
記住我


An elderly man was involved in a motor vehicle collision in which he sustained fatal blunt force injuries. A complete autopsy was performed. The decedent had a complex past medical history that included chronic obstructive pulmonary disease and coronary artery disease status-post three-vessel coronary artery bypass grafting. He also had a history of cognitive impairment following an undisclosed incident approximately 30 years prior to death. Magnetic resonance imaging of the brain performed approximately 20 years before death showed bilateral pallidal lesions (Box ).
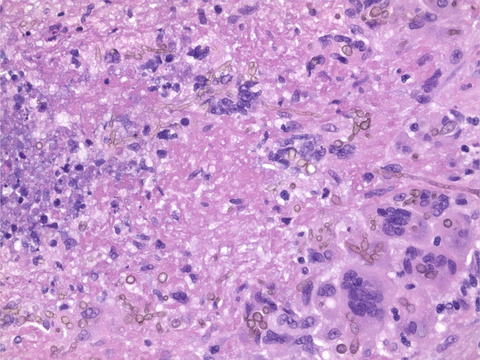
2 FINDINGSThe autopsy examination revealed extensive blunt force injuries of the head, torso, and extremities. Natural diseases identified at autopsy included severe atherosclerotic and hypertensive cardiovascular disease, a remote myocardial infarct, emphysema, and severe hepatic steatosis. Examination of the brain revealed traumatic pontomedullary avulsion, mild diffuse white matter atrophy, and bilateral, symmetric, 0.2–0.3 cm, yellow-brown cavitary lesions in the globus pallidus (Figure 1A,B). Microscopic examination of the globus pallidus confirmed the presence of cavitation with traversing glial fiber bundles. Perilesional gliosis was exuberant and highlighted by vimentin immunostaining with diffuse, mild reactive astrocytosis scattered throughout the entire basal ganglia and internal capsule (Figure 2A,B). Vimentin immunostaining of the frontoparietal lobe also showed diffuse reactive astrocytosis with the white matter more severely affected than the gray matter. Luxol fast blue and H&E staining of the frontoparietal lobe revealed patchy demyelination in the white matter. What is your diagnosis?

Coronal sections of the brain demonstrated bilateral symmetric cavitary lesions in the globus pallidus (A and B)

Microscopic examination showed cavitary lesions with perilesional gliosis (A, H&E, x200, and B, vimentin immunohistochemistry, x400)
3 FINAL DIAGNOSISRemote carbon monoxide poisoning.
4 DISCUSSIONThe differential diagnosis for cavitary lesions in the basal ganglia includes hypertensive lacunar infarcts, methanol poisoning, and carbon monoxide poisoning. Whereas methanol poisoning classically affects the putamen, carbon monoxide classically affects the globus pallidus.
Carbon monoxide is a colorless and odorless toxic gas produced from the incomplete combustion of carbon-containing compounds. It disrupts cellular metabolism and competitively binds hemoglobin, resulting in decreased oxygen-carrying capacity of blood, cellular injury, and tissue hypoxia [1-3]. Common mechanisms of carbon monoxide poisoning include accidental smoke or engine exhaust inhalation and furnace malfunctions; carbon monoxide inhalation may also be intentional. Approximately 50,000 cases of accidental carbon monoxide poisoning are estimated to occur in the United States annually, of which less than 5% are fatal [1, 3]. In this case, it was discovered that the decedent's incident 30 years prior to death involved a chimney obstruction that resulted in carbon monoxide inhalation and poisoning.
Neuropathologic examination in cases of carbon monoxide poisoning may reveal infarction of the globus pallidus. The mechanisms underlying preferential involvement of the pallidal nuclei in carbon monoxide poisoning are poorly understood but have been hypothesized to involve vascular distribution, metabolic activity, immunologic responses, and the iron content of the globus pallidus. Additional findings in carbon monoxide poisoning may include necrosis of the putamen and thalamus, diffuse brain atrophy, and white matter demyelination [2].
Neurologic sequelae of carbon monoxide poisoning are highly variable and may develop in a delayed fashion. Such sequelae may include memory and concentration deficits, psychiatric conditions including depression and anxiety, personality changes, and motor dysfunction including Parkinsonism [1, 3].
5 CONCLUSIONCarbon monoxide disrupts cellular metabolism, competitively binds hemoglobin and causes tissue hypoxia. We presented an interesting case of an elderly man with a remote history of accidental carbon monoxide poisoning who died of multiple blunt force injuries sustained in a motor vehicle crash. Neuropathologic examination revealed bilateral globus pallidus cavitary infarcts, which is a classic finding in remote carbon monoxide poisoning. Differential considerations include lacunar infarcts because of hypertension, and methanol poisoning.
CONFLICT OF INTERESTThe authors have no conflicts of interest to declare.
AUTHOR CONTRIBUTIONSTracy Halvorson wrote the manuscript. Stephanie Stauffer and Karra Jones reviewed and edited the manuscript.
Data sharing is not applicable to this article as no new data were created or analyzed in this study.
REFERENCES
1Chiew AL, Buckley NA. Carbon monoxide poisoning in the 21st century. Crit Care. 2014; 18(2): 221– 8. 2Lo CP, Chen SY, Lee KW, Chen WL, Chen CY, Hsueh CJ, et al. Brain injury after acute carbon monoxide poisoning: early and late complications. Am J Roentgenol. 2007; 189(4): W205– 11. 3Rose JJ, Wang L, Xu Q, McTiernan CF, Shiva S, Tejero J, et al. Carbon monoxide poisoning: pathogenesis, management, and future directions of therapy. Am J Respir Crit Care Med. 2017; 195(5): 596– 606.
留言 (0)