
記住我

Atypical teratoid/rhabdoid tumours (AT/RT) are highly malignant neoplasms of the central nervous system (CNS), which predominantly occur in infants, but may also be encountered in older patients. Histopathologically, AT/RT are characterised by the presence of rhabdoid tumour cells and loss of nuclear SMARCB1/INI1 protein expression.1, 2 Using DNA methylation profiling and gene expression analysis, three distinct molecular subgroups of AT/RT can be distinguished, that is, ATRT-TYR, -SHH and -MYC.3, 4 Recently, low-grade diffusely infiltrative tumour with SMARCB1/INI1-deficiency (CNS LGDIT-INI1) has been proposed as a new entity.5 CNS LGDIT-INI1 represents a low-grade tumour composed of inconspicuous SMARCB1-deficient tumour cells diffusely infiltrating the brain. Progression of CNS LGDIT-INI1 to AT/RT has been reported,5, 6 but the molecular relationship between CNS LGDIT-INI1 and AT/RT remains uncertain. We here report the first case of a child with a CNS LGDIT-INI1 that featured a high-grade AT/RT component at the time of initial surgery.
The 14-year-old boy presented as an acute emergency with clinical signs of increased brain pressure, anisocoria and a possible seizure. He was the only surviving child of a triplet pregnancy, naturally conceived after induction of ovulation. Infants from a previous triplet pregnancy did not survive due to complications from prematurity. Further medical history and family history were unremarkable.
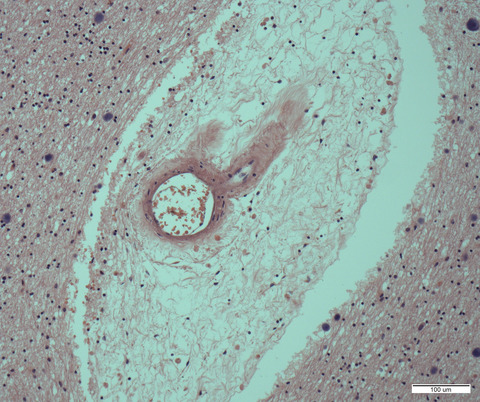
Magnetic resonance imaging showed a 5.7 × 3.0 × 3.7 cm large, right-sided parieto-occipital mass with cystic, solid and calcified areas (Figure 1A). Gross total resection could be achieved. On histopathological examination, two dissimilar and widely separated morphological components could be distinguished. The first component displayed calcification and a fibrillary matrix with scantly distributed unremarkable cells with oval nuclei and occasional interspersed larger ganglioid cells (Area 1, Figure 1B). The second component was highly cellular and was composed of large rhabdoid tumour cells with prominent nucleoli and/or eosinophilic cytoplasm (Area 2, Figure 1C).
 Radiological, histopathological and epigenetic analysis. (A) Preoperative MRI demonstrating a parieto-occipital tumour. The scale bar is 3 cm. (B–C) Histomorphology revealed two distinct components, annotated as Areas 1 (B) and 2 (C). Arrows show interspersed ganglioid cells of Area 1. The scale bar is 50 μm. (D–G) Area 1 displayed strong immunohistochemical positivity for GFAP (D) and synaptophysin (E). Only very few nuclei stained for positive for Ki67 (F). Sparsely distributed larger cell nuclei showed retained INI-1 expression (G). (H–K) Area 2 showed negativity for GFAP (H), synaptophysin (I) and a considerably elevated Ki67 nuclear labelling (J) as well as extended loss of nuclear INI-1 (K). The scale bar is 50 μm in (D)–(K). (L) The Ki67 proliferation index was significantly higher in Area 2 compared with Area 1. Cell nuclei of six regions corresponding to the ROIs of Figure 2 were manually counted. Welch's t test, **p = 0.0053. (M) INI1-positive cells were more frequently found in Area 1 compared with Area 2. Cell nuclei of six regions corresponding to the ROIs of Figure 2 were manually counted. Welch's t test, *p = 0.0365. (N–O) Copy number profiles of both tumour areas indicated homozygous SMARCB1/INI1 deletion. (P–Q) UMAP analysis including a reference set of brain tumours (P) (GSE90496,8) as well as extracranial malignant rhabdoid tumours (Q) (eMRT, GSE123601,9) showed affiliation of both tumour components to the group of ATRT-MYC and a molecularly similar subset of eMRTs
Radiological, histopathological and epigenetic analysis. (A) Preoperative MRI demonstrating a parieto-occipital tumour. The scale bar is 3 cm. (B–C) Histomorphology revealed two distinct components, annotated as Areas 1 (B) and 2 (C). Arrows show interspersed ganglioid cells of Area 1. The scale bar is 50 μm. (D–G) Area 1 displayed strong immunohistochemical positivity for GFAP (D) and synaptophysin (E). Only very few nuclei stained for positive for Ki67 (F). Sparsely distributed larger cell nuclei showed retained INI-1 expression (G). (H–K) Area 2 showed negativity for GFAP (H), synaptophysin (I) and a considerably elevated Ki67 nuclear labelling (J) as well as extended loss of nuclear INI-1 (K). The scale bar is 50 μm in (D)–(K). (L) The Ki67 proliferation index was significantly higher in Area 2 compared with Area 1. Cell nuclei of six regions corresponding to the ROIs of Figure 2 were manually counted. Welch's t test, **p = 0.0053. (M) INI1-positive cells were more frequently found in Area 1 compared with Area 2. Cell nuclei of six regions corresponding to the ROIs of Figure 2 were manually counted. Welch's t test, *p = 0.0365. (N–O) Copy number profiles of both tumour areas indicated homozygous SMARCB1/INI1 deletion. (P–Q) UMAP analysis including a reference set of brain tumours (P) (GSE90496,8) as well as extracranial malignant rhabdoid tumours (Q) (eMRT, GSE123601,9) showed affiliation of both tumour components to the group of ATRT-MYC and a molecularly similar subset of eMRTs
Immunohistochemistry of Area 1 showed strong staining for GFAP (Figure 1D) and synaptophysin (Figure 1E). The Ki67 proliferation index was approximately 1% (Figure 1F,L). Staining for SMARCB1/INI1 further demonstrated a diffuse growth pattern of immunonegative tumour cells but retained SMARCB1/INI1 staining mainly in the ganglioid cells (Figure 1G,M, arrows). In contrast, negative staining for GFAP (Figure 1H) and synaptophysin (Figure 1I) was observed in Area 2. Here, Ki67-staining revealed a substantially higher proliferation index of about 20% (Figure 1J,L) and, aside from blood vessels, nearly complete loss of nuclear SMARCB1/INI1 expression (Figure 1K,M).
DNA was extracted from both tumour components and subjected to DNA methylation profiling using the Illumina EPIC BeadChip array. Using the brain tumour methylation classifier (v11b4),8 both components matched with ATRT-MYC (calibrated scores: 0.99). The copy number profiles revealed similar characteristics with homozygous SMARCB1 deletions in both components (Figure 1N,O). UMAP analysis including a reference set of brain tumours8 confirmed the close epigenetic similarity of both tumour components with ATRT-MYC (Figure 1P,Q). DNA panel sequencing did not reveal relevant mutations in either area (Table S1). MLPA detected compound heterozygosity for two different large deletions encompassing all exons of SMARCB1 in tumour-derived DNA. No SMARCB1 mutation was found in lymphocyte-derived DNA.
We next used NanoString GeoMx Digital Spatial Profiler (DSP) technology to measure area-specific whole transcriptome RNA expression (Figure 2A). Hierarchical clustering based on RNA counts of all regions of interest (ROIs, n = 3 for each area) showed clustering according to morphology (Figures 2B and S1A). In line with the histomorphological and immunohistochemical characteristics, we found significant upregulation of INI1 (Figure 2C) in Area 1 as well as strongly elevated expression levels of multiple cell cycle genes in Area 2 (Figure 2D). Moreover, we found strongly increased expression of markers of neuronal, oligodendroglial and astrocytic differentiation in Area 1 (Figures 2E–G and S1B,C; Tables S2 and S3). To investigate Areas 1 and 2 for functional transcriptional differences, we performed gene set enrichment analysis (Figure 2H,I). The most significantly enriched gene sets of two databases (Reactome and PID) in Area 2 primarily reflected major changes in post-transcriptional processes (Figure 2H and Table S4) and, interestingly, activation of the MYC pathway (Figure 2I and Table S5). The robust changes in ribosomal function were confirmed using an additional database (KEGG, Figure S2 and Table S6). In order to exclude the possibility that these findings were solely due to residual nontumorous tissue contamination of Area 1, we additionally performed normalisation of RNA expression counts to the number of INI1-negative cells (Figure 2J) for all respective genes of the gene sets. RNA expression counts per INI1-negative tumour cells were significantly higher in Area 2 when compared with Area 1 (Figure 2K,L). Thus, transcriptional differences in nearly all of the investigated genes could not be explained by varying cell type compositions across ROIs. More details concerning the applied methods can be found in the supporting information.
 Spatial RNA expression analysis. (A) NanoString GeoMx DSP technology was used to measure RNA expression in both tumour areas (left column) by manually assigning regions of interest (ROIs, middle column). Morphological markers used were DNA (blue), Ki67 (red), Vimentin (yellow) and CD34 (green). CD34 positive cells corresponding to blood vessels were excluded from the analysis via segmentation technique (right column). Three independent ROIs per area were determined for analysis. Scale bar is 250 μm. (B) Hierarchical clustering of RNA expression data demonstrated primary clustering of all ROIs according to their respective morphology. (C) Expression of INI1 was significantly elevated in Area 1, reflective of immunostaining characteristics (Figure 1G,K). (D) Expression of diverse cell cycle genes was significantly elevated in Area 2, reflective of elevated Ki67 immunostaining (Figure 1F,J). (E–G) Area 1 demonstrated consistently increased expression of multiple neuronal (E), oligodendroglial (F) and astrocytic (G) markers,7 suggesting the presence of residual brain tissue of varying cell types. For (C)–(G), each gene was analysed with unpaired t test. Adjusted p values after multiple testing correction (Holm–Šidák method) within each graph are shown: *p p p p p p S4 and S5. (J) Cell counts of all ROIs per tumour area were obtained from the segment properties reported by the GeoMx DSP Analysis Suite. Numbers of INI1-positive and negative cells were calculated using the percentages demonstrated in Figure 1M. (K, L) RNA counts of genes of the significant gene sets after GSEA (H, I) were reinvestigated after normalisation to the number of INI1-negative cells in both tumour areas. The x-axis demonstrates the genes included in the respective gene set in the order of their appearance in the pre-ranked gene list used for GSEA. The y-axis demonstrates RNA counts (after background subtraction) divided by the number of INI1-negative cells (J) in all ROIs of the two tumour areas. Statistical testing confirmed persistent significant differential expression between Areas 1 and 2. ***p
Spatial RNA expression analysis. (A) NanoString GeoMx DSP technology was used to measure RNA expression in both tumour areas (left column) by manually assigning regions of interest (ROIs, middle column). Morphological markers used were DNA (blue), Ki67 (red), Vimentin (yellow) and CD34 (green). CD34 positive cells corresponding to blood vessels were excluded from the analysis via segmentation technique (right column). Three independent ROIs per area were determined for analysis. Scale bar is 250 μm. (B) Hierarchical clustering of RNA expression data demonstrated primary clustering of all ROIs according to their respective morphology. (C) Expression of INI1 was significantly elevated in Area 1, reflective of immunostaining characteristics (Figure 1G,K). (D) Expression of diverse cell cycle genes was significantly elevated in Area 2, reflective of elevated Ki67 immunostaining (Figure 1F,J). (E–G) Area 1 demonstrated consistently increased expression of multiple neuronal (E), oligodendroglial (F) and astrocytic (G) markers,7 suggesting the presence of residual brain tissue of varying cell types. For (C)–(G), each gene was analysed with unpaired t test. Adjusted p values after multiple testing correction (Holm–Šidák method) within each graph are shown: *p p p p p p S4 and S5. (J) Cell counts of all ROIs per tumour area were obtained from the segment properties reported by the GeoMx DSP Analysis Suite. Numbers of INI1-positive and negative cells were calculated using the percentages demonstrated in Figure 1M. (K, L) RNA counts of genes of the significant gene sets after GSEA (H, I) were reinvestigated after normalisation to the number of INI1-negative cells in both tumour areas. The x-axis demonstrates the genes included in the respective gene set in the order of their appearance in the pre-ranked gene list used for GSEA. The y-axis demonstrates RNA counts (after background subtraction) divided by the number of INI1-negative cells (J) in all ROIs of the two tumour areas. Statistical testing confirmed persistent significant differential expression between Areas 1 and 2. ***p
Histopathology, immunohistochemical staining profiles and molecular findings resulted in a diagnosis of CNS LGDIT-INI1 featuring a high-grade AT/RT component, and the case was signed out as AT/RT (Grade IV WHO). The patient was treated with systemic chemotherapy, intraventricular methotrexate and local intensity-modulated radiotherapy with photons (54 Gy) according to the EURHAB registry protocol. He made a good clinical and neurological recovery, returned back to school and remained in complete remission on magnetic resonance imaging at last follow-up, over 12 months after surgery.
The simultaneous presence of a low-grade and high-grade component on initial presentation has not yet been described in CNS LGDIT-INI1 and is compatible with the concept of potential malignant progression of these tumours. However, the possibility of a high-grade tumour displaying well-differentiated regions with low-grade features cannot be excluded. Importantly, methylation profiles of the low- and the high-grade component of the presented tumour yielded high similarity with ATRT-MYC. In two previously published cases of similar INI1-deficient tumours, both the low-grade primary as well as the high-grade recurrent lesions demonstrated epigenetic similarity with ATRT-MYC.5, 6 Proliferative indices previously reported in three of such high-grade recurrent INI1-deficient tumours amounted to 53.7%, 18.2% and >20%.5, 6 Appositely, the herein presented tumour demonstrated a proliferation index of about 20%. In contrast, AT/RTs commonly display rather high Ki67 indices (mean 63.9%).10 It remains to be determined in a larger series, if CNS LGDIT-INI1 form a distinct subgroup or blend with AT/RT of the MYC subgroup.
Spatial RNA analyses reflected regional histomorphological features. The consistent detection of diverse glioneuronal markers in Area 1 most likely suggests the presence of residues of nontumorous infiltrated brain tissue (e.g., INI1-positive cells of Area 1) and underlines the concept of diffuse infiltrative behaviour of CNS LGDIT-INI1. Moreover, our results hint towards potential biological mechanisms involved in the formation of high-grade tumour areas with increased translational activity and proliferation. Intriguingly, the most significant enrichment found in the PID database related to MYC pathway activation, which is potentially linked to the affiliation of CNS LGDIT-INI1 to the ATRT-MYC subgroup. Although spatial RNA expression analysis demonstrated robust accordance with histomorphological features and therefore displayed its potential as a strong method for spatial tissue analysis, it is important to recognise the limitations of this approach with respect to the influence of varying cell type compositions (e.g., tumour vs nontumour) on transcriptional differences across ROIs. Although we address this by approximating the number of tumour cells (i.e., INI1-negative cells) of individual ROIs, presently this issue can only be adequately accounted for via proper segmentation of ROIs or single cell RNA-sequencing. Unfortunately, fresh-frozen material of this tumour was not available.
In conclusion, despite low proliferative activity and benign histopathological features, CNS LGDIT-INI1 shows epigenetic similarities to AT/RT and growing evidence corroborates its potential for malignant progression with development of a high-grade rhabdoid component. Close follow-up of patients harbouring CNS LGDIT-INI1 is warranted.
ACKNOWLEDGEMENTSWe thank Anthony Zucca, Stephan Hesse and Alison Vanschoiack (NanoString) for support in data acquisition and analysis. We thank Celina Soltwedel, Carolina Janko, Karin Gehlken, Ulrike Rumpf, Dagmar Drexler, Nicole Bernhardt, Helena Zinn and Prof Dr Ulrich Schüller (Hamburg) for excellent technical support. J.N. was supported by the Deutsche Forschungsgemeinschaft (DFG, Emmy Noether programme). M.D. was supported by the Erich und Gertrud Roggenbuck-Stiftung.
CONFLICT OF INTERESTThe authors have no competing interests to declare.
ETHICS STATEMENTStudy approval was obtained from the local ethics committee of the Hamburg State Chamber of Physicians. The patient and/or guardian gave their informed consent for scientific use of the data.
AUTHOR CONTRIBUTIONSM.D. and J.N. conceived the study and drafted the manuscript. All authors acquired and analysed data, provided critical feedback, helped shape the manuscript and approved its final version.
留言 (0)