
記住我
Potentially inappropriate medications (PIMs), a type of polypharmacy, are associated with adverse drug events, hospitalization, mortality, and higher health-care costs.1-5 Hence, decreasing the use of PIMs among elderly individuals is an important issue in medical care because they are at a higher risk for adverse drug events as they have reduced physiological function and multiple comorbidities compared with younger populations.3 Nevertheless, elderly patients hospitalized due to acute illness or treated in the intensive care unit (ICU) have higher PIMs after hospitalization.6, 7 In addition, a separate study reported that 65%–87% of elderly patients admitted to tertiary care hospitals are prescribed with PIMs.8, 9 However, to the best of our knowledge, there have been no reports about PIMs at the time of discharge among elderly patients transported to, hospitalized at, and discharged alive from tertiary care hospitals in Japan. We hypothesized that elderly patients are more likely to receive more PIMs during admission at tertiary care hospitals because they have more comorbidities and are more critically ill. Hence, this study compared the proportion of patients aged 75 years or older who received PIMs at admission and discharge and that of patients transferred to tertiary emergency medical institutions. Moreover, the characteristics of PIMs at discharge and their associated factors were investigated.
Methods Ethics statementThis study was approved by the research ethics committee of Tokyo Medical University (approval no. T2020-0377) and was carried out in accordance with the Declaration of Helsinki. Only data from medical records were used, and there was no contact with the patients. Hence, the need for informed consent was waived by the research ethics committee of Tokyo Medical University.
Study design, setting, and participantsThis was a retrospective observational study undertaken at Tokyo Medical University Hospital, a 904-bed tertiary institution in Shinjuku-ku, Tokyo, Japan, from August 2018 to September 2019. Patients are admitted at the hospital’s emergency intensive care unit (EICU) or at the general ward. In the EICU, patients receive intensive care. If they no longer require intensive care, they are transferred to the general ward. Emergency physicians oversee the entire process from the initial treatment to intensive care to the management in the general ward.
The study included elderly patients who were admitted to our tertiary care emergency medical institution. The Japan Geriatric Society and the Japan Gerontological Society, as well as the Japanese guidelines for medications, define elderly as individuals aged 75 years or older.10, 11 Thus, only patients aged 75 years or older were included in the analysis. We excluded patients who died in the emergency room (ER) and during hospitalization, those transferred directly from our ER to another hospital, those hospitalized at our department for less than 24 h, and those with unknown medications.
Data collection and patient characteristicsData including age, sex, primary diagnosis at admission, social and medical history, and medication use were collected from the electronic medical records of Tokyo Medical University Hospital. Information about medication use at the time of admission at our hospital was based on prescriptions and referral letters issued by the attending physician at the outpatient department of the referring medical institution. The attending physician at the referring institution was responsible for medication management during hospitalization and for determining and documenting the prescriptions at discharge. Medication information at the time of discharge was based on the prescription at discharge issued by the attending physician at our institution. The discharge prescriptions included all regular oral, inhalant, and injectable medications used at discharge. Moreover, medications given on an as-needed basis for chronic diseases were included in the discharge prescriptions. Potentially inappropriate medications were identified using the Screening Tool of Older Persons’ Potentially Inappropriate Prescription (STOPP) criteria version 2.12
Prescriptions in the EICUAt the EICU, emergency physicians, nurses, and pharmacists assessed the medications of each patient on admission and documented any medication duplication or the prescription of medications with a high risk of side-effects. Moreover, they evaluated whether a patient’s medication was discontinued or continued or whether a new prescription was provided after hospitalization. Next, a dedicated pharmacist immediately reviewed the prescription and directly consulted with the prescribing physician if required. We considered the risks and benefits of modifying each medication per case.
In addition, oral medications were given through a gastric tube in patients who could not tolerate them due to impaired consciousness or swallowing.
OutcomesThe primary outcomes were the proportion of elderly patients taking at least one PIM at admission and at discharge. The number of PIMs according to drug type and factors associated with PIMs at discharge were investigated.
Statistical analysisA nonparametric test (Mann–Whitney’s U-test) and multivariate analysis using the logistic regression model were used to examine the association between the use of PIMs at hospital discharge and selected variables. With reference to previous studies,13-15 the following variables were entered in the nonparametric test and multivariate analysis: age, sex, total number of medications at admission, number of PIMs at admission, length of hospital stay, Acute Physiology and Chronic Health Evaluation (APACHE) II score, total number of medications at discharge, and Charlson Comorbidity Index. Analyses were undertaken using SPSS software (version 24; IBM), and a p-value of less than 0.05 was considered statistically significant.
Results Patient selectionDuring the study period, 704 patients aged 75 years or older were transferred to the ER of our hospital. In total, 440 patients were excluded from the study due to the following reasons: less than 24 h of hospital stay (from ER to hospitalization) (n = 230), death at the outpatient department (n = 132), in-hospital death (n = 52), and without medication data (n = 26). Hence, only 264 patients were included in the final analysis (Figure 1).

Flowchart of patient inclusion in this study of potentially inappropriate medications at discharge among elderly patients at a single tertiary emergency medical institution in Japan
Patient characteristicsTable 1 depicts the baseline characteristics of patients. Their mean age was 84 years (standard deviation [SD], 5.7), and 169 (64%) were men. The mean Charlson Comorbidity Index was 3.1 (SD, 1.3), and the mean APACHE II score was 19 (SD, 6.7). The primary diagnoses were exogenous (n = 24; 9.1%) and endogenous (n = 240; 91%). Heart failure was the most common endogenous disease (n = 46; 17%).
Table 1. Demographic and clinical characteristics of study participants at baseline Variable (n = 264) Age at enrollment, years 84 ± 5.7 Men 169 (64) Charlson Comorbidity Index at enrollment 3.1 ± 1.3 APACHE II score 19 ± 6.7 Admission diagnosis Endogenous disease 240 (91) Heart failure 46 (17) Ischemic stroke 34 (13) Pneumonia 27 (10) ACS 13 (5) Septic shock 12 (5) Postcardiac arrest syndrome 10 (4) Exogenous disease 24 (9) Length of hospital stay, days 26 ± 27.5 Length of EICU stay, days 7 ± 8.3 Use of ventilator 107 (40.5) Duration of ventilation treatment, days 3.8 ± 10Medical cost, ¥
Medical cost, $†
2,187,663 ± 2,254,961
19,888 ± 20,500
Discharge disposition Home 121 (46) Rehabilitation hospital 21 (8) Other acute care hospital 121 (46) Nursing home 1 (0.4) Note: Data are presented as mean ± standard deviation or n (%). Abbreviations: ACS, acute coronary syndrome; APACHE II, Acute Physiology and Chronic Health Evaluation II; EICU, emergency intensive care unit. † $1 = ¥110. Proportions of patients with PIMs at admission and dischargeTo determine how PIMs use changed during hospitalization, we compared the proportion of patients taking PIMs at admission and those taking PIMs at discharge. In total, 175 (55%) and 74 (28%) patients had PIMs prescribed at admission and discharge, respectively. Thus, the proportion of patients taking PIMs decreased during hospitalization at our facility.
Potentially inappropriate medications prescribed at admission and dischargeTable 2 shows the individual PIMs at admission and discharge according to drug subcategory. At admission, benzodiazepines were the most frequently prescribed PIMs, followed by proton pump inhibitors (PPIs) and nonsteroidal anti-inflammatory drugs. At discharge, PPIs were the most common PIMs, followed by benzodiazepines and antipsychotics. These three categories accounted for 69% of all PIMs at discharge. We compared PIMs at admission and discharge. Results showed that the number of PPI prescriptions only increased at discharge, and the rest of the PIMs decreased at admission.
Table 2. Number of potentially inappropriate medications (PIMs) at admission and at discharge of elderly patients at a single tertiary emergency medical institution in Japan, by type of drug At admission At discharge Total, n 244 78 Benzodiazepines 41 (16.8) 13 (16.6) Proton pump inhibitors 31 (12) 32 (41) NSAIDs 24 (9.8) 2 (2.5) Laxative 23 (9.4) 0 (0.0) Mucosal protective drugs 17 (6.9) 0 (0.0) Vitamin preparations 13 (5.3) 0 (0.0) Antiplatelet 12 (4.9) 0 (0.0) Antihistamines 12 (4.9) 3 (3.8) Hypnotics (nonbenzodiazepines) 11 (4.5) 5 (6.4) Antipsychotics 10 (4.1) 9 (11.5) Note: Data are shown as n (%), unless otherwise noted. PIMs were defined based on the Screening Tool of Older Persons’ Potentially Inappropriate Prescription (STOPP) criteria version 2. Abbreviation: NSAID, nonsteroidal anti-inflammatory drug. Predictors of PIMs at dischargeIn the nonparametric test (Mann–Whitney U-test), longer length of hospital stay and higher number of medications at discharge was directly related to a patient taking at least one PIM at discharge (Table 3).
Table 3. The nonparametric test results of PIMs at discharge Patient/institutional variables All patients PIMs† group Non PIMs† group P-valuesAge‡
Median (IQR)
84 (78–88) 86 (79–88) 83 (78–88) 0.055Sex‡
Female/male (n)
95/169 35/30 60/139 0.267No. of medications at admission‡
Median (IQR)
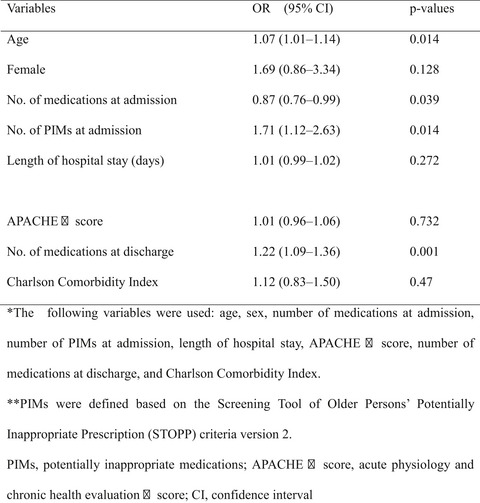
6 (4–9) 6 (4–9) 6 (3–9) 0.6 No. of PIMs† at admission‡ Median (IQR) 1 (0–1) 1 (0–1) 1 (0–1) 0.131 Length of hospital stay(days)‡ Median (IQR) 19 (2–192) 26 (2–128) 16 (2–192) 0.001 APACHE Ⅱ score‡ Median (IQR) 18 (14–23) 18 (14–23) 19 (14–24) 0.846 No. of medications at discharge‡ Median (IQR) 2 (0–18) 7 (2–14) 4 (0–18) <0.01 Charlson Comorbidity index‡ Median (IQR) 1 (0.5–2) 1 (1–2) 1 (0–2) 0.131 APACHE Ⅱ score, acute physiology and chronic health evaluation Ⅱ score; PIMs, potentially inappropriate medications. † PIMs were defined based on screening tool of older persons’ potentially inappropriate prescription (STOPP) criteria version 2. ‡ The following variables were used: age, sex, number of medications at admission, number of PIMs at admission, length of hospital days, APACHE Ⅱ score, number of medications at discharge, and Charlson Comorbidity Index.In the multivariate analysis using the logistic regression model, older age, greater number of PIMs at admission, and greater number of medications at discharge were independently associated with a higher risk of using PIMs at discharge (Table 4). In addition, patients with a higher total number of medications at admission had a lower association with PIMs at discharge (Table 4). No other indicators were statistically significant predictors of PIMs use at discharge.
Table 4. Multivariate analysis using logistic regression model results of PIMs at discharge Variables OR (95% CI) P-values Age‡ 1.07 (1.01–1.14) 0.014 Female‡ 1.69 (0.86–3.34) 0.128 No. of medications at admission‡ 0.87 (0.76–0.99) 0.039 No. of PIMs† at admission‡ 1.71 (1.12–2.63) 0.014 Length of hospital stay (days)‡ 1.01 (0.99–1.02) 0.272 APACHE Ⅱ score‡ 1.01 (0.96–1.06) 0.732 No. of medications at discharge‡ 1.22 (1.09–1.36) 0.001 Charlson Comorbidity Index‡ 1.12 (0.83–1.50) 0.47 APACHE Ⅱ score, acute physiology and chronic health evaluation Ⅱ score; CI, confidence interval; PIMs, potentially inappropriate medications. † PIMs were defined based on the Screening Tool of Older Persons’ Potentially Inappropriate Prescription (STOPP) criteria version 2. ‡ The following variables were used: age, sex, number of medications at admission, number of PIMs at admission, length of hospital stay, APACHE Ⅱ score, number of medications at discharge, and Charlson Comorbidity Index. DiscussionTo the best of our knowledge, this study is the first to assess the prescription of PIMs at discharge using the STOPP criteria in elderly patients discharged from a tertiary emergency medical institution in Japan.
The number of PIMs increased at discharge in elderly patients hospitalized due to acute illnesses and in patients treated and discharged from the ICU. Moreover, 85% of patients are discharged from the ICU with at least one PIM.6, 7 However, in our study, the proportion of patients taking PIMs decreased from 55% at admission to 28% at discharge. This result might be attributed to the fact that the multidisciplinary approach used in the EICU, as described in the Materials and Methods section, has incidentally reduced the number of PIMs. Furthermore, the timely rehabilitation provided by occupational and physical therapists and appropriate nutritional guidance by nutritionists might have prevented the administration of additional unnecessary drugs.
Potentially inappropriate medications are usually reduced after admission to a geriatric care unit, treatment by a geriatric specialist, as well as daily collaboration between a senior geriatrician and psychiatrist who is part of the geriatric interdisciplinary care team.16, 17 However, in our EICU, there is no geriatric specialist, and emergency physicians and intensivists are in charge of the treatment. Hence, emergency physicians and intensivists, who are not geriatric medicine specialists, can correct the prescription of PIMs in elderly patients who are critically ill by providing interventions based on the patient’s background and by collaborating with other professionals.
The use of most PIMs decreased at discharge compared with at admission. However, the prescription of PPIs increased. For the past four decades, the use of PPIs as a prophylaxis for upper gastrointestinal bleeding or stress ulcer has been considered essential among critically ill hospitalized patients. Moreover, it is used in the standard of care among patients admitted at the ICU.18 In recent years, there have been reports about the adverse events of PPIs.19-23 In the EICU of our hospital, physicians and pharmacists collaborate during daily patient rounds to evaluate for risk factors associated with stress ulcers. Moreover, they decide whether to continue or discontinue treatments. However, this assessment is not undertaken after the patients are transferred to the general ward. Thus, treatment with PPIs is continued indiscriminately after discharge from the EICU. In several cases, the use of PPIs is not required after ICU discharge. Therefore, the risk factors for stress ulcers must be assessed, and the prescribed medication should be modified at the time of ICU discharge and after discharge. Not only the use of PPIs but also the integration of medication adequacy assessment in the process of discharging patients from the ICU should be considered. Thus, medical professionals must cautiously evaluate for the inappropriate prescription of PPIs in patients discharged from tertiary care institutions.
In addition, hypnotics (benzodiazepines + nonbenzodiazepines) accounted for 23% of all PIMs at discharge. Hypnotics are associated with the risk of falls and fractures, and all benzodiazepines should be avoided according to the STOPP and Beers criteria.12, 24 The use of hypnotics (benzodiazepines + nonbenzodiazepines) at discharge (n = 18) compared with at admission (n = 52) decreased. However, it should still be further reduced. Hypnotics cannot be abruptly discontinued because this disrupts the sleep patterns of patients. Hence, physicians should prescribe nonpharmacological sleep therapy, rather than new benzodiazepines. To modify treatment for chronic insomnia, the number of prescriptions should be limited through a society-wide effort by educating patients and the general public about the risks of the long-term use of benzodiazepines.
In this study, older patients with a higher number of medications at discharge were at a higher risk of using PIMs at discharge. This finding is consistent with that of a study undertaken in a primary care setting.13-15 Even among patients who were transferred to a tertiary care hospital and discharged, clinicians ought to consider PIMs if the number of prescriptions at discharge is high. Nevertheless, previous studies have reported no association between age at admission and use of any PIMs at discharge.25, 26 Moreover, in this study, patients with a higher total number of medications at admission were less likely to have PIMs at discharge. This result might be attributed to the small sample size, which is one of the limitations of this study. Other possible factors could be that patients with a higher total number of medications at admission had more comorbidities and needed more appropriate medications, which could have led to fewer inappropriate prescriptions. Therefore, further studies must be undertaken to assess the impact of factors on PIMs use at discharge in elderly patients who are critically, acutely ill.
The current study had several limitations. First, the research was retrospective in nature and had a small sample size. Hence, bias might have existed. Second, the rate of PIMs use after discharge was not assessed. Therefore, whether the reduced use of PIMs, as observed in our study, is sustainable in the long term and whether it can improve outcomes in clinically important patients remain unclear. Hence, the study results should be interpreted with caution, and further studies must be confirmed.
ConclusionsTransfer to tertiary care hospitals can improve the quality of medication use in elderly patients. However, PIMs are still prescribed at discharge. Thus, caution must be observed while prescribing these medications to older patients with a higher number of PIMs at admission and a higher number of medications at discharge.
AcknowledgmentsThe authors want to thank Miyuki Moriwaki for helping in the collection of patient data from the database.
DisclosureApproval of the research protocol: This study was approved by the medical ethics committee of the institution (no. T2020-0377). It was carried out in accordance with the Ethical Guidelines for Epidemiological Research in Japan.
Informed consent: The need for individual informed consent was waived as this was a retrospective analysis of data collected prospectively for routine care and there was no breach of privacy or anonymity.
Conflict of interest: None.
留言 (0)