
記住我

The term ‘lower urinary tract obstruction’ (LUTO) covers a heterogeneous group of anatomical anomalies caused by an obstruction of the urethra1. The most common cause of LUTO is the presence of posterior urethral valves (PUV), which has a prevalence of 1–2 per 10 000 male live births2, 3. LUTO can also be caused by a complete infravesical obstruction obliterating the most distal portion of the prostatic urethra, known as urethral atresia (UA), which represents the most severe form of LUTO3, 4. These two subtypes of LUTO have different prognosis and management. In patients with PUV (Figure 1), physiological micturition can be restored by endoscopic valve ablation, which can be performed either pre- or postnatally5. Alternatively, a vesicoamniotic shunt can be placed prenatally to restore amniotic fluid and prevent lung hypoplasia. In contrast, UA (Figure 2) has a poor prognosis, is not amenable to prenatal surgical correction and has a high risk of intrauterine death. Information on UA is scarce regarding postnatal outcome, as liveborn infants are rarely reported in the literature6. The differential diagnosis between these two conditions prenatally is very subtle and a definitive diagnosis can be reached only after birth or at postmortem examination. So far, neither prenatal ultrasound nor urine biochemistry have been able to differentiate accurately between these two subtypes of LUTO7.

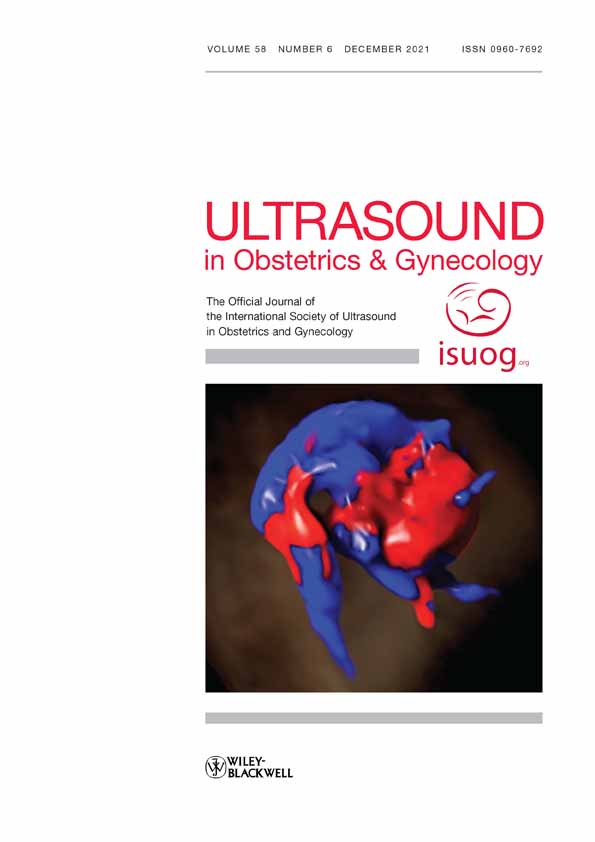
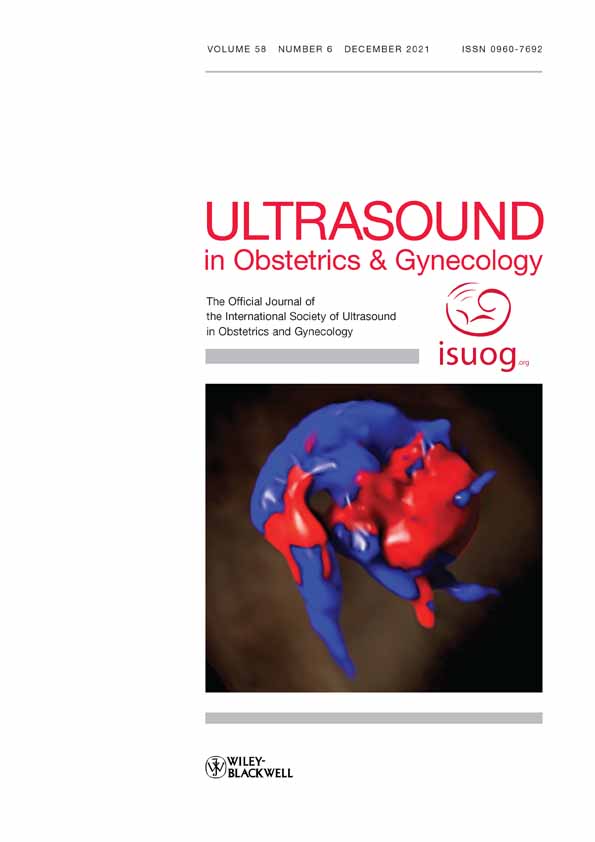
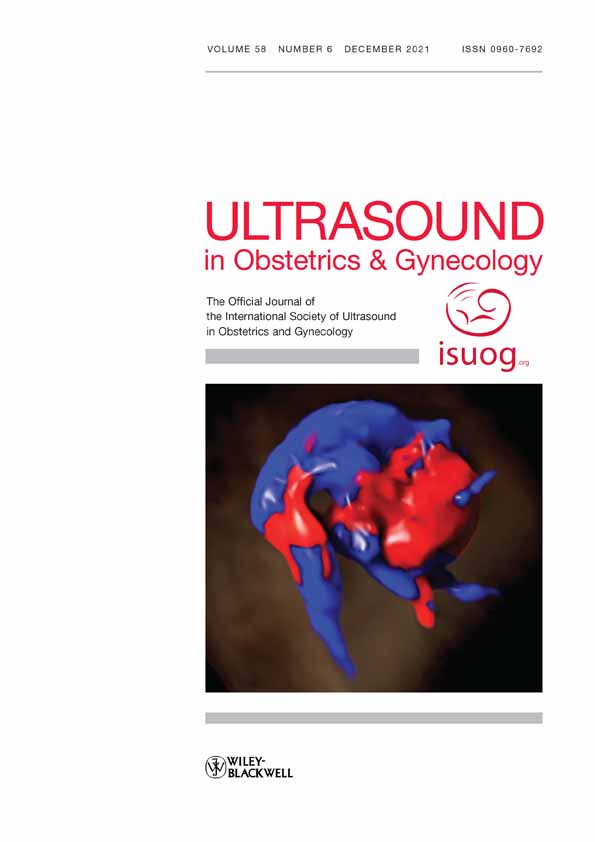
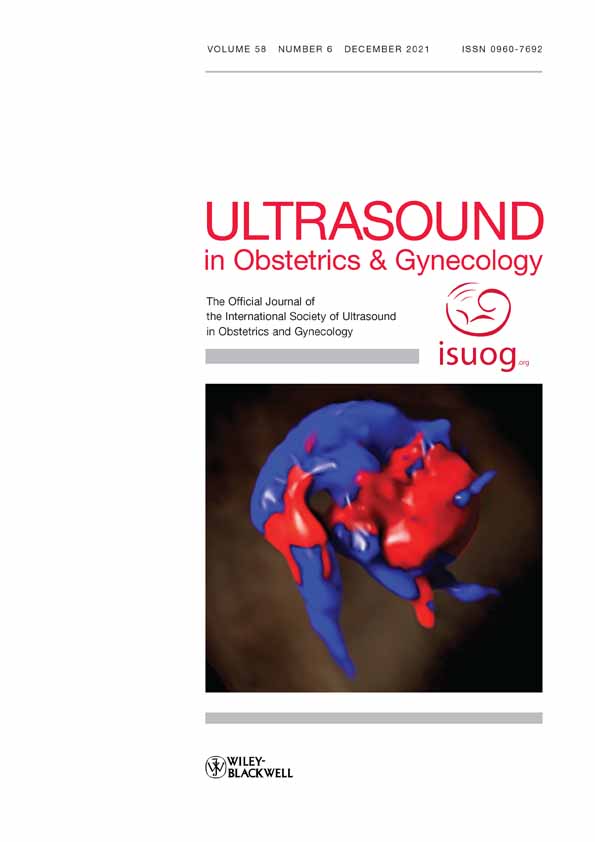
Postmortem examination (a,b) and ultrasound images (c,d) in a 20 + 6-week fetus with posterior urethral valves, tortuous ureters and multicystic renal dysplasia. RK, right kidney.

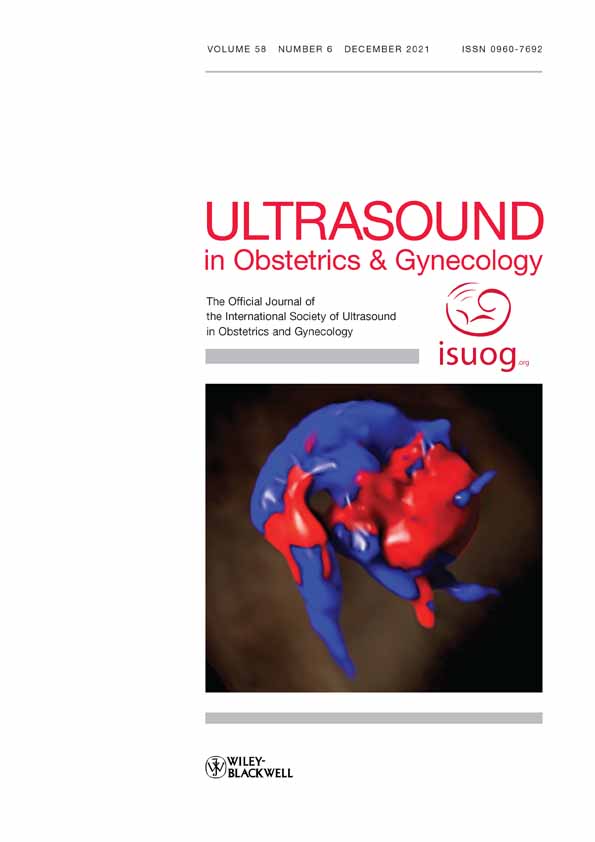
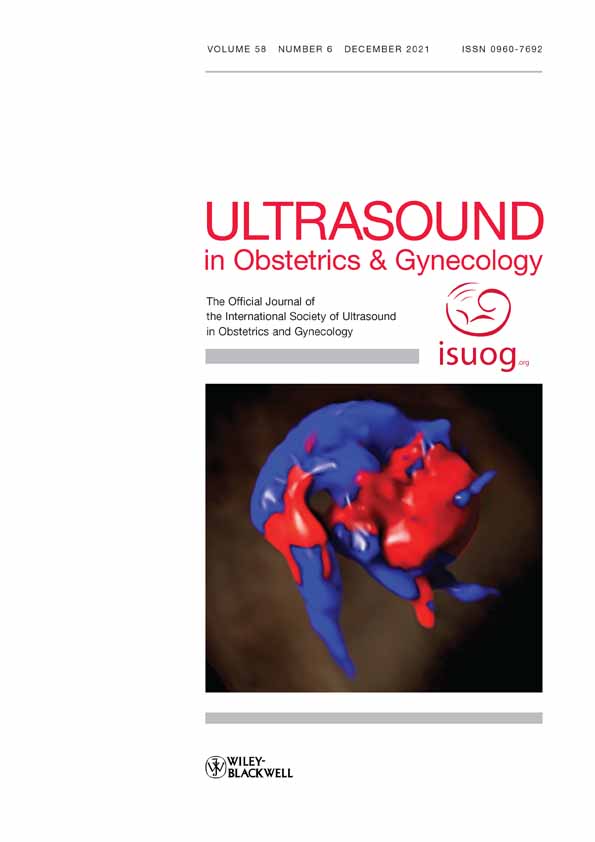
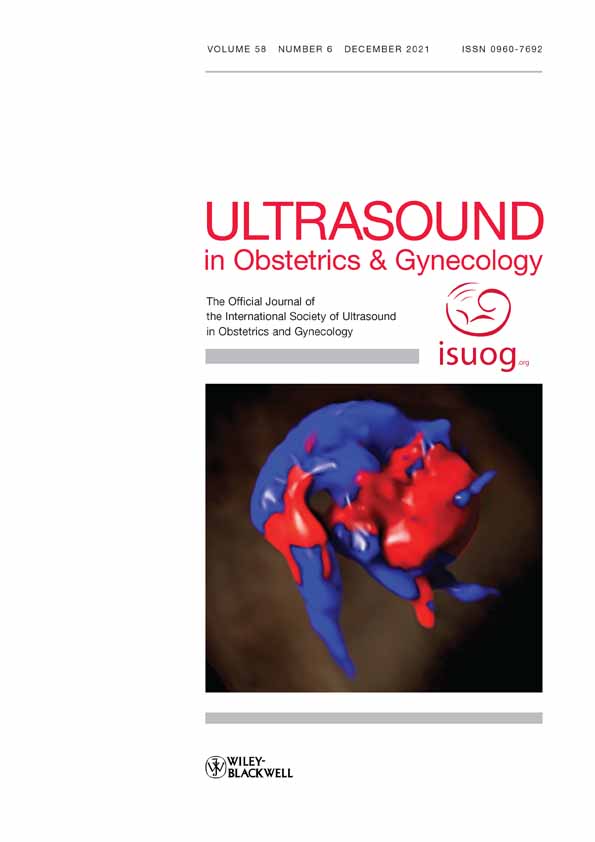
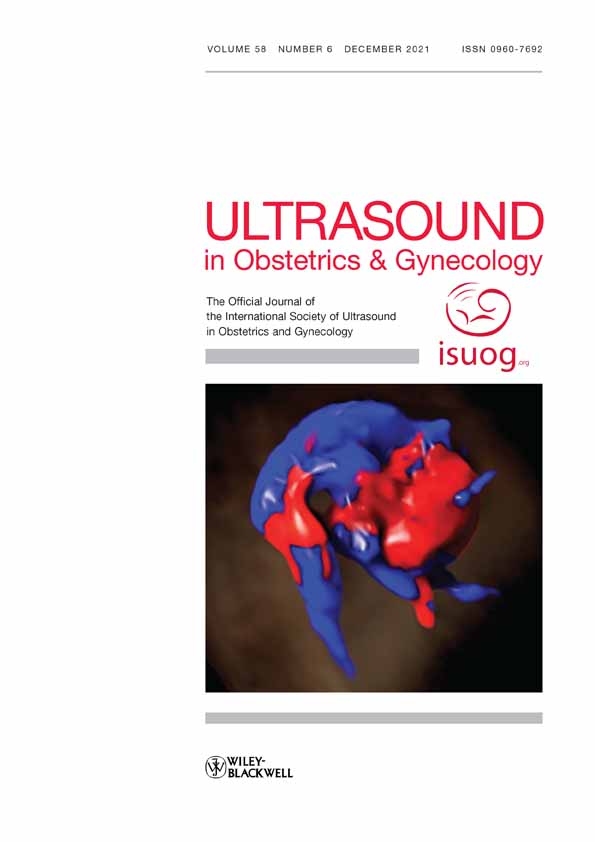
Postmortem examination (a–c) and ultrasound images (d,e) in a 23 + 2-week fetus with urethral atresia. BLA, bladder; L, left; PU, posterior urethra; URE, ureter.
Previous studies have demonstrated a pivotal role of the degree of bladder distension in the diagnostic and prognostic assessment of megacystis and LUTO8-10. However, due to the lack of normative data, bladder distension has not yet been evaluated using an objective, reproducible and gestational-age (GA)-specific method. The aim of this study was to develop and validate the clinical use of nomograms of fetal bladder diameter and volume and derived Z-scores for distinguishing fetuses with PUV from those with other subtypes of LUTO. This would enable tailored antenatal counseling and management in fetuses with congenital LUTO.
METHODS Development of fetal bladder nomogramsThis cross-sectional prospective study was carried out from May 2016 to October 2017 at the University Medical Center Groningen. Pregnant women with a viable singleton uncomplicated pregnancy with confirmed GA were recruited from the 15th week of gestation until 35 weeks' gestation. GA was established based on a dating scan performed between 8 and 11 weeks. Exclusion criteria were: multiple pregnancy, fetal congenital abnormality detected either before or after birth, use of medication, alcohol or drugs, and maternal disease that could potentially affect fetal growth or diuresis (e.g. diabetes mellitus, smoking, hypertensive disorder). Postnatal data were collected in order to exclude neonates with abnormalities or pathological conditions at birth.
A transabdominal ultrasound examination was performed once for each patient by a trained operator (F.F.), using either a Voluson E8 or an E10 system, equipped with a 2–6-MHz RM6C transducer (GE Healthcare, Zipf, Austria). The scan lasted 40 min and serial two- and three-dimensional (2D and 3D) ultrasound images of the fetal urinary bladder were collected.
For measurement of urinary bladder volume (BV), 3D sweeps of the lower fetal abdomen were taken, stored and subsequently analyzed digitally with 4D View software (GE Healthcare). BV was calculated using two methods: automated volume calculation (SonoAVC) and manual Virtual Organ Computer-aided AnaLysis (VOCAL), by tracing the contours of the fluid-filled area with rotational steps of 30°. The longitudinal bladder diameter (LBD) was measured manually in a precise midsagittal plane, by placing one caliper on the inner border of the bladder wall at the upper pole (bladder dome) and the other on the inner border of the lower pole (bladder neck).
For the study design, patient selection and statistical method, the methods of Ioannou et al.11 and Altman and Chitty12 were followed. The measurements were modeled against GA and reference charts were constructed. Polynomial regression models were fitted to the mean and SD of each measurement as functions of GA.
The study was approved by the medical ethics committee in Groningen (dossier number: NL54636.042.15).
Validation of Z-scoresFor clinical validation of the obtained nomograms in a cohort of fetuses with LUTO, cases were collected retrospectively from both The Netherlands (2000–2015) and Mediscan Ultrasound Center in Chennai (2007–2012). The cohort included cases with megacystis referred to one of the eight fetal medicine units (FMUs) in The Netherlands and to Mediscan Ultrasound Center in Chennai. The eight FMUs act as tertiary referral centers for all anomalies suspected in peripheral hospitals in The Netherlands and, similarly, Mediscan Ultrasound Center in Chennai acts as tertiary referral center from the South Asian region for both prenatal diagnosis and fetal therapy.
For each case, the following data were collected: LBD, anteroposterior bladder diameter, transverse bladder diameter, GA at diagnosis and outcome. Ultrasound measurements were either retrieved from the local database or performed on suitable images stored in the database, by a single researcher (F.F.) using the ultrasound machine's built-in measurement tool. The LBD was obtained from a midsagittal view of the fetus, by measuring the distance from the fetal bladder dome to the bladder neck, as was done for creation of the nomograms. BV was calculated using the formula13: LBD × transverse diameter × anteroposterior diameter × π/6.
Final outcome and underlying diagnosis were determined based on the postmortem examination report in cases of termination of pregnancy or perinatal death, and from medical examination or surgery reports for liveborn infants. Cases without an ascertained final diagnosis at postmortem examination or postnatal investigation were not included in this study.
Z-scores were calculated using the formula:  . Predicted LBD was calculated by the formula derived from the fetal nomogram: LBD = 1.48 × GA − 17.15 (Appendix S1).
. Predicted LBD was calculated by the formula derived from the fetal nomogram: LBD = 1.48 × GA − 17.15 (Appendix S1).
The accuracy of the Z-scores was evaluated by receiver-operating-characteristics (ROC)-curve analysis. Antenatal characteristics were compared using the chi-square test or Fisher's exact test for categorical variables and Student's t-test for continuous variables. Data analysis was performed using the statistical software package SPSS Statistics 23 (IBM Corp., Armonk, NY, USA).
RESULTS Development of fetal bladder nomogramsIn total, 225 women with singleton pregnancies at different GAs between 15 and 35 weeks participated in the study (Table S1). BV and LBD were measured at 20-min intervals. In total, 1238 measurements (619 of BV and 619 of LBD) were obtained. BV was measured using both SonoAVC and VOCAL methods.
GA-based reference charts for the fetal urinary bladder were constructed for largest LBD (Table 1), mean LBD (Table 2), largest BV (Table 3) and mean BV (Table 4). A linear relation was observed between LBD and GA (r2 = 0.78 for largest LBD and r2 = 0.76 for mean LBD).
Table 1. Fitted centiles for largest fetal longitudinal bladder diameter (LBD), according to gestational week, between 15 and 35 weeks' gestation Largest LBD (mm) GA (weeks) n 5th centile 50th centile 95th centile SD 15 12 3.99 6.08 8.17 1.27 16 11 5.43 7.79 10.15 1.43 17 13 6.84 9.50 12.16 1.62 18 9 8.21 11.21 14.21 1.83 19 10 9.53 12.92 16.31 2.06 20 15 10.82 14.63 18.44 2.32 21 17 12.06 16.34 20.62 2.60 22 15 13.25 18.05 22.85 2.92 23 19 14.40 19.76 25.12 3.26 24 16 15.49 21.47 27.45 3.64 25 12 16.53 23.18 29.83 4.04 26 13 17.51 24.89 32.27 4.49 27 7 18.44 26.60 34.76 4.96 28 14 19.30 28.31 37.32 5.48 29 9 20.10 30.02 39.94 6.03 30 9 20.84 31.73 42.62 6.62 31 6 21.51 33.44 45.37 7.25 32 5 22.11 35.15 48.19 7.93 33 5 22.64 36.86 51.08 8.64 34 4 23.10 38.57 54.04 9.41 35 4 23.48 40.28 57.08 10.22 Table 2. Fitted centiles for mean fetal longitudinal bladder diameter (LBD), according to exact gestational week, between 15 and 35 weeks' gestation Mean LBD (mm) GA (weeks) n 5th centile 50th centile 95th centile SD 15 12 NC 5.05 11.47 3.90 16 11 NC 6.53 13.32 4.13 17 13 0.85 8.01 15.17 4.36 18 9 1.95 9.49 17.03 4.58 19 10 3.06 10.97 18.88 4.81 20 15 4.17 12.45 20.73 5.03 21 17 5.28 13.93 22.58 5.26 22 15 6.38 15.41 24.44 5.49 23 19 7.49 16.89 26.29 5.71 24 16 8.60 18.37 28.14 5.94 25 12 9.70 19.85 30.00 6.17 26 13 10.81 21.33 31.85 6.39 27 7 11.92 22.81 33.70 6.62 28 14 13.03 24.29 35.55 6.85 29 9 14.13 25.77 37.41 7.07 30 9 15.24 27.25 39.26 7.30 31 6 16.35 28.73 41.11 7.53 32 5 17.46 30.21 42.96 7.75 33 5 18.56 31.69 44.82 7.98 34 4 19.67 33.17 46.67 8.21 35 4 20.78 34.65 48.52 8.43 GA, gestational age; NC, non-calculable. Table 3. Fitted centiles for largest fetal bladder volume (BV), according to exact gestational week, between 15 and 35 weeks' gestation Largest BV (cm3) GA weeks n 5th centile 50th centile 95th centile SD 15 12 NC 0.85 2.10 0.64 16 11 NC 0.69 1.66 0.50 17 13 NC 0.57 1.33 0.39 18 9 NC 0.53 1.13 0.31 19 10 0.03 0.55 1.08 0.27 20 15 0.14 0.67 1.20 0.27 21 17 0.27 0.89 1.52 0.32 22 15 0.41 1.23 2.05 0.42 23 19 0.57 1.70 2.83 0.58 24 16 0.76 2.32 3.87 0.79 25 12 0.98 3.09 5.21 1.08 26 13 1.24 4.05 6.85 1.43 27 7 1.55 5.20 8.84 1.86 28 14 1.91 6.55 11.19 2.37 29 9 2.34 8.14 13.93 2.96 30 9 2.83 9.96 17.09 3.64 31 6 3.40 12.05 20.69 4.41 32 5 4.06 14.41 24.76 5.28 33 5 4.81 17.07 29.32 6.25 34 4 5.67 20.04 34.41 7.33 35 4 6.63 23.34 40.04 8.52 GA, gestational age; NC, non-calculable. Table 4. Fitted centiles for mean fetal bladder volume (BV), according to exact gestational week, between 15 and 35 weeks' gestation Mean BV (cm3) GA (weeks) n 5th centile 50th centile 95th centile SD 15 12 NC 0.69 1.99 0.66 16 11 NC 0.55 1.46 0.46 17 13 NC 0.45 1.06 0.31 18 9 NC 0.39 0.79 0.21 19 10 0.10 0.39 0.68 0.15 20 15 0.18 0.46 0.73 0.14 21 17 0.24 0.60 0.96 0.18 22 15 0.29 0.82 1.36 0.27 23 19 0.34 1.15 1.95 0.41 24 16 0.40 1.58 2.75 0.60 25 12 0.49 2.13 3.77 0.84 26 13 0.62 2.81 5.01 1.12 27 7 0.79 3.64 6.49 1.45 28 14 1.02 4.62 8.22 1.84 29 9 1.33 5.77 10.21 2.27 30 9 1.72 7.10 12.48 2.74 31 6 2.21 8.62 15.04 3.27 32 5 2.81 10.35 17.90 3.85 33 5 3.53 12.30 21.07
留言 (0)