Referral Patterns of Central Retinal Artery Occlusion to an Academic Center Affiliated With a Stroke Center
Background:
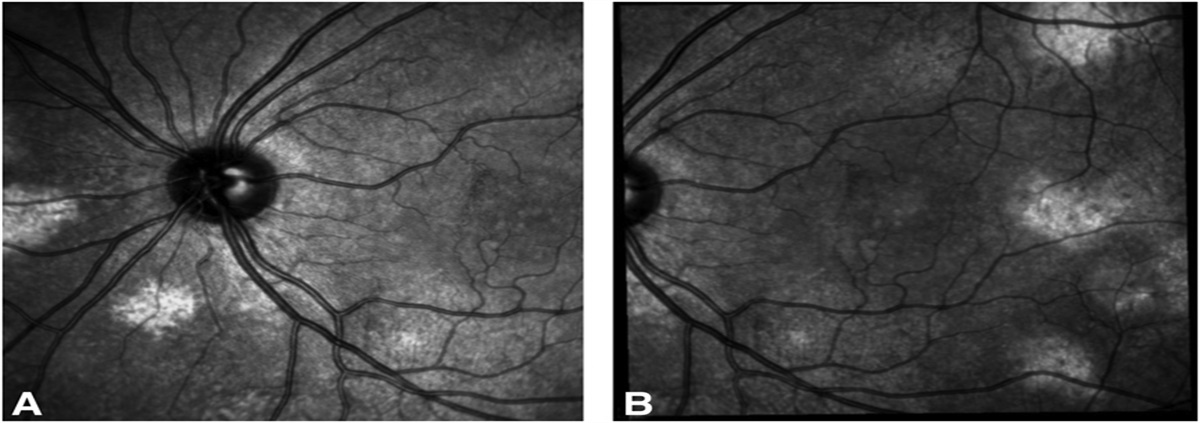
Central retinal artery occlusion (CRAO) is a medical emergency, and patients who present acutely should be immediately referred to the nearest stroke center. We evaluated practice patterns for CRAO management at one academic center over the last decade.
Methods:
This was a retrospective study on all adult patients diagnosed with a CRAO seen at one tertiary hospital and outpatient clinic affiliated with a comprehensive stroke center (“our institution”) from 2010 to 2020. Our electronic medical records were searched for CRAO diagnoses, and patient medical records were reviewed. The exclusion criteria were incorrect diagnosis, unclear diagnosis, historical CRAO, or satellite clinic location. Demographics, distance and time to presentation to our institution, number and type of prior providers seen, diagnostic tests performed, and treatments provided were collected. Summary statistics of median, mean, and frequency were calculated and reported with measures of variance (interquartile range [IQR], ranges). F, Tukey, and Fisher exact tests were used for comparisons.
Results:
We included 181 patients with a diagnosis of CRAO (80 [44.2%] women; median age 69 years [range 20–101]). The median distance from patient's home to our institution was 27.8 miles (IQR 15.5–57.4; range 2.4–930). The median time from visual loss to presentation at our institution was 144 hours (IQR 23–442 hours, range 0.5–2,920) from 2010 to 2013, 72 hours (IQR 10.5–372 hours, range 0–13,140) from 2014 to 2016, and 48 hours (IQR 7–180 hours, range 0–8,030) from 2017 to 2020 (P = 0.07). 91/181 (50%) patients presented to an outpatient provider. 73/181 (40%) presented to an emergency department. Eighty-six percent presented within 1 week of visual loss onset, and rates of comprehensive inpatient evaluation for acute CRAO improved from 44% in 2010–2013 to 82% in 2017–2020 (P < 0.01).
Conclusions:
Patients with CRAO often present late and only after evaluation by multiple outpatient providers. Improvement has occurred over the past decade, but delays underscore the barriers to performing clinical trials evaluating very acute treatments for CRAO. Educational interventions for healthcare providers and patients are necessary.


留言 (0)