohort study. Acta Obstet Gynecol Scand 2018; 97: 1438– 1446. 4Roman H. A national snapshot of the surgical management of deep infiltrating endometriosis of the rectum and colon in France in 2015: A multicenter series of 1135 cases. J Gynecol Obstet Hum Reprod 2017; 46: 159– 165. 5Balla A, Quaresima S, Subiela JD, Shalaby M, Petrella G, Sileri P. Outcomes after rectosigmoid resection for endometriosis: a systematic literature review. Int J Colorectal Dis 2018; 33: 835– 847. 6Donnez O, Roman H. Choosing the right surgical technique for deep endometriosis: shaving, disc excision, or bowel resection? Fertil Steril 2017; 108: 931– 942. 7Roman H, Vassilieff M, Tuech JJ, Huet E, Savoye G, Marpeau L, Puscasiu L. Postoperative digestive function after radical versus conservative surgical philosophy for deep endometriosis infiltrating the rectum. Fertil Steril 2013; 99: 1695– 1704. 8Roman H, Tuech JJ, Huet E, Bridoux V, Khalil H, Hennetier C, Bubenheim M, Branduse LA. Excision versus colorectal resection in deep endometriosis infiltrating the rectum: 5-year follow-up of patients enrolled in a randomized controlled trial. Hum Reprod 2019; 34: 2362– 2371. 9Hudelist G, English J, Thomas AE, Tinelli A, Singer CF, Keckstein J. Diagnostic accuracy of transvaginal ultrasound for non-invasive diagnosis of bowel endometriosis: systematic review and meta-analysis. Ultrasound Obstet Gynecol 2011; 37: 257– 263. 10Aas-Eng MK, Montanari E, Lieng M, Keckstein J, Hudelist G. Transvaginal Sonographic Imaging and Associated Techniques for Diagnosis of Ovarian, Deep Endometriosis, and Adenomyosis: A Comprehensive Review. Semin Reprod Med 2020; 38: 216– 226. 11Aas-Eng MK, Dauser B, Lieng M, Diep LM, Leonardi M, Condous G, Hudelist G. Transvaginal sonography accurately predicts lesion-to-anal-verge distance in women with deep endometriosis of the rectosigmoid. Ultrasound Obstet Gynecol 2020; 56: 766– 772. 12Vanhie A, Meuleman C, Tomassetti C, Timmerman D, D'Hoore A, Wolthuis A, Van Cleynenbreugel B, Dancet E, Van den Broeck U, Tsaltas J, Renner SP, Ebert AD, Carmona F, Abbott J, Stepniewska A, Taylor H, Saridogan E, Mueller M, Keckstein J, Pluchino N, Janik G, Zupi E, Minelli L, Cooper M, Dunselman G, Koh C, Abrao M, Chapron C, D'Hooghe T. Consensus on Recording Deep Endometriosis Surgery: the CORDES statement. Hum Reprod 2016; 31: 1219– 1223. 13Guerriero S, Condous G, van den Bosch T, Valentin L, Leone FP, Van Schoubroeck D, Exacoustos C, Installe AJ, Martins WP, Abrao MS, Hudelist G, Bazot M, Alcazar JL, Goncalves MO, Pascual MA, Ajossa S, Savelli L, Dunham R, Reid S, Menakaya U, Bourne T, Ferrero S, Leon M, Bignardi T, Holland T, Jurkovic D, Benacerraf B, Osuga Y, Somigliana E, Timmerman D. Systematic approach to sonographic evaluation of the pelvis in women with suspected endometriosis, including terms, definitions and measurements: a consensus opinion from the International Deep Endometriosis Analysis (IDEA) group. Ultrasound Obstet Gynecol 2016; 48: 318– 332. 14Keckstein J, Hudelist G. Classification of deep endometriosis (DE) including bowel endometriosis: From r-ASRM to #Enzian-classification. Best Pract Res Clin Obstet Gynaecol 2021; 71: 27– 37. 15Voscopoulos C, Lema M. When does acute pain become chronic? Br J Anaesth 2010; 105: i69– 85. 16Leonardi M, Singh SS, Murji A, Satkunaratnam A, Atri M, Reid S, Condous G. Deep Endometriosis: A Diagnostic Dilemma With Significant Surgical Consequences. J Obstet Gynaecol Can 2018; 40: 1198– 1203. 17Abrao MS, Petraglia F, Falcone T, Keckstein J, Osuga Y, Chapron C. Deep endometriosis infiltrating the recto-sigmoid: critical factors to consider before management. Hum Reprod Update 2015; 21: 329– 339. 18Roman H, Bubenheim M, Huet E, Bridoux V, Zacharopoulou C, Darai E, Collinet P, Tuech JJ. Conservative surgery versus colorectal resection in deep endometriosis infiltrating the rectum: a randomized trial. Hum Reprod 2018; 33: 47– 57. 19Bokor A, Hudelist G, Dobo N, Dauser B, Farella M, Brubel R, Tuech JJ, Roman H. Low anterior resection syndrome following different surgical approaches for low rectal endometriosis: A retrospective multicenter study. Acta Obstet Gynecol Scand 2021; 100: 860– 867. 20Di Giovanni A, Casarella L, Coppola M, Iuzzolino D, Rasile M, Malzoni M. Combined Transvaginal/Transabdominal Pelvic Ultrasonography Accurately Predicts the 3 Dimensions of Deep Infiltrating Bowel Endometriosis Measured after Surgery: A Prospective Study in a Specialized Center. J Minim Invasive Gynecol 2018; 25: 1231– 1240. 21Goncalves MO, de Mattos LA, Abrao MS. Rectum, Rectosigmoid, and Sigmoid Endometriosis. In How to perform ultrasonography in endometriosis ( 1st edn), S Guerriero, G Condous, JL Alcázar (eds). Springer International Publishing AG: Cham., 2018; 103– 120. 22Woods RJ, Heriot AG, Chen FC. Anterior rectal wall excision for endometriosis using the circular stapler. ANZ J Surg 2003; 73: 647– 648. 23Anaf V, El Nakadi I, Simon P, Van de Stadt J, Fayt I, Simonart T, Noel JC. Preferential infiltration of large bowel endometriosis along the nerves of the colon. Hum Reprod 2004; 19: 996– 1002. 24Haas D, Wurm P, Shamiyeh A, Shebl O, Chvatal R, Oppelt P. Efficacy of the revised Enzian classification: a retrospective analysis. Does the revised Enzian classification solve the problem of duplicate classification in rASRM and Enzian? Arch Gynecol Obstet 2013; 287: 941– 945. 25
留言 (0)