As mentioned, this study was conducted to evaluate morphological changes in retinal anatomy as assessed by OCT or in retinal cell function as assessed by various forms of ERG as well as its correlation with BM. They are procedures widely used in human clinics and data from these two methods constitute an important contribution to resolve controversies in retinal participation in this intoxication.
Mercury vapor is a significant source of mercuric load in occupational exposure because it is odorless and colorless and tends to accumulate in poorly ventilated areas. Once the lungs have absorbed the inhaled vapor, the mercury can reach different tissues via the bloodstream, with the primary target of the CNS and the eye [2, 31]. When it is oxidized, it cannot penetrate the blood-barrier again and remains for prolonged periods of time in tissues [2, 6, 7, 15, 31].
As mentioned, the neurologic and thus the visual pathway effects resulting from mercury toxicity have been described widely [2, 31, 32]. The long-term exposure neurological effects can include symptoms from tremor, neuropathy, personality changes referred to as mercurial erethism, speech disruption, delirium, or rigidity to symptoms of VF defects, reduced VA, color and night vision disfunction, or decreased CS [2, 7, 31, 33]. However, after the introduction of electrophysiology there is a strong suspicion that the retina may also be primarily affected and that not all alterations of the visual pathway are due to CNS poisoning [16].
As previously mentioned, in this event the first patients’ complaints were attributed to a viral infection, which delayed the diagnosis and analytical determinations. At the time of correct diagnosis, the mercuric values in urine (mean, 302.86 μg/g Cr) and blood (mean, 392.93 μg/L) significantly exceeded the maximal accepted level for occupational exposure (< 30 μg/g Cr and 10 μg/L, respectively) [17, 18]. In such cases, the mainstay of treatment is chelation therapy; however, only three patients underwent early chelation, which was stopped prematurely because of severe adverse reactions. Fifteen workers underwent delayed chelation (8 to 12 months after the initial incident). However, this late chelation did not result in significant symptom relief.
Twenty-six workers exhibited symptoms related to erethism. Some, also showed symptoms associated with cognitive mercury poisoning such as memory and attention disturbances [31, 32]. Tremor of the hands, head, and eyelids, a late symptom of mercury poisoning, also occurred in some patients. EMG showed signs of mixed sensorimotor polyneuropathy and multiple mono-neuropathy alterations 12 to 18 months after exposure.
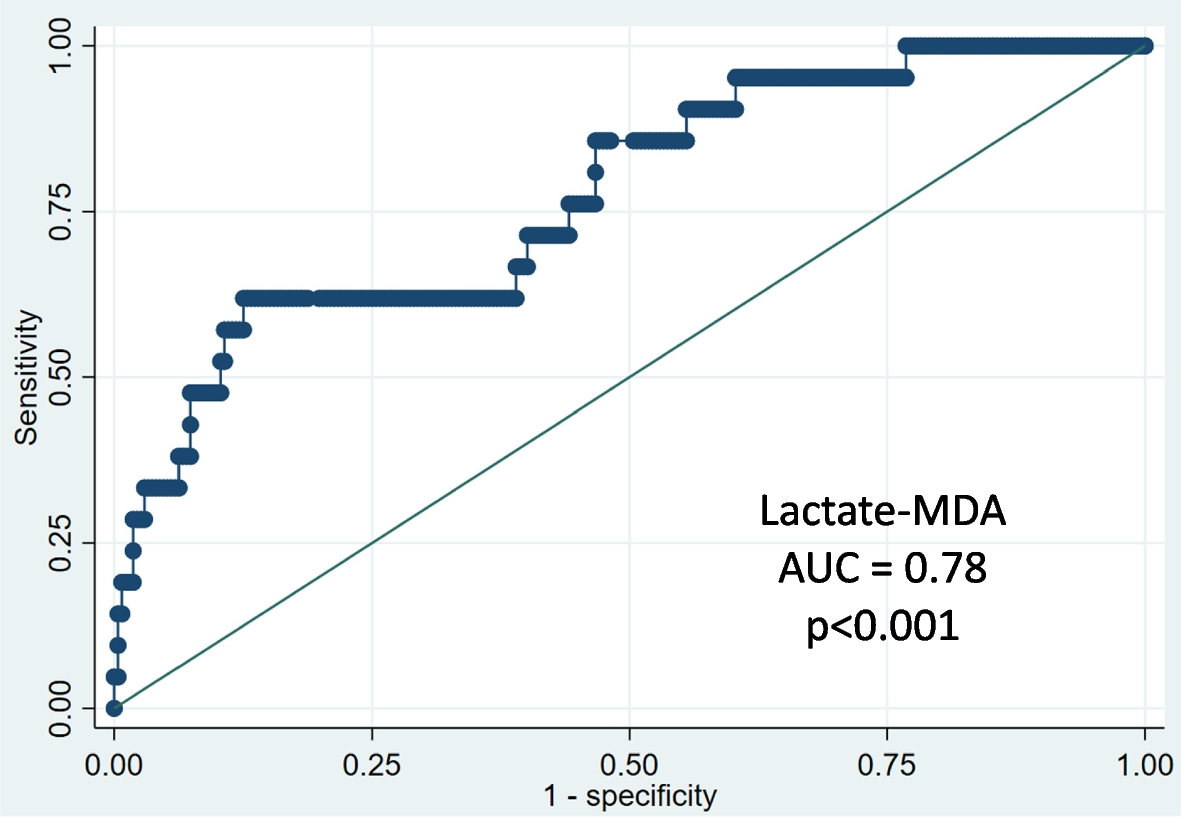
In this series, the VA slightly decreased in fourteen patients; however, advanced visual functions were impaired apparently in an independent way from mercury levels since significant negative correlations were detected only among the BML, BCVA, and ffERG. There was no correlation between BML and ocular findings in agreement with previous similar studies [7, 34, 35]. It is also reported that findings from one eye cannot be similar to the fellow one, so it is highly recommended to evaluate both eyes separately, as we did.
Color vision and CS impairment at high spatial frequencies also were found, being the most frequently observed color vision alteration in the blue-yellow axis. It is well known that the results of the CS measurement are very unspecific, although they are very sensitive. These findings are in agreement with previous studies [33, 36,37,38].
The most prevalent VF defect pattern was concentric constriction (17 eyes, 29.3%), in agreement with previous studies [39, 40]. This visual impairment may have a central origin (calcarine cortex), as it has been reported previously [41]. In addition, the increased implicit time of P100 in the affected patients, especially in those of Group 1, indicates delayed nerve conduction and involvement of the visual pathway. Group 1 was constituted by a subgroup of patients with evident visual disturbances in their VF test, therefore patients with most severe visual alterations. Consequently, Group 1 showed lower amplitudes and lengthened latencies in PRVER than all patients together as expected. In 2008 da Costa et al. had already reported this finding These results were consistent with the findings obtained in previous publications (27, 39). But data of current series demonstrated a significant retinal involvement showing retinal dysfunction in the ffERG, PERG, and mfERG tests, with both a generalized retinal response loss and a clear alteration of the central retinal area, which could have influenced the results obtained in the VF.
The ffERG showed changes in SRR (the scotopic responses), suggesting that rod cells were impaired in the mercury-vapor intoxicated patients, as well as in OP, suggesting additional involvement of the inner retina.
Besides, results in photopic ffERG responses and the lower amplitude of P50 in PERG found in Group 1, suggest that cones and ganglion macular cells can also be affected in mercury intoxication. These findings harmonize with the psychophysical color-vision losses reported here and in other previous studies and with spatial and temporal luminance contrast-sensitivity losses (16).
Moreover, it is known that ffERG could not be a useful tool for detecting small retinal lesions [42, 43], but the mfERG does and its results add further evidence of damage to the photoreceptors since the amplitudes of the P1 wave showed loss of the retinal response within the central 50 degrees, as reported previously [16]. All these findings reinforce the idea that both the outer and inner retina visual processes are both involved in visual mercury toxicity.
A discrepancy was observed between the dysfunction patterns observed in the VF and the mfERG, with less involvement in the electrophysiological test. This finding also would confirm a visual pathway damage (detected by the mfERG) in addition to that in the retina. Besides, although the PRPEV measurements do not correlate with the BML, patients in group 1 had latencies significantly over 100 milliseconds and significantly reduced P100 amplitudes. Though these results typically occur in optic neuropathies and visual cortex abnormalities, they also can be associated with maculopathies, especially when they are interpreted in conjunction with other retinal function tests (PERG, mfERG, and ffERG). Findings in PRPVE are in agreement with those reported by Ventura et al. and da Costa et al. [16, 27].
Despite the functional retinal involvement and in contrast to the results obtained by Ekinci et al. [6, 15], OCT did not reveal structural changes in the RNFL, macular CRT, and choroid thickness [25, 26]. These differences might be related to the intensity and the manner of poisoning, as the current patients reached higher levels of mercury in a short period of time compared to the long exposure times of workers examined by Ekinci et al. [6, 15].
Current study has several limitations. There were no environmental measurements of mercury either before the accident or during the occupational event. In addition, probably only the most affected patients were evaluated at the IOBA-Eye Institute, and the time that elapsed after the acute accident and the assessment likely was not the most appropriate for adequate follow-up over time. Most of the identified visual alterations seem attributable to the occupational exposure to mercury vapor, but we have not objective information on the ophthalmologic status before the accident. In addition, because a programmed follow-up was not possible, we had no information about the current clinical situation or about the evolution of most patients. Regarding the electrophysiologic tests, most of the patients were minimally affected and the number of patients with significant ophthalmological signs (group 1) was small, thus caution should be taken when interpreting these findings. Finally, the OCT technology has evolved so rapidly that it is possible that with new OCTs based on swept source or ultra-high resolution it would have been possible to detect changes in the retinal or choroidal structures.
Even so, this study presents some relevant findings from a very rare and extremely serious event, for which references are scarce. There was no correlation between BML and ophthalmologic examination findings. As mentioned before, the VA in those patients is slightly affected and there is more VF involvement. The most prevalent VF alteration was diffuse decreased sensibility, but central involvement also was found. This finding could be of retinal and/or neurologic origin considering the mfERG results.
In summary, despite its limitations, this series of patients affected by the same event contributes to the information obtained about mercury poisoning for future similar situations and reinforces the idea of a retinal alteration in addition to CNS damage.





留言 (0)